A rare variant of lichen planopilaris: Familial Graham-Little-Piccardi-Lassueur syndrome in Saudi Arabia
Sadeen T. Shahbar, Hadeel A. Maaddawi, Yara E. Aljefri, Nawal R. Al Yamani, Zainab A. Khalaf, Mostafa A. Safar

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
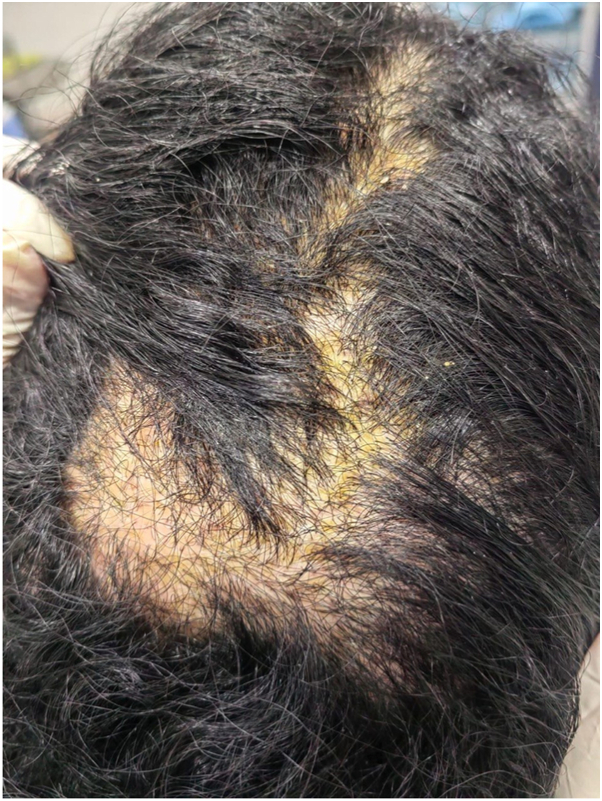 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3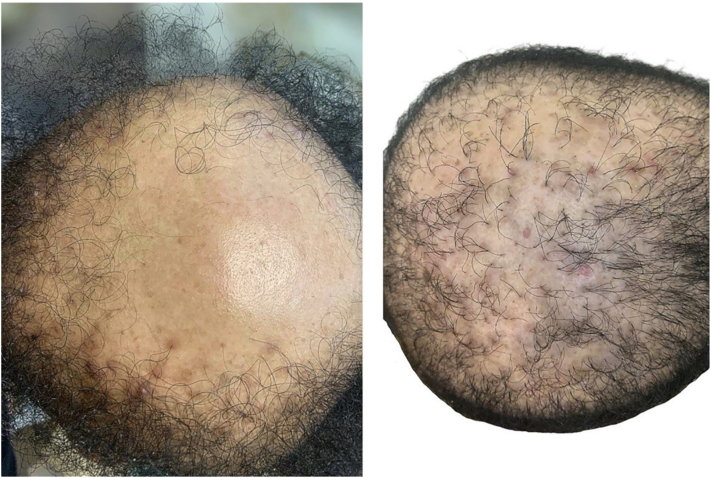 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood disorders and treatments · Autoimmune and Inflammatory Disorders · Genetic factors in colorectal cancer
Case description
A 28-year-old woman from Jeddah, Saudi Arabia, presented with a 1-year history of progressive scalp hair loss associated with pruritus and scalp tenderness. Hair loss initially involved the parietal region and gradually progressed to affect the entire scalp. She additionally reported a 14-year history of widespread follicular papules, first noted on the upper extremities and later involving the trunk and lower limbs. Cutaneous examination revealed patchy cicatricial alopecia of the scalp with associated hyperpigmented, keratotic follicular papules distributed over the scalp, trunk, and extremities (Figs 1 and 2). The eyebrows, axillae, and pubic regions were spared. Trichoscopic evaluation demonstrated perifollicular erythema, scaling, and absence of follicular openings, findings consistent with lichen planopilaris (LPP) (Fig 3). Scalp biopsy showed nonspecific features of cicatricial alopecia and was performed primarily to exclude histologic mimickers rather than to confirm the diagnosis.Fig 1. Patchy areas of cicatricial alopecia involving the parietal scalp, demonstrating perifollicular scale and erythema, and loss of follicular ostia, consistent with LPP.Fig 2. Diffuse follicular keratotic papules involving the upper back of the index female patient, consistent with the extracephalic cutaneous manifestations of Graham-Little-Piccardi-Lassueur syndrome.Fig 3. Dermoscopy findings suggestive of the trichoscopic features of lichen planopilaris with perifollicular scaling and erythema and absent follicular openings.
Family history was significant for similar cutaneous and scalp findings in her father and 2 brothers, all of whom developed follicular papules followed by patterned scalp alopecia during adolescence or early adulthood, supporting a familial form of disease (Fig 4). One affected brother failed to respond to hydroxychloroquine therapy, while the other remained untreated.Fig 4. Scalp involvement in affected siblings demonstrating alopecia with a similar distribution pattern, supporting a familial presentation.
The patient was treated with oral isotretinoin (20 mg daily for 6 months), resulting in approximately 80% improvement of follicular papules. Hydroxychloroquine (200 mg daily for 2 years) led to stabilization of hair loss without regrowth. Intralesional corticosteroids provided symptomatic relief but did not induce hair regrowth, and a 6-month trial of dutasteride (0.5 mg daily) yielded no clinical benefit.
Question: A 28-year-old woman presents with progressive scarring alopecia of the scalp associated with pruritus and pain. She has a long-standing history of widespread follicular papules on the trunk and extremities. Trichoscopy reveals perifollicular erythema, scaling, and absent follicular openings. Family history is notable for similar findings in her father and 2 brothers. Which of the following is the most likely diagnosis?
- **A.**Graham-Little-Piccardi-Lassueur syndrome
- **B.**Classic lichen planopilaris
- **C.**Folliculotropic mycosis fungoides
- **D.**Familial keratosis pilaris with coincidental alopecia
- **E.**Central centrifugal cicatricial alopecia
Correct Answer: A. Graham-Little-Piccardi-Lassueur syndrome.
Answer discussion
This presentation is most consistent with Graham-Little-Piccardi-Lassueur syndrome (GLPLS), a rare variant of lichen planopilaris characterized by the triad of cicatricial scalp alopecia, widespread follicular keratotic papules, and variable non-scarring alopecia at other sites. The latter feature, commonly involving the axillary or pubic regions, may be absent or delayed, particularly early in the disease course.1 The prominent extracephalic follicular papules and strong familial clustering favor GLPLS over classic lichen planopilaris, which typically lacks these features. Familial cases of GLPLS have been reported and suggest an underlying genetic predisposition.2, 3, 4, 5 Folliculotropic mycosis fungoides would demonstrate atypical lymphocytes on histopathology, keratosis pilaris does not result in scarring alopecia, and central centrifugal cicatricial alopecia predominantly affects women of African descent with vertex-centered involvement.1
In this case, the diagnosis was established primarily on clinical and trichoscopic findings. Histopathologic features in GLPLS are frequently nonspecific and are most useful for excluding alternative diagnoses rather than confirming the condition.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bolduc C.Sperling L.C.Shapiro J.Primary cicatricial alopecia: lymphocytic primary cicatricial alopecias, including chronic cutaneous lupus erythematosus, lichen planopilaris, frontal fibrosing alopecia, and Graham-Little syndrome J Am Acad Dermatol 7562016108110992784694410.1016/j.jaad.2014.09.058 · doi ↗ · pubmed ↗
- 2Viglizzo G.Verrini A.Rongioletti F.Familial Lassueur-Graham-Little-Piccardi syndrome Dermatology 208220041421441505700510.1159/000076489 · doi ↗ · pubmed ↗
- 3Soto-García D.Feal-Cortizas C.Álvarez C.Couselo-Rodríguez C.Martínez-Fernández S.FlórezÁ.Familial Graham-Little-Picardi-Lassueur syndrome across 3 generations JAAD Case Rep 2320221281323549596910.1016/j.jdcr.2022.03.033PMC 9039857 · doi ↗ · pubmed ↗
- 4Bishnoi A.Mahajan R.Vishwajeet V.Saikia U.N.Scarring alopecia with follicular papules in a father and his daughter Clin Exp Dermatol 44320193373403015217310.1111/ced.13724 · doi ↗ · pubmed ↗
- 5Biondi G.Satta R.Lissia A.Fara A.M.Montesu M.A.Graham-Little-Piccardi-Lassueur syndrome in siblings Int J Dermatol 6092021 e 347e 3493377275510.1111/ijd.15534 · doi ↗ · pubmed ↗