A real-world comparison study of the efficacy of dual-target first-line rescue treatment of human epidermal growth factor receptor 2 positive advanced breast cancer: trastuzumab combined with pertuzumab versus trastuzumab combined with pyrotinib
Liang Zhang, Chao Li, Shubin Song, Fukai Wang, Tingting Ding, Zhengrui Liu, Yuqin Jin, Zhiyong Yu

TL;DR
This study compares two first-line treatments for HER2-positive advanced breast cancer and finds they are similarly effective.
Contribution
The study provides a real-world comparison of two dual-target therapies for HER2-positive breast cancer using a retrospective cohort.
Findings
HPyr and HP showed similar progression-free survival in HER2-positive advanced breast cancer patients.
HPyr benefitted older patients while HP was more effective in younger patients, though differences were not statistically significant.
No significant differences in clinical efficacy were observed between the two regimens in most subgroups.
Abstract
Trastuzumab combined with pertuzumab (HP) is a first-line therapy for advanced breast cancer (ABC). However, trastuzumab combined with pyrotinib (HPyr) could also exert complementary and synergistic effects. Currently, clinical trials directly comparing the effectiveness of the above two treatment approaches are lacking. Herein, a registered single-center, retrospective study (NCT04609540) was caried out. In the present study, patients diagnosed with human epidermal growth factor receptor 2 (HER2)-positive ABC and treated with dual-target first-line rescue treatment at the Shandong Cancer Hospital between January 2018 and February 2023 were included. Patients were assigned to the HP or HPyr treatment groups by the physician-in-charge. The clinical, pathological and prognostic data of all patients were collected and recorded. Among the 89 patients included, 47 received HP, while the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
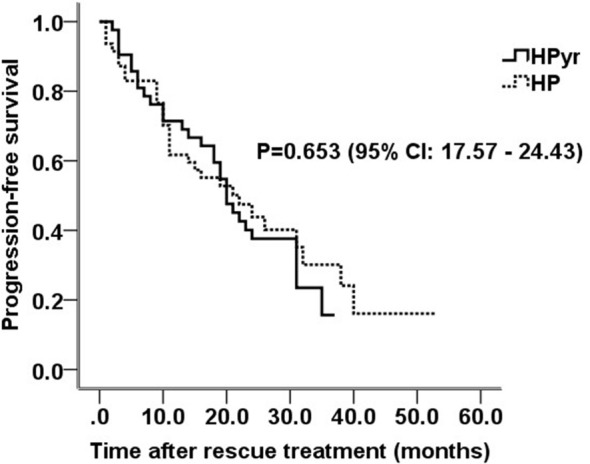 Figure 1
Figure 1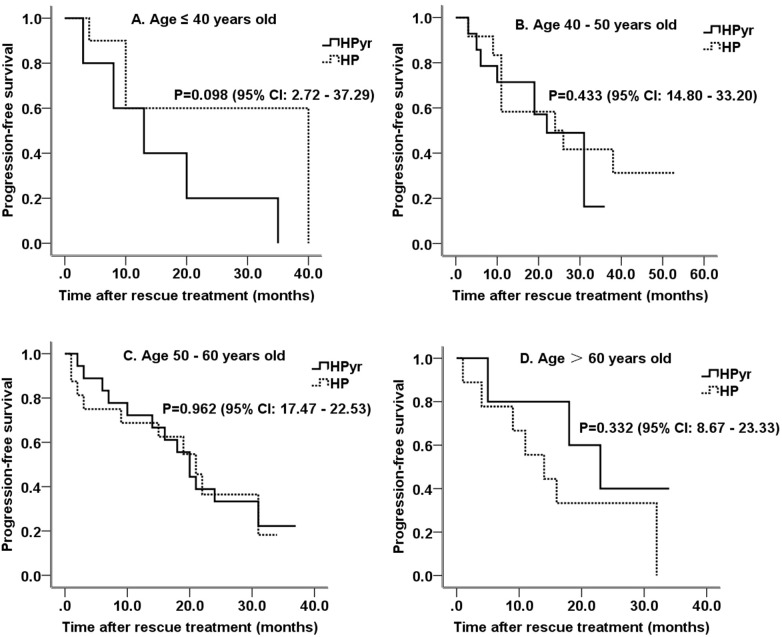 Figure 2
Figure 2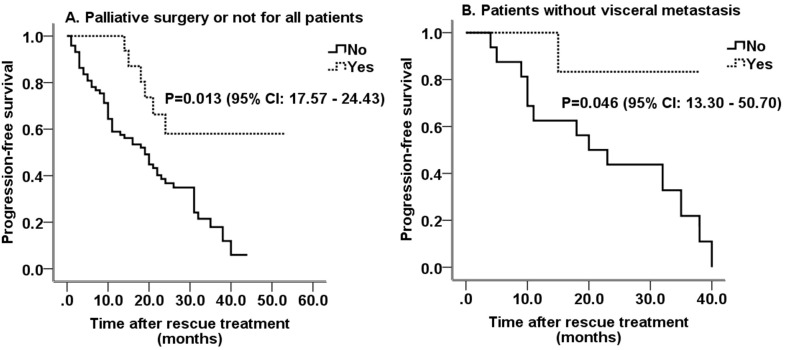 Figure 3
Figure 3| Variable | HP (n=47) | HPyr (n=42) | P value |
|---|---|---|---|
| Family history of cancer | 3 | 6 | 0.011 |
| Onset age | 50.6 (26–75) | 50.2 (31–71) | 0.068 |
| <40 | 10 | 5 | |
| 41-50 | 13 | 15 | |
| 51-60 | 15 | 18 | |
| >60 | 9 | 4 | |
| Primary tumor side | 0.319 | ||
| Left | 24 | 20 | |
| Right | 22 | 22 | |
| Initial diagnosis status | 0.406 | ||
| Advanced stage | 29 | 18 | |
| Early stage | 18 | 24 | |
| Stage I | 0 | 4 | |
| Stage II a | 6 | 3 | |
| Stage II B | 3 | 4 | |
| Stage III A | 4 | 6 | |
| Stage III B | – | – | |
| Stage III C | 5 | 7 | |
| Menstrual status | 0.955 | ||
| Postmenopausal | 27 | 18 | |
| Premenopausal | 20 | 24 | |
| Hormone receptor expression | 0.482 | ||
| Positive | 22 | 18 | |
| Negative | 25 | 24 | |
| Viscera metastases | 33 | 33 | 0.074 |
| Brain metastases | 1 | 9 | <0.001 |
| Liver metastases | 15 | 18 | 0.054 |
| Lung metastases | 24 | 20 | 0.816 |
| Bone metastases | 21 | 17 | 0.440 |
| Palliative surgery | 0.486 | ||
| Yes | 9 | 7 | |
| No | 38 | 35 | |
| Combined therapy | |||
| Initial chemotherapy | 47 | 42 | 0.069 |
| T | 22 | 25 | |
| X | 5 | 7 | |
| N | 3 | 2 | |
| AC-T | 5 | 4 | |
| TCb | 12 | 4 | |
| Maintenance therapy | 43 | 32 | 0.264 |
| X | 19 | 15 | |
| N | 3 | 2 | |
| AI ± OFS | 21 | 15 | |
| Response Evaluation | 0.133 | ||
| Progressive Disease | 30 (63.8%) | 30 (71.4%) | |
| Stable Disease | 4 | 3 | |
| Partial Response | 10 | 7 | |
| Complete Response | 3 | 2 | |
| Survival | 0.295 | ||
| Yes | 43 | 37 | |
| No | 4 | 5 |
| Variable | HP (n=47) | HPyr (n=42) |
|---|---|---|
| Cycles of treatment | Median cycles (range) | Median cycles (range) |
| Docetaxel | 6 (3 – 6) | 6(2 - 6) |
| Nab-paclitaxel (weekly) | 18(6 - 18) | 18(12 - 18) |
| H | 17(2 - 52) | 20.5(3 - 48) |
| P | 17(2 - 52) | |
| Pyr | 20.5(3 - 48) | |
| Adverse Events | ||
| TEAE | 44 | 41 |
| Grade ≥r TEAE | 3 | 14 |
| Drug dose reduction | 2 | 6 |
| Variable | HP (month) | HPyr (month) | P value |
|---|---|---|---|
| Primary tumor side | |||
| Left | 27.1 ± 4.4 | 19.8 ± 2.6 | 0.461 |
| Right | 22.1 ± 3.1 | 22.0 ± 2.6 | 0.834 |
| Initial diagnosis status | |||
| Advanced stage | 23.8 ± 3.5 | 19.2 ± 2.3 | 0.392 |
| Early stage | 22.3 ± 3.9 | 22.0 ± 2.7 | 0.942 |
| Menstrual status | |||
| Postmenopausal | 19.8 ± 2.6 | 21.6 ± 2.3 | 0.838 |
| Premenopausal | 28.7 ± 4.7 | 20.4 ± 2.7 | 0.339 |
| Hormone receptor expression | |||
| Positive | 25.3 ± 3.1 | 19.3 ± 2.7 | 0.158 |
| Negative | 22.2 ± 4.0 | 22.2 ± 2.6 | 0.543 |
| Viscera metastases | 22.0 ± 3.5 | 19.8 ± 2.0 | 0.883 |
| Liver metastases | 21.4 ± 5.0 | 19.4 ± 2.6 | 0.959 |
| Lung metastases | 19.0 ± 3.3 | 17.8 ± 2.4 | 0.919 |
| Bone metastases | 24.7 ± 4.4 | 21.0 ± 2.7 | 0.643 |
| Palliative surgery | |||
| Yes | 33.1 ± 6.7 | 27.4 ± 2.1 | 0.365 |
| No | 20.8 ± 2.5 | 19.1 ± 2.0 | 0.538 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHER2/EGFR in Cancer Research · Advanced Breast Cancer Therapies · Protease and Inhibitor Mechanisms
Introduction
Breast cancer is the most common type of cancer and the most serious death threat for female cancer patients (1). The human epidermal growth factor receptor 2 (HER2) gene was first discovered in 1987 (2). It has been reported that HER2 upregulation accounts for approximately 15-20% of all breast cancer cases, while it is used to predict early recurrence, metastasis, and poor prognosis (3). Currently, targeted treatment strategies for HER2-positive breast cancer include specific monoclonal antibodies, such as trastuzumab and pertuzumab, and tyrosine kinase inhibitors (TKIs), including lapatinib, lenvatinib and pyrotinib.
Trastuzumab is the first monoclonal antibody which specifically binds to the extracellular segment of HER2. It inhibits tumor growth via inhibiting the dimerization of HER2 and other HERs, and is therefore applied to improve the survival of patients for more than 10 years (4). However, due to the development of drug resistance, HER2-positive metastatic breast cancer still threatens the lives of patients due to the development of drug resistance. In recent years, several drug resistance mechanisms, such as impaired drug binding to HER2, constitutive activation of signaling pathways parallel to or downstream of HER2, metabolic reprogramming, and decreased activation of the immune system, have been identified (5).
Pertuzumab, a HER2-directed humanized monoclonal antibody, exerts different binding sites from those of trastuzumab. Pertuzumab inhibits the two main signaling pathways of ligand initiated intracellular signaling, namely mitogen activated protein kinase and phosphoinositol 3-kinase signaling, thus leading to cell growth arrest and apoptosis. Pyrotinib is a pan-HER TKI that targets HER1, HER2, and HER4. It can inhibit tyrosine kinase phosphorylation via irreversibly binding to the ATP binding site on the intracellular tyrosine kinase region, thus blocking subsequent signal transduction (6, 7). Compared with monoclonal antibodies, TKIs have the advantages of multiple targets, low cardiotoxicity, and convenient oral administration (8).
In theory, dual target therapy of trastuzumab combined with pyrotinib (HPyr) is a promising combination for HER2 inhibition, since the underlying mechanisms are different than those previously known. It has been also reported that this regimen is characterized by the lack of adverse reactions. The macromolecule binds to the extracellular HER2 domain, while micromolecular TKIs penetrate the cell membrane to target the HER family’s membrane domain. They complement each other internally and externally.
Currently, trastuzumab combined with pertuzumab (HP) is considered as a first-line rescue treatment strategy for advanced breast cancer (ABC) (9) However, HPyr could achieve complementary and synergistic effects. Nowadays, comparative clinical trial evidence on the effectiveness of HPyr compared with HP is still missing. Therefore, we retrospectively analyzed the efficacy of HP compared with that of HPyr as first-line rescue treatment of patients with HER2-positive ABC patients.
Materials and methods
Inclusion and exclusion criteria
The current single-center, retrospective study included patients, who were diagnosed with HER2-positive ABC and received first-line rescue treatment at the Shandong Cancer Hospital between January 2018 and February 2023. The study was conducted according to the Chinese laws and regulatory requirements. The inclusion criteria were as follows: i. Patients with pathological confirmation of breast cancer, clinically diagnosed as ABC, and without rescue treatment; ii. immunohistochemistry results showing HER2 3+ or HER2 2+ with a positive fluorescence in situ hybridization test; and iii. patients who received HP or HPyr targeted therapy. The exclusion criteria were the following: i. Patients who received targeted therapy other than trastuzumab, pertuzumab or pyrotinib; ii. those who were treated with single targeted therapy; and iii. those who did not receive targeted therapy; or received rescue therapy in the past.
HER2 assessment
HER2 testing was performed using the methodology outlined in the American Society of Clinical Oncology (ASCO)/CAP HER2 testing guidelines. The therapeutic effect of each treatment approach was evaluated using the Response Evaluation Criteria in Solid Tumors (10). Tumor progression was defined as the appearance of new lesions or an increase in tumor diameter (or the sum of all lesion diameters) by more than 20% in imaging compared with the previous examination.
Grouping
Patients were assigned to the HP or HPyr by the supervising physician. In addition, chemotherapy and endocrine treatment strategies were also developed by the supervising physician. The initial dose of trastuzumab was 8mg/kg, followed by 6mg/kg of each 21-day cycle. Patients who were treated with HPyr were given continuous oral pyrotinib at an initial dose of 400 mg once daily. Based on patient tolerance, the dose could be reduced to 320 and 240 mg per day. In the HP group, the initial dose of pertuzumab was 840mg, followed by 420 mg of each 21-day cycle until disease progression. The clinical, pathological, and prognostic data of all patients were collected and recorded in this study. For premenopausal patients, endocrine therapy involves aromatase inhibitors (AIs, including Exemestane, Letrozole, and Anastrozole) in combination with ovarian function suppression (OFS), while for postmenopausal patients, endocrine therapy consists of AIs alone.
Statistical analysis
The SPSS software version 22 (SPSS, Chicago, IL, USA) was used for all statistical analyses. A P value of < 0.05 for a two-sided test was considered statistically significant. Continuous data are expressed as medians and intervals, while categorical ones are expressed as counts and percentages. The therapeutic effect was determined via evaluating progression-free survival (PFS). Survival analysis was calculated by Kaplan-Meier analysis.
Results
Patient characteristics
A total of 89 eligible patients were enrolled, including 47 and 42 patients in the HP and HPyr groups, respectively. All patients were female, with an average onset age of 50.4 years. Except for the family history of cancer and brain metastases, the baseline characteristics were generally well balanced between the two groups (Table 1). Two brain metastases in HPyr group were active, and the other 8 brain metastases in both groups were stable. One patient had bilateral breast cancer. The average and median follow-up time for patients in the HP group was 29.1 ± 11.2 months and 34 months, while that for patients in the HPyr group was 28.6 ± 8.9 months and 35 months.
All patients continued to receive dual-targeted therapy until disease progression. The most common and severe adverse reaction was myelosuppression, which was resolved with supportive care. Although some patients required chemotherapy dose reductions, no treatment was discontinued due to myelosuppression. Other manageable adverse reactions included joint stiffness, limb numbness, nausea, vomiting, and alopecia (Table 2).
HP and HPyr therapy, and PFS
The average PFS time was 23.3 ± 2.0 months, with a median PFS of 21.0 ± 1.8 months. Overall, patients who received HPyr dual-target therapy had a larger progression rate (71.4% vs. 63.8%). However, there was no significant difference in PFS between the HPyr and HP groups (mean PFS, 21.0 ± 1.9 vs. 24.1 ± 2.8 months; P = 0.653; 95% confidence interval (CI), 17.57-24.43; Figure 1). Older patients (>60 years old) who received HPyr therapy showed a longer PFS (22.8 ± 4.9 vs. 16.8 ± 4.2 months; P = 0.332; 95% CI, 8.67-23.33; Figure 2D). Additionally, younger patients (≤ 40 years old) who were treated with HP also displayed a longer PFS (27.4 ± 5.5 vs. 15.8 ± 5.6 months; P = 0.098; 95% CI, 2.72-37.29; Figure 2A). However, statistical significance was not reached. For patients aged 40–50 and 50–60 years, there was no significant difference in PFS between the two groups (P = 0.433; 95% CI, 14.80-33.20 and P = 0.962; 95% CI, 17.47-22.53, respectively; Figure 2B, C). Consistently, PFS efficacy was also achieved in various different subgroups based on the primary tumor side, initial diagnosis status, menstrual status, hormone receptor expression, visceral metastasis site, and whether palliative surgery was performed (Table 3). There was only one patient with brain metastasis in the HP group, and therefore an efficient analysis could not be performed.
Survival curves for all patients in HP and HPyr groups. HPyr, trastuzumab combined with pyrotinib; HP, trastuzumab combined with pertuzumab; CI, confidence interval.
Survival curves of patients in different age brackets. (A) Survival curves for patients ≤40 years old; (B) Survival curves for patients over 40 years old but ≤50 years old; (C) Survival curves for patients over 50 years old but ≤60 years old; (D) Survival curves for patients over 60 years old. HPyr, trastuzumab combined with pyrotinib; HP, trastuzumab combined with pertuzumab; CI, confidence interval.
Palliative surgery and PFS
A total of 16 patients underwent palliative surgery, including nine with visceral metastasis, six with liver metastasis, four with lung metastasis, and five with bone metastasis. No brain metastasis was recorded prior surgery. In addition, patients who underwent palliative surgery showed a significantly longer PFS compared with those who did not (38.6 ± 4.5 vs. 20.1 ± 1.7 months; P = 0.013; 95% CI, 17.57-24.43; Figure 3A). Palliative surgery still improved PFS in patients without visceral metastasis (34.2 ± 3.5 vs. 22.7 ± 3.4; P = 0.046 (34.2 ± 3.5 vs. 22.7 ± 3.4 months; P = 0.046; 95% CI, 13.30-50.70; Figure 3B).
Survival curves of patients underwent palliative surgery or not. (A) Survival curves for all patients underwent palliative surgery or not; (B) Survival curves for patients without visceral metastasis underwent palliative surgery or not. HPyr, trastuzumab combined with pyrotinib; HP, trastuzumab combined with pertuzumab; CI, confidence interval.
Discussion
Compared with single-target therapy, dual-target therapy combined with chemotherapy (with or without endocrine therapy for hormone receptor-positive patients) has been proven to improve the survival of patients in the first-line rescue treatment of HER2-positive ABC and is therefore considered as the standard treatment approach for ABC (11–14). The CLEOPATRA trial (13) showed that docetaxel combined with HP significantly improved overall survival by 15.7 months (56.5 vs. 40.8 months; P<0.001) compared to docetaxel combined with trastuzumab. Additionally, this therapeutic strategy notably extended PFS by 6 months, thus establishing the first-line standard treatment status of the HP regimen.
During the development of HER2-positive ABC, brain metastasis occurs in ~30-50% of patients and is the main cause of treatment failure, thus ultimately leading to shortened survival (15). Compared with macromolecular monoclonal antibodies, micromolecular TKIs, such as pyrotinib, are more likely to penetrate the blood-brain barrier, effectively control brain metastasis, prolong patient survival (8) and improve patient sensitivity to cranial radiation therapy (16). The PERMEATE trial (15) showed that for patients with HER2-positive ABC with brain metastasis, who did not undergo local radiotherapy, pyrotinib combined with capecitabine, yielded a better intracranial objective response rate (74.6%) and median PFS (11.3 months) compared with other agents. The PHENIX (17), PHOEBE (18), and PHILA (19) trials showed that pyrotinib was associated with a good response rate for extracranial lesions and was of practical clinical significance in reducing the risk of brain metastasis and delaying occurrence.
The first-line rescue efficacy of HP compared with that of HPyr has not been previously validated. However, the comparisons of the data between different studies could provide novel insights into the efficacy of these treatment approaches. The PERTAIN trial (20) indicated that the PFS benefit of HP and aromatase inhibitors (AIs) was superior to that of trastuzumab and AIs, particularly for patients not receiving chemotherapy, for whom the median PFS was 22.6 months. However, dual-target therapy did not improve PFS (16.9 vs. 16.9 months) in patients who received induction chemotherapy (21), thus suggesting that HP could only benefit some high-risk patients.
The PHILA trial (19) showed that the median PFS in patients treated with docetaxel combined with HPyr group was 24.3 months, which was significantly better than that in the docetaxel combined with trastuzumab group(PFS, 10.4 months). This was the longest survival without progression in first-line treated HER2-positive ABC patients reported thus far, with an absolute difference of 14 months. This difference was greater compared with the difference of 6 months reported in the CLEOPATRA trial. However, different studies cannot be directly compared. This is also evident from the data on risk ratios. Therefore, the risk ratio in the HPyr combined with docetaxel group was 0.41, while that in the HP combined with docetaxel group was 0.62. The former exerted a numerical advantage. On the other hand, the data from different clinical studies also corroborated each other. The PHILA trial was not the only superior validation study. Moreover, pyrotinib displayed a stable therapeutic effect on HER2-positive breast cancer both as a second-line and late-line treatment (PHOEBE and PHENIX trials), and as a new adjuvant treatment (PHEDRA, NeoATP, and PANPHILA trials).
Currently there is no study to prospectively compare HP vs. HPyr, but the current retrospective study showed that HP was superior for patients <40 years of age, while HPyr was more effective for patients >60 years of age. However, the difference was not significant. In addition, there was no significant difference in the efficacy of the HP and HPyr dual targets for first-line rescue of ABC in the other subgroups. Based on the current medical insurance policy for the treatment of ABC in China, pertuzumab cannot be reimbursed, while pyrotinib is included in the medical insurance reimbursement list. As a domestically produced drug in China that can be reimbursed, pyrotinib is cheaper than pertuzumab and has better treatment accessibility. Furthermore, pertuzumab is administrated through intravenous infusion, while pyrotinib is administered orally. Therefore, the dual-target HPyr is more easily accepted by patients in terms of economy, accessibility and convenience.
Herein, whether palliative surgery was necessary for patients receiving first-line rescue treatment was also analyzed. Therefore, palliative surgery could improve PFS in all patients, including those without visceral metastasis. On the one hand, this difference may be related to the reduction in tumor burden, and on the other hand, the metastasis burden was more limited in patients who underwent surgery. Therefore, for patients with extensive metastasis, the therapeutic value and surgical approach selection of palliative surgery deserve further discussion.
The present study has certain limitations. Most of the comparative results in this study did not show statistical differences, since the number of patients was relatively small. Therefore, the research conclusions require a larger sample size or additional multivariate analysis to be further confirmed and clarified. Herein, a comparison based on brain metastasis could not be performed, since there was only one patient with brain metastasis in the HP group. Rescue chemotherapy and endocrine treatment plans are not unique. This can cause certain interference in the evaluation of therapeutic effects. Due to the short follow-up time, effective overall survival statistical analysis could not be conducted, which was a significant limitation for evaluating the treatment effectiveness in advanced cancer patients. PFS data can provide evidence of “disease control ability” but cannot answer the core question of “whether it prolongs survival.” In addition, as a retrospective study, this study only received feedback from a small number of patients with severe toxic side effects in this regard, and effective statistical analysis could not be performed. Therefore, these findings need to be further clarified in prospective clinical trials. However, there is still a lack of information on whether such clinical trials have been established.
Conclusion
From the retrospective non-randomized small study, HP showed better clinical efficacy as a first-line rescue treatment for ABC in younger patients, while the efficacy of HPyr was numerically better in older patients. Currently, more prospective large-sample studies are needed to further validate our conclusions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660, PMID: 33538338 · doi ↗ · pubmed ↗
- 2Slamon DJ Clark GM Wong SG Levin WJ Ullrich A Mc Guire WL . Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. (1987) 235:177–82. doi: 10.1126/science.3798106, PMID: 3798106 · doi ↗ · pubmed ↗
- 3Wolff AC Hammond ME Hicks DG Dowsett M Mc Shane LM Allison KH . Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. Arch Pathol Lab Med. (2014) 138:241–56. doi: 10.5858/arpa.2013-0953-SA, PMID: 24099077 PMC 4086638 · doi ↗ · pubmed ↗
- 4Cossetti R Tyldesley S Speers C Zheng Y Gelmon K . Comparison of breast cancer recurrence and outcome patterns between patients treated from 1986 to 1992 and from 2004 to 2008. J Clin Oncol Off J Am Soc Clin Oncol. (2015) 33:65–73. doi: 10.1200/JCO.2014.57.2461, PMID: 25422485 · doi ↗ · pubmed ↗
- 5Vernieri C Milano M Brambilla M Mennitto A Maggi C Cona MS . Resistance mechanisms to anti-HER 2 therapies in HER 2-positive breast cancer: Current knowledge, new research directions and therapeutic perspectives. Crit Rev Oncol Hematol. (2019) 139:53–66. doi: 10.1016/j.critrevonc.2019.05.001, PMID: 31112882 · doi ↗ · pubmed ↗
- 6Zhu Y Li L Zhang G Wan H Yang C Diao X . Metabolic characterization of pyrotinib in humans by ultra-performance liquid chromatography/quadrupole time-of-flight mass spectrometry. J Chromatogr B Analyt Technol Bio Med Life Sci. (2016) 1033-1034:117–27. doi: 10.1016/j.jchromb.2016.08.009, PMID: 27541626 · doi ↗ · pubmed ↗
- 7Li X Yang C Wan H Zhang G Feng J Zhang L . Discovery and development of pyrotinib: A novel irreversible EGFR/HER 2 dual tyrosine kinase inhibitor with favorable safety profiles for the treatment of breast cancer. Eur J Pharm Sci. (2017) 110:51–61. doi: 10.1016/j.ejps.2017.01.021, PMID: 28115222 · doi ↗ · pubmed ↗
- 8Xuhong JC Qi XW Zhang Y Jiang J . Mechanism, safety and efficacy of three tyrosine kinase inhibitors lapatinib, neratinib and pyrotinib in HER 2-positive breast cancer. Am J Cancer Res. (2019) 9:2103–19. PMC 683447931720077 · pubmed ↗