Dropout rates and factors associated with adherence to opioid agonist treatment among adults with opioid use disorder at Sekou Toure Regional Referral Hospital, Mwanza, Tanzania
Tusherahma Hussein Tuli, Allen Rweyendera, Greyson Gwahula, Yacinter Vedastus, Raymond Maziku, Peter Chilipweli, Kiyeti A. Hauli

TL;DR
This study found a high dropout rate in opioid treatment in Tanzania and identified factors like gender, education, and social support that affect adherence.
Contribution
The study provides insights into dropout factors for opioid treatment in a Tanzanian hospital setting.
Findings
The dropout rate for opioid agonist treatment was 37.9%.
Most dropouts were men with primary education and limited social support.
Perceived treatment effectiveness was low, with 46.6% rating it as effective or very effective.
Abstract
Opioid use remains a significant global public health concern, with approximately 60 million people using opioids and 39.5 million living with opioid use disorders. Opioid agonist treatment (OAT), particularly methadone, is an effective intervention for opioid dependence, though retention remains problematic worldwide. This study aimed to determine the dropout rate and identify factors influencing adherence to OAT among patients at Sekou Toure Regional Referral Hospital (SRRH) in Mwanza, Tanzania. A mixed-method design combining a retrospective cohort and cross-sectional approach was used. Retrospective data were extracted from records of patients enrolled from February 2018 to March 2024. A cross-sectional survey was conducted from September to November 2024 among 223 systematically selected patients. Data analysis included descriptive statistics and Chi-square tests, with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
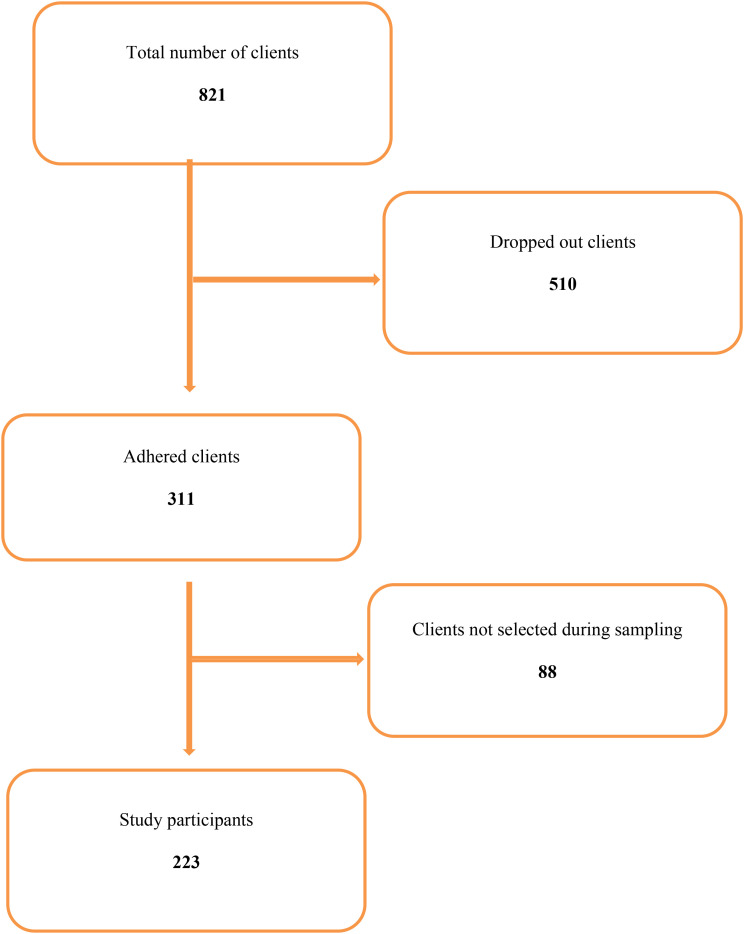 Figure 1
Figure 1| Variable | Categories | Frequency | Percentage |
|---|---|---|---|
| Gender | Female | 91 | 11.0 |
| Male | 730 | 89.0 | |
| Age group | 18-25 | 178 | 21.7 |
| 26-35 | 129 | 15.7 | |
| 36-45 | 161 | 19.6 | |
| 46-55 | 198 | 24.1 | |
| 56+ | 155 | 18.9 | |
| Educational level | No formal education | 113 | 13.7 |
| Primary | 392 | 47.7 | |
| Secondary | 248 | 30.1 | |
| Tertiary (collage/university) | 68 | 8.5 | |
| Marital status | Single | 414 | 50.4 |
| Married | 242 | 29.4 | |
| Divorced | 165 | 20.1 | |
| Employment | Employment | 323 | 39.3 |
| Unemployed | 498 | 60.7 |
| Variable | Categories | Frequency | Percentage |
|---|---|---|---|
| Age | 18-25 | 54 | 24.2 |
| 26-35 | 34 | 15.2 | |
| 36-45 | 44 | 19.7 | |
| 46-55 | 54 | 24.2 | |
| 56+ | 37 | 16.6 | |
| Gender | Female | 19 | 8.5 |
| Male | 204 | 91.5 | |
| Employment status | Employed | 50 | 22.4 |
| Retired | 64 | 28.7 | |
| Student | 15 | 6.7 | |
| Unemployed | 94 | 42.1 | |
| Educational level | No formal education | 58 | 26.0 |
| Primary | 55 | 24.7 | |
| Secondary | 46 | 20.6 | |
| Tertiary | 64 | 28.7 | |
| Living situation | Alone | 35 | 15.7 |
| Other | 51 | 22.9 | |
| Shelter | 51 | 22.9 | |
| With family | 50 | 22.4 | |
| With friends | 36 | 16.1 | |
| Treatment period | 6–12 months | 52 | 23.3 |
| 1–2 years | 67 | 30.0 | |
| 2+ years | 104 | 46.6 |
| Variable | Categories | Frequency | Percentage |
|---|---|---|---|
| Gender | Female | 4 | 2.6 |
| Male | 149 | 97.4 | |
| Educational level | No formal education | 21 | 13.7 |
| Primary | 73 | 47.7 | |
| Secondary | 46 | 30.1 | |
| Tertiary (collage/university) | 13 | 8.5 | |
| Marital status | Divorced | 27 | 17.6 |
| Married | 45 | 29.4 | |
| Single | 81 | 52.9 |
| Variable | Categories | Frequency | Percentage |
|---|---|---|---|
| Personal motivations and beliefs | |||
| Personal goals | Gain employment | 49 | 22 |
| Improve health | 62 | 27.8 | |
| Maintain sobriety | 61 | 27.4 | |
| Reunite with family | 51 | 22.9 | |
| Confidence in adherence | Confident | 39 | 17.5 |
| Neutral | 47 | 21.1 | |
| Not confident | 41 | 18.4 | |
| Very confident | 59 | 26.5 | |
| Very unconfident | 37 | 16.6 | |
| Motivation | Employment | 34 | 15.2 |
| Family | 48 | 21.5 | |
| Health | 44 | 19.7 | |
| Legal | 54 | 24.2 | |
| Personal growth | 43 | 19.3 | |
| Effectiveness | Effective | 52 | 23.3 |
| Ineffective | 46 | 20.6 | |
| Neutral | 43 | 19.3 | |
| Very effective | 52 | 23.3 | |
| Very ineffective | 30 | 13.5 | |
| Social support | |||
| Support network | Moderate | 62 | 27.8 |
| None | 57 | 25.6 | |
| Strong | 42 | 18.8 | |
| Weak | 62 | 27.8 | |
| Communication frequency | Daily | 51 | 22.9 |
| Monthly | 47 | 21.1 | |
| Rarely | 66 | 29.6 | |
| Weekly | 59 | 26.5 | |
| Provider support | Excellent | 45 | 20.2 |
| Good | 42 | 18.8 | |
| Neutral | 49 | 22 | |
| Poor | 52 | 23.3 | |
| Very poor | 35 | 15.7 | |
| Psychological factors | |||
| Experiencing severe Psychological issues | yes, severe | 85 | 38.1 |
| Yes, mild | 65 | 29.1 | |
| no | 73 | 32.7 | |
| Cravings or urges to use heroin | Engaging in other activities | 79 | 35.4 |
| Not sure | 39 | 17.5 | |
| Seeking support from others | 93 | 41.7 | |
| Using coping strategies | 12 | 5.4 | |
| Engaged in any counseling | Yes, occasionally | 118 | 52.9 |
| Yes, regularly | 68 | 30.5 | |
| No | 37 | 16.6 | |
| Treatment environment | |||
| Environment of heath facility | Neutral | 75 | 33.6 |
| Supportive but could improve | 57 | 25.6 | |
| Unsupportive | 51 | 22.9 | |
| Very supportive and welcoming | 40 | 17.9 | |
| Adequate privacy | No | 83 | 37.2 |
| Yes, always | 53 | 23.8 | |
| Yes, sometimes | 87 | 39 | |
| Variable | Adhered (%) | Dropped out (%) | Chi-square | p-value |
|---|---|---|---|---|
| Gender | ||||
| Male | 91.5 | 97.4 | 5.12 | 0.02 |
| Female | 8.5 | 2.6 | ||
| Age group | ||||
| 18-25 | 24.2 | 21.7 | 1.12 | 0.45 |
| 26-35 | 15.3 | 15.7 | ||
| 36-45 | 19.7 | 19.6 | ||
| 46-55 | 24.2 | 24.1 | ||
| 56+ | 16.6 | 18.9 | ||
| Education level | ||||
| - Primary | 47.7 | 47.7 | 4.56 | 0.04 |
| - Secondary (%) | 30.1 | 30.1 | ||
| - Higher | 13.7 | 8.5 | ||
| Employment status | ||||
| - Employed | 22.4 | 30.0 | 3.89 | 0.05 |
| - Unemployed | 42.1 | 70.0 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOpioid Use Disorder Treatment · Substance Abuse Treatment and Outcomes · HIV, Drug Use, Sexual Risk
Introduction
1
Opioid use remains a major global public health challenge. According to the 2023 World Drug Report, 296 million people used drugs in 2021, with amphetamine-type stimulants being more widely used globally than opioids. Approximately 60 million people used opioids, and 31.5 million used opiates such as heroin. Opioids contribute to the majority of drug-related deaths, mainly due to overdose, with risk highest shortly after treatment discontinuation when tolerance has diminished (1).
Opioid agonist treatment (OAT), including methadone, buprenorphine, slow-release oral morphine (SROM), and heroin-assisted treatment (HAT), is the most effective intervention for opioid dependence. These medications alleviate withdrawal symptoms, reduce cravings, and decrease the likelihood of relapse, overdose, and infectious disease transmission. Antagonist medications such as naltrexone play a more limited role globally due to adherence barriers and restricted availability in low-resource settings.
In Tanzania, OAT was introduced in 2011 and has expanded to multiple regions, including Mwanza. Despite this progress, retention remains a major challenge. Studies from Dar es Salaam have documented dropout rates ranging from 30% to 40% (2, 3), with retention influenced by methadone dosing, psychosocial support, comorbid mental health conditions, stigma, transport challenges, and facility-level factors.
However, most evidence comes from Dar es Salaam, and little is known about adherence and dropout patterns in regional referral hospitals such as SRRH in Mwanza. This represents a critical knowledge gap, particularly because treatment discontinuation is associated with relapse, overdose, increased mortality, and poor social outcomes.
Therefore, this study aimed to determine the dropout rate and identify factors influencing adherence to OAT among patients attending Sekou Toure Regional Referral Hospital in Mwanza, Tanzania.
Methodology
2
Study area
2.1
The study was conducted at the Methadone Clinic of Sekou Toure Regional Referral Hospital (SRRH) in Mwanza, Tanzania. The hospital serves approximately 2.2 million people in the Lake Zone and provides methadone-based OAT to a large population of adults with opioid use disorder.
Study design
2.2
A mixed-methods approach combining a retrospective cohort and cross-sectional design was used. The retrospective component assessed OAT dropout using clinical records of patients enrolled between February 2018 and March 2024. The cross-sectional survey, conducted from September to November 2024, assessed current factors associated with adherence among active patients. This integration allowed examination of both historical trends and current determinants of adherence.
Study population
2.3
The study population included all heroin-dependent patients enrolled in OAT between February 2018 and March 2024 and who had been on treatment for at least six months. Complete clinic records up to March 2024 were available. Files with significant missing information were excluded to ensure data validity.
Sample size estimation, selection criteria and sampling method
2.4
Sample size was calculated using the Kish–Leslie formula with a 95% confidence interval, 5% margin of error, and a prevalence of heroin use (17.6%) from a national Tanzanian survey. Because no reliable dropout prevalence data existed for Mwanza at the time of planning, heroin-use prevalence served as the best available estimate.
“Heroin smoking alone” refers to individuals who used heroin exclusively by smoking rather than injection.
A systematic random sampling technique was used to select 223 eligible patients.
Inclusion criteria:
Verified heroin use confirmed through clinical assessment, patient history, and urine drug screeningEnrollment in OAT for ≥6 monthsAttendance at SRRH during the study period
Exclusion criteria:
Primary dependence on non-opioid substances.
Patients with co-occurring substance use were included if heroin was the primary drug.
Data collection data analysis
2.5
Data were collected using two tools: a checklist and a self-administered questionnaire. The checklist was used to extract secondary data from clinic records regarding patients’ dropout rates from methadone-assisted treatment (OAT), while the self-administered questionnaire was designed to assess factors contributing to adherence among patients receiving OAT. The questionnaire captured variables such as socio-demographic characteristics, duration on treatment, support systems, and individual perceptions toward OAT. All completed questionnaires were coded and assigned serial numbers for ease of reference and data management. The collected data were compiled, cleaned, and analyzed using the Statistical Package for the Social Sciences (SPSS) software version 26. Descriptive statistics including frequencies and percentages were used to summarize categorical variables. Cross-tabulation was performed to explore associations between independent variables and adherence status, and Chi-square tests were used to determine statistical significance. A p-value of less than 0.05 was considered statistically significant.
Ethics
2.6
Ethical approval was soughed from the Joint BMC/CUHAS Research Ethical Committee and Director of research and innovation CUHAS numbered CRECU/3378/2024. Written informed consent was sought and obtained before the recruitment of study respondents, after they were provided with sufficient information about the risks and benefits of the study. Confidentiality was ensured, and those who agreed to participate signed the consent form, while illiterate participants provided a thumbprint.
Results
3
Sociodemographic information of study participants
3.1
This section presents the demographic characteristics of the study participants, including gender, age, education level, marital status and employment status (Table 1).
Characteristics of adhered clients
3.2
Characteristics of patients who remained in methadone treatment provide insight into factors contributing to adherence (Table 2).
Dropout rate
3.3
The dropout rate among patients enrolled in OAT at SRRH was 37.9%. Of the 821 patients registered between 2018 and 2024, 510 discontinued treatment. Most patients were male, and this distribution was mirrored among dropouts (97.4%). Therefore, the high proportion of male dropouts reflects the underlying gender distribution of the clinic population (Figure 1; Table 3).
Flow diagram of study patients included in the analysis.
Factors for adherence to medication assisted treatment
3.4
Living situations further illustrate the patients’ varied support systems, with 22.9% each living in shelters or other arrangements, 22.4% living with family, 16.1% with friends, and 15.7% living alone. Treatment duration plays a crucial role in adherence, with the largest group (46.6%) having been on treatment for more than 2 years, followed by those on treatment for one to two years (26.9%), 6–12 months (23.3%). These findings underscore the importance of targeted interventions tailored to specific age groups, gender identities, and socioeconomic backgrounds to improve adherence rates and support systems among patients with heroin dependence undergoing OAT.
Factors influencing adherence to Opioid Agonist Treatment (OAT) among patients with heroin dependence at Sekou-Toure Methadone Clinic highlight the critical role of personal motivations and beliefs. Clients cited improving health (27.8%), maintaining sobriety (27.4%), reuniting with family (22.9%), and gaining employment (22.0%) as key personal goals for adherence. Confidence levels varied, with 26.5% feeling very confident in their ability to adhere to treatment, while 16.6% were very unconfident. Motivational factors included legal concerns (24.2%), family (21.5%), health (19.7%), personal growth (19.3%), and employment (15.2%). Perceived effectiveness of OAT also played a role, with 23.3% rating it as very effective and 23.3% as effective, compared to 20.6% who found it ineffective and 13.5% who deemed it very ineffective. These findings underline the importance of addressing patients’ personal goals and reinforcing confidence and perceived effectiveness to enhance treatment adherence.
Social support significantly influences adherence to Opioid Agonist Treatment (OAT) among patients with heroin dependence at Sekou-Toure Methadone Clinic. The strength of support networks varied, with 27.8% describing their support as moderate or weak, while 18.8% reported having strong support, and 25.6% indicated no support at all. Communication frequency with their support networks showed that 29.6% rarely communicated, 26.5% communicated weekly, 22.9% daily, and 21.1% monthly. Regarding provider support, 20.2% rated it as excellent and 18.8% as good, while 23.3% found it poor, 15.7% very poor, and 22.0% remained neutral. These findings underscore the need to strengthen both personal and provider-based support systems to improve treatment adherence.
Psychological factors play a crucial role in adherence to Opioid Agonist Treatment (OAT) among patients with heroin dependence at Sekou-Toure Methadone Clinic. A significant portion of patients (38.1%) reported experiencing severe psychological issues, while 29.1% reported mild issues, and 32.7% reported none. To manage cravings or urges to use heroin, 41.7% sought support from others, 35.4% engaged in other activities, 17.5% were unsure of their approach, and 5.4% used coping strategies. Counseling engagement was also notable, with 52.9% attending occasionally, 30.5% regularly, and 16.6% not engaging at all. These findings highlight the need for integrated psychological support and counseling services to enhance treatment adherence.
The treatment environment significantly affects adherence to Opioid Agonist Treatment (OAT) at Sekou-Toure Methadone Clinic. Regarding the health facility’s environment, 33.6% of patients found it neutral, 25.6% described it as supportive but needing improvement, 22.9% considered it unsupportive, and 17.9% viewed it as very supportive and welcoming. Privacy during treatment was another key factor, with 39.0% indicating they had adequate privacy sometimes, 23.8% stating they always had privacy, and 37.2% reporting a lack of privacy. These findings underscore the importance of creating a more welcoming and private treatment environment to foster greater adherence among patient (Table 4).
Comparison of dropout and adhered participants
3.5
A comparison of dropout participants and those who adhered to methadone treatment based on similar characteristics (Table 5).
Discussion
4
Dropout rate
4.1
The dropout rate of 37.9% observed in this study among patients with heroin dependence undergoing Opioid agonist treatment (OAT), at Sekou-Toure Regional Referral Hospital is a concerning finding, with a higher proportion of male patients discontinuing treatment. This is consistent with global trends indicating that male drug patients are generally more likely to drop out of treatment compared to females, possibly due to various factors such as social stigmas or greater impulsivity (4). Moreover, the dropout rate in this study aligns with findings from a study conducted in Tanzania, where dropout rates in OAT programs ranged from 30% to 40% (5). These results highlight the challenges faced by OAT programs in retaining participants, especially males, and underscore the need for more targeted strategies to engage this population.
The social demographics of the dropout patients in this study revealed that the majority were male (97.4%), and many had limited educational backgrounds, with 47.7% having only primary education. These findings are consistent with previous studies that indicate a higher dropout rate among individuals with lower educational attainment, as they may face more significant socio-economic challenges (6). Additionally, the marital status of dropouts showed that the majority were single (52.9%), which could suggest a lack of strong family support, which is often a key factor in the successful continuation of addiction treatment (7). These demographic factors emphasize the importance of tailoring OAT interventions to address the specific needs of individuals with lower education levels and those lacking strong familial support.
Factors for adherence to OAT
4.2
Personal motivations and beliefs emerged as significant factors influencing adherence to OAT. Clients in this study reported that their primary goals were to improve health, maintain sobriety, and reunite with family. These goals align with findings from studies in other regions, which show that health improvement and family reunification are common motivators for individuals seeking treatment for substance use disorders (8). Interestingly, a substantial proportion of patients (26.5%) reported being very confident in adhering to treatment, while 16.6% were very unconfident, suggesting that confidence in treatment outcomes plays a critical role in whether patients remain in treatment (9). The perceived effectiveness of OAT also varied, with 46.6% finding it effective or very effective, highlighting the need for continuous reinforcement of the benefits of OAT to maintain motivation.
Social support was another key factor impacting adherence. The majority of patients in this study reported moderate or weak support networks, with 25.6% indicating no support at all. Research has shown that social support is one of the strongest predictors of treatment adherence in substance use disorders (10). In this study, patients who had strong family or peer support were more likely to stay in treatment, consistent with findings from studies that emphasize the importance of a supportive environment for individuals in OAT (11). However, a significant number of patients experienced inadequate privacy, which could contribute to a lack of trust and further discourage adherence to treatment. A more private and confidential treatment environment could therefore be crucial in improving retention rates.
Finally, the treatment environment itself played a role in adherence. While 33.6% of patients viewed the facility as neutral, 25.6% felt that it was supportive but could be improved, and 22.9% described it as unsupportive. These findings are in line with research that highlights the importance of a welcoming and supportive treatment environment in ensuring the success of OAT programs (12–14). The absence of adequate privacy for 37.2% of patients is particularly concerning, as privacy is a significant factor in patients’ comfort and trust in the treatment process. Enhancing privacy and creating a more welcoming environment could potentially improve both retention and overall treatment outcomes for patients undergoing OAT at this facility.
Study limitation
4.3
While this study provides valuable insights into the dropout rates and adherence factors in methadone-assisted treatment, several limitations should be considered, such as;
Limited generalizability as the study was conducted at a single treatment center and the findings may not be fully generalized to other regions healthcare settings, Potential confounding factors as variables such as mental health status and co-occurring substance use disorders where not controlled for in-depth which may have influenced adherence rates and incomplete records as some participants records may have been missing affecting the comprehensiveness of the dataset.
Recommendations
4.4
To improve adherence and reduce dropout rates in OAT programs, it is recommended that interventions focus on enhancing social support networks, particularly for patients with limited family support or lower educational attainment. Tailored strategies should be implemented to address male patients’ specific needs, including increasing their confidence in treatment and emphasizing the effectiveness of OAT. Furthermore, the treatment environment should be improved by ensuring adequate privacy and a more supportive, welcoming atmosphere. Regular psychological counseling and stronger provider support could also play a crucial role in improving retention. Additionally, further research is necessary to explore the underlying causes of low confidence and the perceived ineffectiveness of OAT in this context.
Conclusion
4.5
The findings of this study highlight significant factors influencing adherence and dropout rates among patients with heroin dependence undergoing Opioid agonist treatment (OAT), at Sekou-Toure Regional Referral Hospital. A dropout rate of 37.9% was observed, with male patients and those with lower educational levels being more prone to discontinuing treatment. Personal motivations such as improving health and maintaining sobriety, along with social support, psychological factors, and treatment environment, were all found to significantly impact treatment adherence. These findings are consistent with global research, underscoring the complexity of factors contributing to both successful treatment retention and dropout in OAT programs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1W.H.O . World Drug. In: Report Vienna, Austria: United Nations Office on Drugs and Crime (UNODC) City. (2023).
- 2Damas AM Jessie.KM Sheryl.M Frank.AM Pamela.AK . Twelve-month treatment retention and associated factors: A Comparison of 2 Medically assisted therapy clinics in Dar-es-Salaam, Tanzania. J Addict Med. (2022) 16:e 382–9. 10.1097/ADM.000000000000099535678425 · doi ↗ · pubmed ↗
- 3Lambdin BH Masao F Chang O Kaduri P Mbwambo J Magimba A . Methadone treatment for HIV prevention—feasibility, retention, and predictors of attrition in Dar-es-Salaam, Tanzania: a retrospective cohort study. Clin Infect Dis. (2014) 59:735–42. doi: 10.1093/cid/ciu 382, PMID: 24855149 PMC 4809981 · doi ↗ · pubmed ↗
- 4Mkumbo M Mwaisobwa A Salum T . Assessment of factors influencing retention and dropout among patients in methadone-assisted treatment in Tanzania. Eas Afr J Public Health. (2018) 15:165–70.
- 5Gowing L Ali R White JM . Evidence for the effectiveness of methadone maintenance treatment in the management of opioid dependence. Addiction. (2009) 104:1781–92.
- 6Al-Turki K Al-Busaidi I Al-Dubai SA . The role of family support in the recovery of drug addicts: A literature review. Int J Soc Psychiatry. (2012) 58:532–9.
- 7Dahlin M Falck RS Carlsson B . Motivation for seeking treatment and drug use outcomes in methadone maintenance treatment. J Subst Abuse Treat. (2009) 36:191–9.
- 8Tonigan JS Miller WR Schermer C . Early drinking consequences and self-efficacy as predictors of treatment outcome in alcohol dependence. Addictive Behav. (2010) 35:53–9.