Mood trajectories showing resilience and recovery in young people during and after the COVID-19 pandemic
Yara J. Toenders, Kayla H. Green, Lysanne W. te Brinke, Sophie W. Sweijen, Suzanne van de Groep, Matthijs Fakkel, Danielle Remmerswaal, Eveline A. Crone

TL;DR
This study tracks mood changes in young people during and after the pandemic, finding different recovery patterns and factors linked to resilience.
Contribution
The study identifies distinct mood trajectory profiles and their associated risk and protective factors in youth during the pandemic.
Findings
16% of youth showed high negative mood impact with slow recovery during the pandemic.
Two groups showed stable low to moderate mood levels throughout the pandemic.
Academic stress and executive functioning problems were linked to worse mood outcomes.
Abstract
The COVID-19 pandemic greatly affected daily life of young people but not all youth were affected in the same way. We studied mood trajectories in 363 young people (10–29 years) in the Rotterdam area in the Netherlands across eight longitudinal waves spanning four years to test for resilience and recovery profiles during and after the COVID-19 pandemic. A four-class model using growth mixture modelling confirmed that some adolescents were highly affected with slow recovery (16%), some were moderately affected (27%), and there were two patterns of stable low to moderate mood level groups (24% and 33% respectively). Those that were highly affected in negative mood were characterized by more academic stress, more executive functioning problems, and lower sense of belonging. The same factors were predictive and protective for recovery trends of vigor. These results confirm that group…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
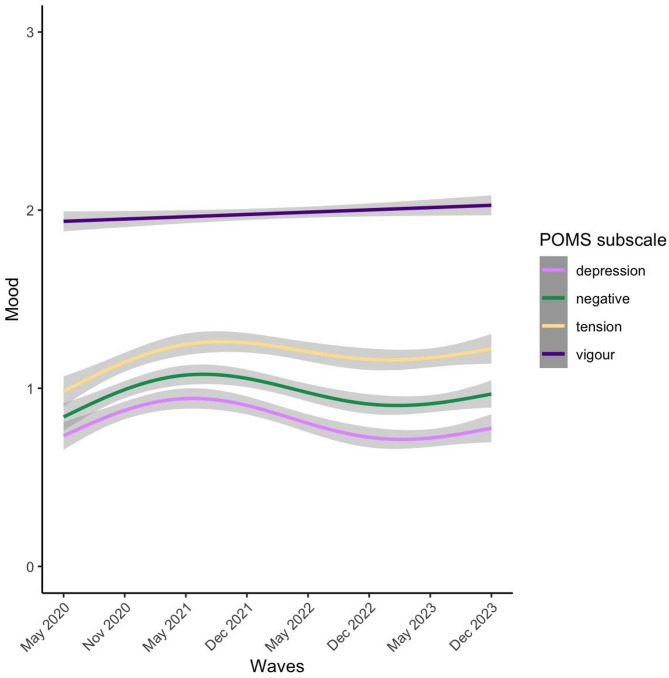 Figure 1
Figure 1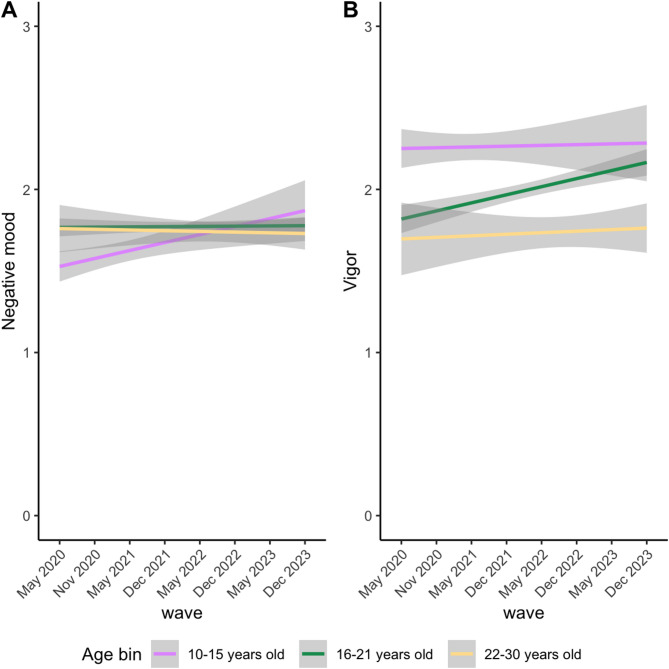 Figure 2
Figure 2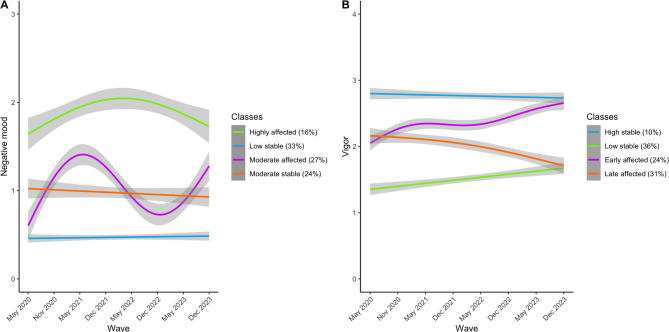 Figure 3
Figure 3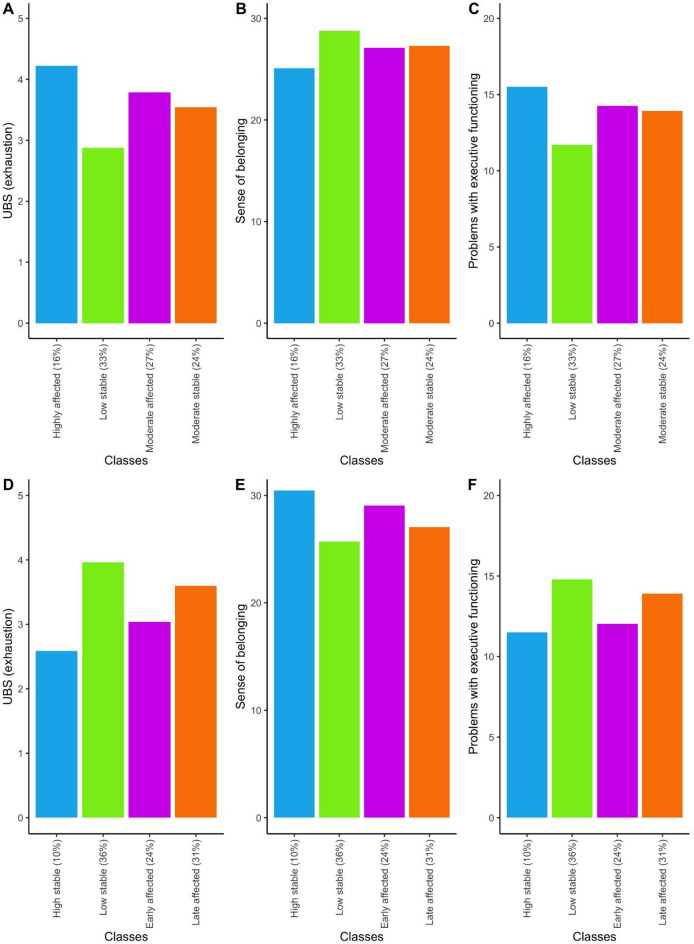 Figure 4
Figure 4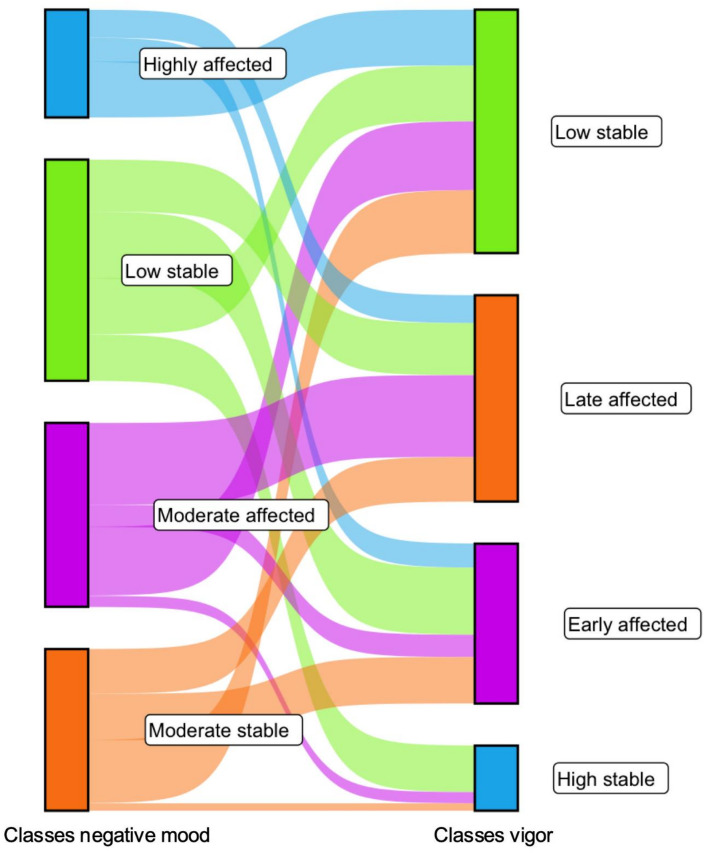 Figure 5
Figure 5- —Muller Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Resilience and Mental Health · Mental Health Research Topics
Introduction
The coronavirus disease 2019 (COVID-19) not only massively affected physical health worldwide, it also impacted mental health and wellbeing^1^. In March 2020, the WHO officially declared the COVID-19 infection spread a pandemic. As a result of pandemic-related policy measures such as social distancing, school closures, and lockdowns, people’s social environments became more restricted. The imposed restrictions and following social isolation resulted in feelings of loneliness, a decline in well-being, and an increase in psychopathological symptoms such as anxiety and depression^2–6^. Adolescents and young adults might have been particularly hit by these social restrictions, since adolescence is a sensitive period for social-affective development and many mental health difficulties develop during adolescence^5,7,8^.
Initial research on mental health during the pandemic showed that children and adolescents reported an increase in internalizing symptoms, both in the general population as in a cohort with existing mental health difficulties^6,9^. Moreover, parents reported an increase in internalizing symptoms for children in the general population. This increase in anxiety and depression was associated with the extent to which adolescents perceived their lifestyle to be affected by the COVID-19 pandemic^10^. Thus, it is important to not only examine the general response to a stressful situation, but also the individual differences.
Many individual trajectories of mood and resilience, the ability to maintain or regain well-being when experiencing adversity, might exist^11–13^. Some adolescents might be affected by a stressful situation initially, but recover swiftly, whereas others suffer from the situation more long-term. Others might not be affected by the adverse experience, or even benefit from it, as suggested by studies demonstrating lower mental health problems or no change in wellbeing^14–16^. Indeed, also after the school closures and lockdown, youth reported increased depression and anxiety compared to pre-COVID-19^17^. However, not all adolescents had similar mental health problems after the to the pandemic-related restrictions were introduced, suggesting that some adolescents are more resilient than others (Fernández et al.,^18^; Pedrini et al.,^19^). Factors that might have acted as a potential buffer for mental health difficulties included higher social or family support, physical activity, and the use of positive coping strategies^20^.
An important question concerns whether there are dissociable trajectories of how adolescents are impacted by pandemic restrictions, and what defined recovery and resilience^11^. Earlier studies into the effect of the prolonged stress of the COVID-19 pandemic suggest that these differential trajectories of mental health, mood and resilience exist^21^. In adults from the UK, it was shown that symptoms of depression and anxiety overall decreased after the first lockdown^22^, suggesting signs of resilience. However, risk factors such as being female, being younger, and having lower income were associated with higher depression and anxiety even when there was an overall decrease observed. Person-centered approaches in young people showed different resilience profiles during the pandemic, with protective factors such as male gender and being younger in a sample of 10–19 years old^23–25^. Higher negative mood, how one feels at a specific time, has been associated with lower mental health^26^. Therefore, prior studies not only examined mental health trajectories, but also mood trajectories. In adolescents, there were some initial increases in vigor found, potentially due to less demands that they might have experienced^27^. The trajectories of potential recovery after the COVID-19 pandemic in adolescents and the risk and resilience factors associated with these trajectories are not yet known. It is important to unravel these trajectories, that earlier person-centered studies hinted towards, as these individual differences can be precursors for mental health problems.
Therefore, in this longitudinal preregistered study (https://osf.io/y35gd) we aimed to examine different trajectories of resiliency, through measuring adolescent mood for a prolonged period of 4 years, during and after the COVID-19 pandemic (May 2020 to December 2023). We investigated how individual trajectories of mood vary in subgroups of adolescents and whether there are identifiable factors that distinguish resilient adolescents, those who were able to maintain their wellbeing or bounce back to being well, from their peers. This research question was investigated in the longitudinal Urban Rotterdam project. In this study adolescents aged 10–29 years old^28^filled out online questionnaires every 6 months for 8 waves. The first timepoint was collected two months after the start of COVID-19 in May 2020, and the last wave was post-pandemic in December 2023. It is hypothesized that four trajectories will be recognized^29,30^. The largest group is expected to show resiliency, displaying a decrease in negative mood post pandemic, with depression and tension at the highest levels during the first 2 timepoints (May 2020 and November 2020).
Next, we studied the effect of age on the development of mood throughout and after the pandemic, given that older adolescents are expected to display more negative mood^31^. Lastly, we examined whether the developmental trajectories of mood differ in protective or risk factors such as academic stress, academic drop-out, sense of belonging, and executive functioning^29^. The COVID-19 pandemic and the level of resilience might influence the school performance of young people (academic stress and academic drop-out), while sense of belonging and executive functioning might function as protective factors, increasing the likelihood that someone will be resilient^32–35^.
Methods
Participants and procedure
Participants from the Urban Rotterdam project were included in this study. Participants were Dutch young people aged 10 to 25 at their first timepoint and took part in the 8-wave longitudinal study (https://erasmus-synclab.nl/project/the-urban-rotterdam-project/). All participants signed an informed consent. Additionally, parents of adolescents aged 15 or below signed parental consent for participation in the study. From wave 4 onwards, new additional participants were recruited and included at each wave (Supplementary Figure S1). Participants were recruited through social media, schools, and our website. Participants filled out online questionnaires through the Qualtrics platform. In the first two waves, participants were asked to fill out daily questionnaires during a period of two weeks, and from wave 3 onwards participants only took part in one questionnaire per wave (approximately 30 min per wave). They received a monetary reward for participation, a total of €15 at wave 1 and 2, and €10 from wave 3 onwards. The Ethics Committee of the Erasmus School of Social and Behavioural Sciences at Erasmus University Rotterdam approved the study (application 20–036).
COVID-19 pandemic
The first wave of data collection took place in May 2020 during the first lockdown of the COVID-19 pandemic, during which social isolation restrictions were put into place. The second, third and fourth wave took place in December 2020, May 2021 and November 2021 respectively, at which time there were also lockdown restrictions in the Netherlands. The fifth to eighth waves were collected from May 2022 to December 2023, which are considered post-COVID (after lockdown restrictions had ended).
Measures
Mood
At each wave, participants filled out 19 items of a Dutch translation of 3 subscales from the Profiles of Mood States (POMS) questionnaire^36^. This is a self-report to assess current mood (in this study specifically tension, depression, and vigor). Participants were asked to what degree 19 adjectives described their current mood on a 5-point Likert scale, ranging from 0 (not at all) to 4 (extremely). In the first 2 waves, daily mood was collected for two consecutive weeks, however, the current study only used the mood data from the first day in line with the latter waves. A sum score was calculated for tension (ranged between 0 and 24), depression (ranged between 0 and 32) and vigor (ranged between 0 and 20). Items were summed to calculate the subscale scores. A sum score for negative mood, based on tension and depression was calculated (ranged between 0 and 56). Vigor was examined separately as an assessment of positive mood and resilience. The Cronbach alpha per subscale was 0.87, 0.92, 0.81, 0.94 for tension, depression, vigor and negative mood respectively. Mood during the first three waves has previously been reported^31,37^.
Executive functioning
Executive functioning was measured with the webexec questionnaire^38^. This questionnaire consists of 6 questions to measure problems with executive functioning such as ‘Do you find it difficult to keep your attention on a specific task?’, that are answered on a 4-point Likert scale. Items were summed to calculate the total score, with a higher score indicating more problems with executive functioning. The stability of this measure over time was examined and a mean score was calculated across all timepoints available by the participant. The intraclass coefficient (ICC) was 0.64 [0.60–0.68].
Academic stress
The exhaustion subscale of the Dutch version of the Maslach Burnout Inventory, called Utrecht Burnout Scale (UBOS) was used to measure academic stress at timepoint 2 to 8^39^. This subscale consists of 5 questions such as ‘At the end of a school/study day I feel empty’ that are rated on a 7-point Likert scale. A higher score indicates higher levels of exhaustion. A mean score was calculated across all timepoints available by the participant. The ICC was 0.55 [0.50–0.60].
Sense of belonging
The sense of belonging at school or studies was assessed using the school factor from the Social Connectedness Scale at wave 6^40^. This subscale consists of 9 questions such as ‘I feel at ease about how I should behave at my school/studies/work’ that are answered on a 4-point Likert scale. A higher score indicates a higher sense of belonging. A sum score of sense of belonging at wave 6 was calculated.
Academic drop-out
At each wave the participants filled out their current education. Based on this information a variable was derived that displayed whether participants dropped out of school, repeated a year, or continued their education. For the current study, participants were divided into 2 groups: continued as normal or other cases (which consisted of dropping out of school or repeating a year).
Statistical analyses
First, the development of mood throughout and after the COVID-19 pandemic was studied in the whole sample using general additive mixed models (GAMMs). This was a deviation from the preregistration since development of mood was found to be non-linear. Mood was used as the outcome variable, with wave as the predictor. A random effect for subject was added. Bayesian Information Criteria (BIC) was used to assess model fit to select the best k (representing the maximum degrees of freedom of the smoothing splines). The ‘mgcv’ package in R was used for the GAMM analyses^41^.
Next, to test whether there is a general developmental effect on mood development during and after the COVID-19 pandemic, a linear mixed model was tested with time and (linear and quadratic) age. Gender was included as a covariate, and a random intercept was added per participant.
Since large individual differences have been observed in the development of mood, we examined different trajectories of mood development throughout the COVID-19 pandemic using growth mixture modelling (GMM)^42^. For the GMM a strategy with 3 steps was used to handle the missing data. In the first step, only participants with data on at least a half of the timepoints were included. This means that participants were included in at least 4 waves of the Urban Rotterdam study. The remaining missing data was imputed using predictive mean matching from the mice package in R^43^. We included age at first wave and gender and all POMS subscales across waves in the imputation model. Five imputed datasets with 50 iterations each were created, the first completed dataset was used in the subsequent analyses. The next step was then to do a sensitivity analysis for which only participants with (almost) complete data were included to test whether the imputation did not majorly alter the results. Only participants with POMS data on at least 7 timepoints were included for this sensitivity check. Lastly, a more lenient approach was taken, for which participants with data on at least 2 timepoints were available were included. The results of these sensitivity analyses can be found in the Supplemental Material.
The mood trajectories were separately identified based on the negative (tension and depression) and positive (vigor) subscales of the POMS. GMM can be used to find trends over time in longitudinal data, while accounting for between-person effects. The ‘lcmm’ package in R was utilized for the analyses^44^. We executed models with an increasing number of trajectories until non-convergence or the proportion of participants per trajectory was below 5%. The fit of the consecutive models were compared using the Akaike Information Criterion (AIC), the Bayesian Information Criterion (BIC), and entropy. We then tested what GMM had a better fit with the Lo-Mendell-Rubin test (LMR).
Next, the different groups (with distant mood trajectories throughout and after the COVID-19 pandemic) were compared on demographic and protective or risk factors. Group membership was predicted based on age, gender, education, psychiatric diagnosis at inclusion, and academic drop-out. Next, the trajectories were compared, by looking at academic stress (burnout), sense of belonging, and mean executive functioning across waves. Analyses for differences on baseline measures were Bonferroni corrected (4 analyses), as well as the analyses for differences on protective or risk factors (3 analyses).
Results
Data from 363 participants who participated in at least 4 timepoints were included, leading to a total of 2904 observations of mood after imputation (Table 1).
Table 1. Overview of demographic and protective or risk factors across waves before imputation. Mean (SD) are being displayed unless otherwise specified. N Mean (SD)363 Demographics Age at first inclusion17.9 (3.2)Gender (M/F/non-binary/other) n (%)76 (21%) / 279 (77%) / 3 (1%) / 5 (1%)Ethnicity at first inclusionDutch243 (67%)Multiple ethnicities including Dutch66 (18%)Education at first inclusionPrimary school2 (1%)High school VMBO6 (2%)High school HAVO/VWO185 (51%)Vocational education (mbo)45 (12%)Higher education (hbo/university)99 (27%)No education25 (7%)Academic drop-out (continued, repeated year, drop-out) n (%)277 (76%) / 12 (3%) / 38 (11%) Mood Tension7.2 (4.3)Depression6.6 (5.2)Negative (sum tension and depression)13.8 (9.1)Vigor10.0 (3.3) Protective or risk factors Utrecht Burnout Scale3.5 (1.3)Executive functioning13.5 (3.9)Sense of belonging27.4 (5.2)
Development of mood during and after the COVID-19 pandemic
Across the entire sample of adolescents, the development of mood during the pandemic was examined using general additive mixed models (GAMMs). It was found that both the negative subscales (tension and depression) and the positive subscale of the POMS (vigor) changed over time (F = 16.99, p<.001, k = 4; F = 19.86, p<.001, k = 4; F = 7.08, p=.02, k = 3 respectively; Fig. 1 and Supplemental Table S1). Tension and depression peaked around wave 3 and 4 (May and December 2021), followed by a subsequent decrease. This decrease was larger for depression than tension. For all subsequent analyses, the two negative subscales tension and depression were combined into one negative subscale because of their high correlation (r=.79, Supplementary Figure S2). Vigor showed a linear increase throughout the waves. Negative mood and vigor were only moderately negatively correlated (r=-.44), therefore they were treated as separate variables in the analyses.
Fig. 1. Development of mood (per subscale) during and after the COVID-19 pandemic. The y-axis presents the mood sum score per subscale (averaged for visualization purposes). Negative mood was the summed value of the depression and tension subscales. The x-axis represents the different waves, from May 2020 to December 2023.
Effect of age on the development of mood during and after the COVID-19 pandemic
Before analysing the classes, we first tested the possible effects of age on the development of mood during and after the COVID-19 pandemic using linear mixed effect models. It was found that age and wave showed an interaction for negative mood (F = 6.47, p = < 0.001), but not vigor (F = 2.12, p=.08). Vigor only showed a main effect of age, with younger ages showing higher vigor (F = 29.72, p = < 0.001). Figure 2 presents the age effects across waves. For visualization purposes, age was divided into three bins (early adolescence, late adolescence and young adulthood). As can be seen in Fig. 2, adolescents with higher ages showed a more negative mood during COVID-19, but they recovered post-COVID, whereas younger adolescents were less affected but did not show a post-COVID decline in negative mood.
Fig. 2. Interaction between age and wave on mood (A: negative mood, B: vigor) during and after the COVID-19 pandemic. The y-axis presents the mood sum score per subscale (averaged for visualization). Age was divided into bins for visualization purposes only. Wave and age showed an interaction effect for negative mood, with younger ages being less affected by the COVID-19 pandemic, but older ages showing a recovering effect post-COVID. A main effect for age was found for vigor, with younger ages showing more positive mood.
Different trajectories of mood during and after COVID-19
Next, we addressed the question whether classes could be distinguished for negative mood trajectories across the waves. For negative mood, a model with 4 different trajectories was considered the best fit based on AIC, entropy, and Lo-Mendell-Rubin test (Supplementary Table S2, Fig. 3A). We identified two classes that did not show a change in mood during the COVID-19 pandemic. They differed on the average negative mood, resulting in a ‘low negative mood’ (Low stable – 33%) and a ‘moderate negative mood’ class (Moderate stable – 24%). The third class (Highly affected – 16%) was characterized by high negative mood, especially during the COVID-19 pandemic, peaking at the third and fourth wave (May 2021 and November 2021), with a small recovering effect afterwards. However, in this group negative mood remained at early pandemic level. The final class (Moderate affected – 27%) showed a similar increase in negative mood during the COVID-19 pandemic, and a subsequent decline, returning to similar levels as the moderate stable class. Similar results were found in the more stringent and lenient dataset (Supplementary Table S3, Supplementary Figure S3-S5).
Fig. 3. Four different trajectories of (left) negative mood and (right) vigor during and after the COVID-19 pandemic. The y-axis on the left presents the negative mood per wave per class (averaged for visualization purposes). The y-axis on the right presents vigor per wave per class (averaged for visualization purposes). The trajectories per class were fit using GAM with 3 knots, linear regression, GAM with 4 knots and linear regression (respectively per class for negative mood) and linear regression, linear regression, GAM with 5 knots and GAM with 3 knots (respectively per class for vigor).
Based on vigor, a model with four different classes was also identified as the optimal solution (Supplementary Table S2). As can be seen in Fig. 3B, the first class was characterized by high stable levels of vigor (High stable, n = 58 (10%)), the second and largest class by low vigor, that slightly improved after the COVID-19 pandemic (Low stable, n = 119 (36%)). The third class showed lower vigor in the earlier waves but improving levels of vigor comparable to the level of the high stable class in the later waves (Early affected, n = 99 (24%)) and lastly the fourth class was characterized by high levels of vigor in the earlier waves but decreasing levels of vigor in the later waves, to the level of the stable low class (Late affected, n = 87 (31%)). Similar results were found in the more stringent and lenient dataset (Supplemental Material).
Identifiable factors of trajectories of mood during and after the COVID-19 pandemic
The identified trajectories of mood based on negative mood and vigor were then compared on identifiable factors. The negative mood classes did not differ based on mean age at inclusion, gender, education, and percentage of academic drop-out (Table 2). However, significant differences were found for academic stress, sense of belonging and executive functioning. Academic stress was lower in the low stable negative mood class compared to the highly affected class, and the other two classes scored in between (Fig. 4; F(3) = 18.95, p<.001). The low stable class had a higher sense of belonging than the highly affected class, and the other two groups did not differ from either of them (F(3) = 4.74, p=.009). Finally, the low stable class showed less problems with executive functioning relative to the highly affected class and the other classes scored at an in between level (F(3) = 17.61, p<.001). Together, these findings show protective effects of sense of belonging and executive functions and accelerating effects of academic stress.
Table 2. Overview of demographic and protective or risk factors per class based on different trajectories of negative mood and Vigor during and after COVID-19 pandemic.Classes based on negative moodHighly affectedLow stableModerate stableModerate affected p N (%)58 (16%)119 (33%)99 (27%)87 (24%)Female (%)84%73%81%80%1.00 (X(3) = 3.49)Mean age at first wave of inclusion18.1617.7917.6418.001.00 (F(3) = 0.39)Education0.90 (X(18) = 22.15) Primary school 0 (0%)2 (2%)0 (0%)0 (0%) High school 30 (54%)67 (56%)55 (56%)39 (45%) Higher education 26 (46%)39 (33%)36 (36%)43 (49%)Academic dropout (%)14%13%20%13%1.00 (X(3) = 2.2)Psychiatric diagnosis at inclusion23%9%14%13%0.59(X(3) = 5.89) Classes based on vigor High vigorLow vigor and improveMiddle vigor and improveMiddle and decreasing p N (%)35 (10%)131 (36%)86 (24%)111 (31%)Female (%)57%84%71%85%0.002 (X(3) = 18.91)Mean age at first wave of inclusion16.1918.3617.7317.901.00 (*F(*3) = 0.40)Education0.28 (X(18) = 28.35) Primary school 1 (3%)0 (0%)1 (1%)0 (0%) High school 25 (71%)68 (52%)46 (53%)52 (47%) Higher education 7 (20%)52 (40%)32 (37%)52 (47%)Academic dropout (%)12%15%19%14%1.00 (X(3) = 1.41)Psychiatric diagnosis at inclusion9%19%5%14%0.18(X(3) = 8.54)
Fig. 4. Protective and risk factors per class based on the negative mood (above) and vigor (below) trajectories.
The classes based on vigor differed on sex, as the high stable vigor class consisted of fewer females than the other three classes (X(3) = 18.91, p<.001) (Table 2). Academic stress was lower in the high stable vigor class and early affected classes compared to the other two classes (Fig. 4; F(3) = 17.08, p<.001). These classes were additionally characterized by higher sense of belonging (F(3) = 10.05, p<.001), and less executive functioning problems (F(3) = 13.79, p<.001). Together, these findings show a two-class differentiation in protective effects of sense of belonging and executive functions and accelerating effects of academic stress, rather than a gradual effect.
Overlap between trajectories
To examine whether participants showed similar trajectories for negative mood and vigor, the overlap between the classes was studied. As can be seen in Fig. 5, there is variability in negative mood and vigor classes, confirming that these classes should be studied separately. The low stable negative mood class shows most overlap with the two highest vigor classes (high stable and early affected). The highly affected negative mood class showed most overlap with the low stable vigor class but not vice versa.
Fig. 5. Overlap between classes based on negative mood development and vigor development.
Discussion
In the current study mood during and after the COVID-19 pandemic was examined in a longitudinal sample of adolescents aged 10–29. Prior research showed that this age group was relatively highly affected in terms of mental health problems compared to other age groups^45,46^. The aim of the study was to investigate in more detail whether there were distinct profiles in how adolescents’ mood responds to a stressful crisis. Consistent with prior research^6,9,47^, on a group level, adolescents showed an increase in negative mood during the COVID-19 pandemic, explained by both an increase in depression and tension, which declined after the pandemic restrictions had ended. Notably, adolescents’ feelings of tension remained relatively high after the restrictions during the pandemic had ended, whereas feelings of vigor gradually increased over time. This shows that adolescence is a vulnerable period, however, adolescents most likely differ in their patterns of resilience^11^. Indeed, we confirmed that the development of mood is better understood when adolescents were divided into subgroups, showing that different adolescents experienced different trajectories of mood over time. The current results should be interpreted with caution, as the observed changes in mood cannot be causally attributed to the pandemic.
Prior research in adolescents mostly studied average trajectories in mood during the COVID-19 pandemic. However, this does not consider how subgroups of adolescents deal with stressful situations, and what they might need in future crises. The subgroups of adolescents showed that the mood of a small majority of adolescents was not affected by the COVID-19 pandemic (57%). However, there were two groups who were significantly more affected by the COVID-19 pandemic and they only showed moderate levels of recovery. Contrary to earlier research, these subgroups only showed a decline in negative mood after the COVID-19 restrictions had finished, some even with a lingering effect^47^. Especially the adolescents who were highly affected (16%) that also showed a high average level of negative mood were characterized by a low sense of belonging, which might be a protector for the groups that showed resilience^33^. In addition, these adolescents showed more executive problems and higher academic stress. These higher levels of executive functioning problems could be a risk factor for negative mood^34^. It might be that less problems with executive functioning, could help adolescents with coping and therefore lead to higher levels of resilience^48^.
Adolescents also showed different trajectories regarding positive mood, specifically vigor, during and after the COVID-19 pandemic. The early affected group could be considered the most resilient, as they showed an initial effect of the COVID-19 pandemic on their vigor but recovered after restrictions had ended. This group, in addition to the high stable group, also showed the most promising protective measures, with high sense of belonging, low burnout and low levels of problems with executive functioning. This suggests that while it is common for adolescents to respond to stressful situations, those who show resilience effects, also experience protective effects of low academic stress, fewer executive functioning problems and more sense of belonging. It should be noted that sense of belonging was assessed post-pandemic, which can therefore not be interpreted as a predictive factor. Earlier research has shown that sense of belonging is relatively stable^49^, but in the current study it might have been affected by the pandemic.
The results are in line with earlier research in adults over the course of 1 year during the pandemic^29^. Here they also identified 4 groups, including a resilient group, an improving group, a worsening group, and a chronic group. The adults in the chronic group were characterized by more emotion regulation difficulties and a more challenging financial situation. However, they did not include data after the pandemic, which lacks the possibility to test how and whether adults recovered post-pandemic. We did not identify a group that showed chronic levels of negative mood that sustained after the pandemic. Although for the adolescents who were highly affected, their negative mood levels did not improve to be lower than those observed during the first COVID-19 lockdown. It should be noted that resilience is a multisystem construct; the current study examining mood trajectories focussed on individual psychological resilience, but future studies could also consider resilience in the adolescent’s social environment, or societal factors such as^50^.
It is important to consider that adolescents might respond differently than adults to the social restrictions, as adolescence is a time of social reorientation. During adolescence the influence of peers becomes increasingly important^51,52^. Adolescents spend more time with their peers and changes in social environment might contribute to the enhanced sensitivity of adolescents for social rejection by peers^53^. Thus, adolescence is a formative period for social processing, which might be dependent on the development of the social brain^54,55^. It is well known that even during pre-pandemic times, adolescents were at higher risk of developing mental health difficulties; 50% of all mental disorders are diagnosed before age 15 and almost 75% before age 25^56,57^. Therefore, it is important to monitor the development of mental health and wellbeing within this group, as they might be especially vulnerable for the effect of changes in the social environment on their mental wellbeing. Especially as they grew up in times of social restriction and lockdowns^5^. In addition, the current study showed that while some young people show individual resilience, others might need additional support from their social environments in challenging times.
The strengths of the current study included the large longitudinal data collection during and after the COVID-19 pandemic, which allowed us to study how and whether adolescents recovered, and the steps taken to test the reliability in more stringent and lenient datasets. However, some limitations should be considered. First, the study started after the COVID-19 pandemic had already begun, with the first wave of data collection taking place in May 2020 during the first lockdown (two months after the start of the pandemic). This means that pre-pandemic mood was not examined in this study. However, this limitation was mitigated by comparison to reports that showed an early pandemic effect on mood by comparing pre-and early pandemic levels^58^, by comparing psychiatric diagnosis at inclusion, and by having information on multiple waves of mood after the COVID-19 pandemic, which allowed us to study how adolescents’ mood recovered when the social situation returned to the pre-pandemic situation. Second, the current study examines mood trajectories, which is related to mental health^26^, but mood is subject to contextual factors (e.g., daily problems and sleep). Future studies could replicate these findings using questionnaires that assess mental health directly. Third, the classes found should be replicated in an independent sample, to examine their stability and replicability, also across different contexts (e.g., other regions). We conducted sensitivity analyses to examine the effects of sample, especially because adolescents with higher negative mood might show higher attrition rates. The lenient sample might therefore be more representative of the general population, in terms of gender, education and mood. The sensitivity analyses showed very similar results to the main analyses, with groups of adolescents who showed more stable mood, and groups that were affected but recovered after the pandemic had ended. Future sensitivity analyses could also focus on more specific age groups, such as early, middle or late adolescence, since the age range included in the current study is relatively large.
Interestingly, the groups identified based on negative mood were different from the groups based on positive mood. While there was some overlap, such as the low negative mood class overlapping with the classes with the higher vigor levels, the largest part of the groups did not overlap. This suggests that positive and negative mood are two separate processes, and not opposites on a spectrum, which is in line with previous studies suggesting them to be independent and having separable contributions to social functioning^59^. This is in line with the distinction between hedonic and eudaimonic well-being, as the reduction of negative affect (hedonic) does not automatically translate into heightened eudaimonic flourishing^60^. Therefore, future studies should also consider the resilience effect of vigor in stressful situations, as resilience in one domain does not imply resilience in another domain.
To conclude, this study showed that different adolescents had different trajectories of mood during and after the COVID-19 pandemic, arguing against a one-size fits all approach when providing support. Not every adolescent experiences and responds to a stressful situation similarly. Therefore, the effect of risk factors such as social restrictions on mental wellbeing should be monitored for potential future preventive strategies as it might differentially affect adolescents.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Panchal, U. et al. The impact of COVID-19 lockdown on child and adolescent mental health: systematic review. European Child and Adolescent Psychiatry. 32 1151–1177 Preprint at (2023). 10.1007/s 00787-021-01856-w 10.1007/s 00787-021-01856-w PMC 837143034406494 · doi ↗ · pubmed ↗
- 2Li, J. et al. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry. 19 249–250 Preprint at (2020). 10.1002/wps.2075810.1002/wps.20758 PMC 721495932394560 · doi ↗ · pubmed ↗
- 3Brooks, S. K. et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. The Lancet. 395 912–920 Preprint at (2020). 10.1016/S 0140-6736(20)30460-810.1016/S 0140-6736(20)30460-8PMC 715894232112714 · doi ↗ · pubmed ↗
- 4Orben, A., Tomova, L. & Blakemore, S. J. The effects of social deprivation on adolescent development and mental health. The Lancet Child and Adolescent Health. 4 634–640 Preprint at (2020). 10.1016/S 2352-4642(20)30186-310.1016/S 2352-4642(20)30186-3PMC 729258432540024 · doi ↗ · pubmed ↗
- 5Blakemore, S. J. Development of the social brain in adolescence. Journal of the Royal Society of Medicine. 105 111–116 Preprint at (2012). 10.1258/jrsm.2011.11022110.1258/jrsm.2011.110221 PMC 330864422434810 · doi ↗ · pubmed ↗
- 6Earvolino-Ramirez, M. Resilience: a concept analysis. Nursing forum. 42 73–82 Preprint at (2007). 10.1111/j.1744-6198.2007.00070.x 10.1111/j.1744-6198.2007.00070.x 17474940 · doi ↗ · pubmed ↗
- 7Toenders, Y. et al. Mood swings during development and their relation to sleep and brain development. Sci Rep 8537 (2024).10.1038/s 41598-024-59227-9PMC 1101492838609481 · doi ↗ · pubmed ↗
- 8Penner, F., Hernandez Ortiz, J. & Sharp, C. Change in youth mental health during the COVID-19 pandemic in a majority Hispanic/Latinx US sample. J Am. Acad. Child. Adolesc. Psychiatry. 60(4), 513–523 (2021).10.1016/j.jaac.2020.12.02733359408 · doi ↗ · pubmed ↗