Effectiveness and safety of auricular therapy for polycystic ovary syndrome: a systematic review and meta-analysis
Xi Li, Shuang Xu, Liangzhen Xie, Hongying Kuang, Jialing Liu, Yan Li

TL;DR
A study finds that auricular therapy may help manage polycystic ovary syndrome when used with other treatments, but more research is needed.
Contribution
This paper provides a systematic review and meta-analysis of auricular therapy's effectiveness and safety for PCOS.
Findings
Auricular therapy combined with TCM or metformin showed improvements in BMI and anxiety/depression scores.
No significant effects were found on hormonal profiles or metabolic parameters when used alone.
Adjunctive auricular therapy may improve anthropometric and psychological outcomes in PCOS patients.
Abstract
Auricular therapy (AT) has attracted significant interest as a potential treatment for polycystic ovary syndrome (PCOS). A systematic review and a meta-analysis were conducted to evaluate the effectiveness and safety of AT in managing PCOS by analyzing evidence from randomized controlled trials (RCTs). Eight electronic databases were searched from their inception until December 22, 2024. Two independent reviewers performed study screening, data extraction, and quality assessment using the Cochrane Collaboration’s Risk of Bias tool. A random-effects meta-analysis was conducted to synthesize data from included studies using mean differences (MDs). This study was registered with the Open Science Framework (OSF) (DOI: 10.17605/OSF.IO/VBPSM). This systematic review and meta-analysis, which included 18 RCTs involving 1,231 patients with PCOS, found insufficient evidence to support the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
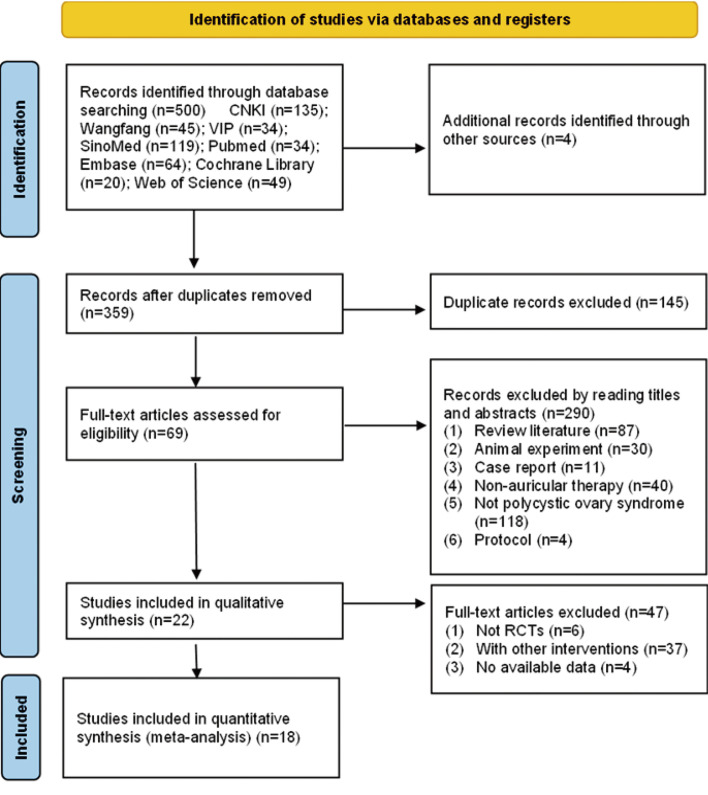 Figure 1
Figure 1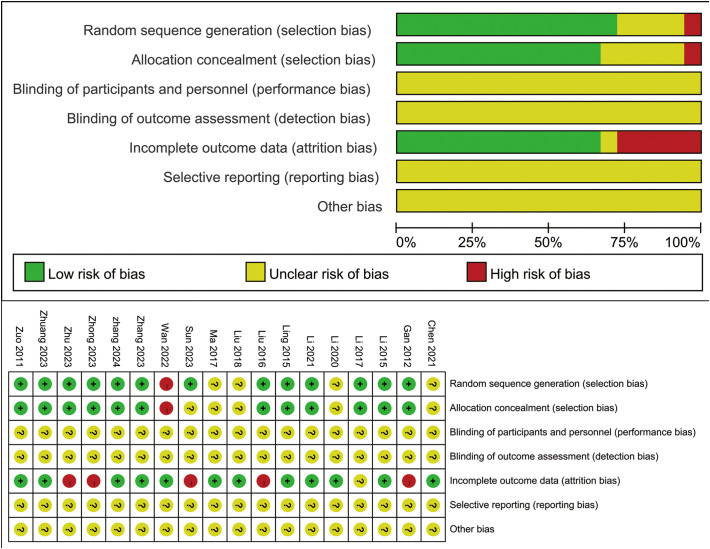 Figure 2
Figure 2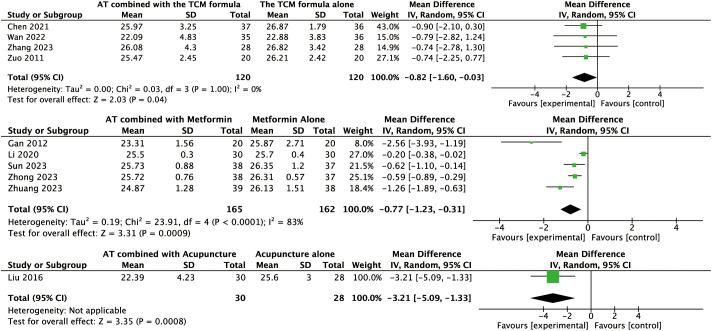 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5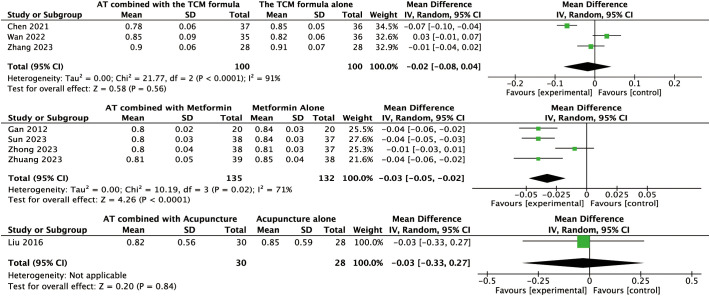 Figure 6
Figure 6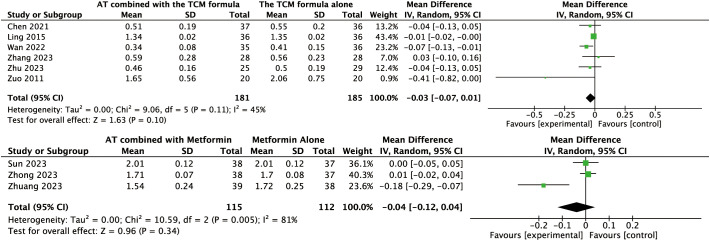 Figure 7
Figure 7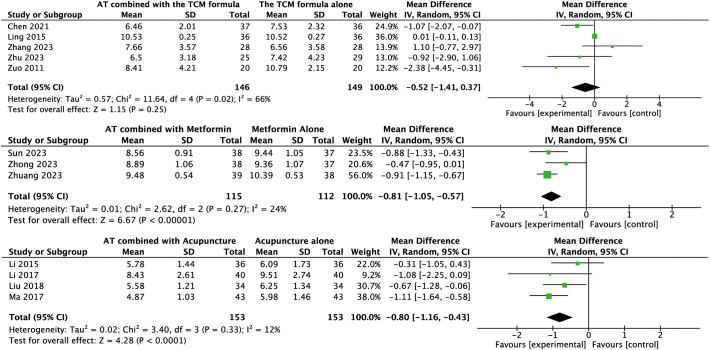 Figure 8
Figure 8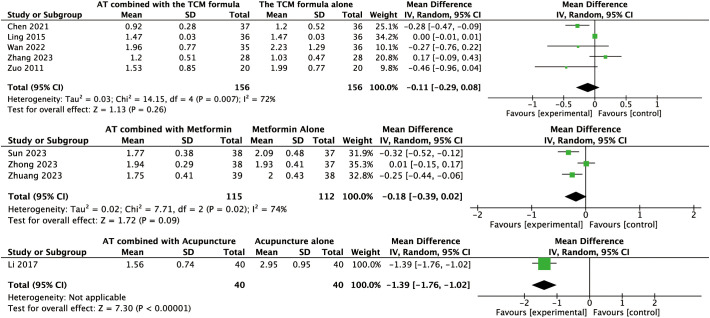 Figure 9
Figure 9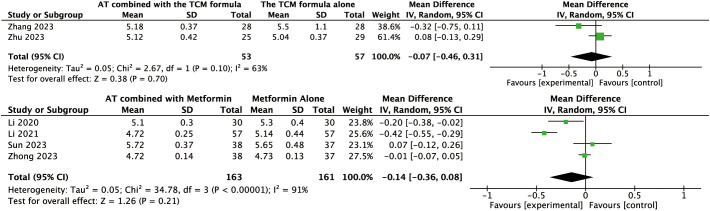 Figure 10
Figure 10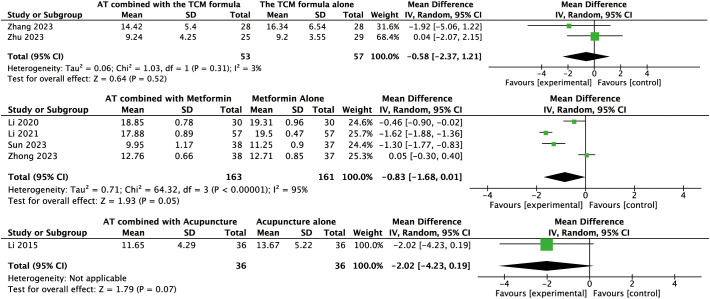 Figure 11
Figure 11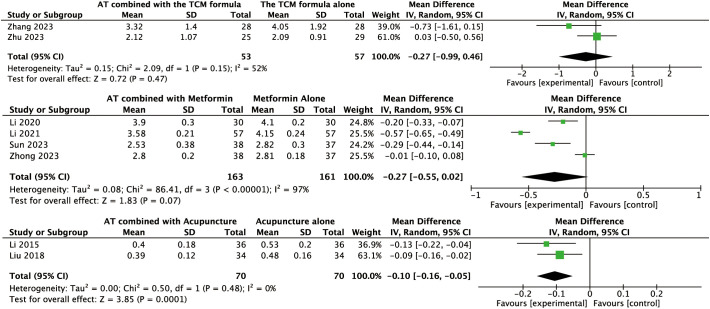 Figure 12
Figure 12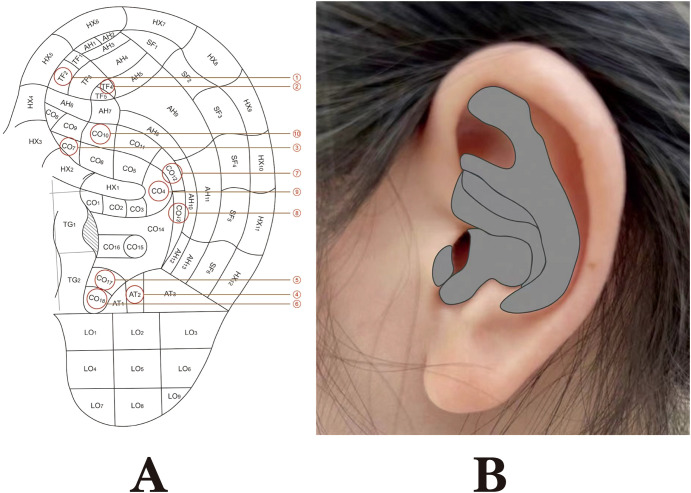 Figure 13
Figure 13 Figure 14
Figure 14| Author (year) | Country | PCOS definition criteria | Sample size (I/C) | Age (years, I/C) | BMI (kg/m², I/C) | Intervention | Control | Duration | Outcome indicators | Adverse reaction |
|---|---|---|---|---|---|---|---|---|---|---|
| Zuo (2011) | China | Rotterdam | 20/20 | 23.80 ± 4.56/24.50 ± 4.37 | 27.77 ± 2.42/28.00 ± 2.41 | AT, 3 times/d + TCMF | TCMF, 2 times/d | 3mth | ①③④⑤ | None |
| Ling (2015) | China | Rotterdam | 36/36 | NM/NM | NM/NM | AT, 3 times/d + TCMF | TCMF, 2 times/d | 3mth | ③④⑤ | None |
| Chen (2021) | China | CMA | 37/36 | 27.78 ± 4.52/28.06 ± 4.27 | 28.63 ± 3.51/27.92 ± 2.17 | AT, 3 times/d + TCMF | TCMF, 2 times/d | 3mth | ①②③④⑤ | None |
| Wan (2022) | China | CMA | 35/36 | 26.43 ± 4.47/25.75 ± 4.83 | 22.56 ± 5.27/23.29 ± 2.11 | AT, 2 times/d + TCMF | TCMF, 2 times/d | 3mth | ①④⑤ | None |
| Zhang (2023) | China | Rotterdam | 28/28 | 27.46 ± 4.24/28.49 ± 3.40 | 27.51 ± 3.94/27.80 ± 3.19 | AT, 3 times/d + TCMF | TCMF, 2 times/d | 3mth | ①②③④⑤⑥⑦⑧⑨⑩ | None |
| Zhu (2023) | China | Rotterdam | 25/29 | 28.70 ± 3.71/28.00 ± 4.16 | 21.37 ± 1.91/21.61 ± 1.82 | AT, 3 times/d + TCMF | TCMF, 2 times/d | 6mth | ③⑤⑥⑦⑧⑨⑩ | None |
| Gan (2012) | China | Rotterdam | 20/20 | NM/NM | NM/NM | AT, 3 times/d + MET | MET 500 mg, 3 times/d | 3mth | ①② | NM |
| Li (2020) | China | Rotterdam | 30/30 | 29.70 ± 2.60/29.50 ± 2.40 | 26.30 ± 1.10/26.20 ± 1.00 | AT, 3 times/d + MET | MET 500 mg, 3 times/d | 3mth | ①⑥⑦⑧ | NM |
| Li (2021) | China | CMA | 57/57 | 31.42 ± 3.22/31.48 ± 3.25 | NM/NM | AT, 3 times/d + MET | MET 500 mg, 3 times/d | 3mth | ⑥⑦⑧ | NM |
| Sun (2023) | China | CMA | 38/37 | 30.63 ± 4.22/30.89 ± 3.84 | 28.27 ± 1.28/27.94 ± 1.28 | AT, 4 times/d + MET | MET 500 mg, 3 times/d | 3mth | ①②③④⑤⑥⑦⑧ | None |
| Zhong (2023) | China | CMA | 38/37 | 15.89 ± 1.72/15.97 ± 1.50 | 26.95 ± 0.63/27.19 ± 0.55 | AT, 4 times/d + MET | MET 500 mg, 3 times/d | 3mth | ①②③④⑤⑥⑦⑧ | None |
| Zhuang (2023) | China | CMA | 39/38 | 16.03 ± 1.81/15.92 ± 1.67 | 28.31 ± 1.61/28.24 ± 1.55 | AT, 4 times/d + MET | MET 500 mg, 3 times/d | 3mth | ①②③④⑤ | None |
| Li (2015) | China | Rotterdam | 36/36 | 36.44 ± 3.11/36.89 ± 4.19 | 23.92 ± 4.19/23.78 ± 5.12 | AT, 3-5 times/d + EA | EA, 1 time/W | 1mth | ③⑦⑧ | NM |
| Liu (2016) | China | Rotterdam | 30/28 | NM/NM | 29.52 ± 3.73/28.31 ± 2.47 | AT, 2 times/d + EA | EA, 1 time/2d | 3mth | ①② | NM |
| Li (2017) | China | Rotterdam | 40/40 | 27.00 ± 8.00/28.00 ± 7.00 | NM/NM | AT, 4 times/d + MA | MA, 1 time/2d | 3mth | ③④ | None |
| Ma (2017) | China | NM | 43/43 | 35.53 ± 5.18/35.53 ± 5.18 | 24.53 ± 4.49/24.19 ± 4.57 | AT, 3-5 times/d + EA | EA, 1 time/W | 1mth | ③ | NM |
| Liu (2018) | China | NM | 34/34 | 35.49 ± 4.26/35.44 ± 4.98 | 24.23 ± 4.66/24.15 ± 4.83 | AT, 3-5 times/d + EA | EA, 1 time/W | 1mth | ③⑧ | NM |
| Zhang (2024) | China | CMA | 30/30 | 28.99 ± 3.58/29.59 ± 3.76 | 26.06 ± 3.08/26.21 ± 3.25 | AT, 1 time/2d + LM | LM | 3mth | ①⑥⑦⑧⑨⑩ | None |
| Auricular acupoint (corresponding to GB standard number) | Frequency of application | References |
|---|---|---|
| CO11 (Uterus) | 13/19 | Chen S Y 2021, Ling W 2015, Wan X 2022, Zhang W F 2023, Zuo J 2011, Gan L 2012, Li Y C 2020, Li Y C 2021, Li L N 2015, Li Q Q 2017, Liu H J 2016, Liu Y 2018, Ma J J 2017 |
| TG2 (Endocrine) | 12/19 | Chen S Y 2021, Ling W 2015, Zhang W F 2023, Zhu S Q 2023, Gan L 2012, Li Y C 2020, Li Y C 2021, Li L N 2015, Li Q Q 2017, Liu H J 2016, Liu Y 2018, Ma J J 2017 |
| CO9 (Kidney) | 12/19 | Chen S Y 2021, Ling W 2015, Wan X 2022, Zhu S Q 2023, Zuo J 2011, Gan L 2012, Li Y C 2020, Li Y C 2021, Sun J G 2023, Zhong L 2023, Zhuang M D 2023, Li L N 2015, Li Q Q 2017, Liu H J 2016, Ma J J 2017 |
| CO4 (Liver) | 10/19 | Chen S Y 2021, Ling W 2015, Zhang W F 2023, Zhu S Q 2023, Li Y C 2021, Sun J G 2023, Zhong L 2023, Zhuang M D 2023, Li Q Q 2017, Liu H J 2016 |
| CO10 (Spleen) | 10/19 | Chen S Y 2021, Ling W 2015, Zhang W F 2023, Zuo J 2011, Gan L 2012, Li Y C 2020, Li Y C 2021, Sun J G 2023, Zhong L 2023, Zhuang M D 2023, Li Q Q 2017, Liu H J 2016 |
| AT4 (Subcortex) | 8/19 | Chen S Y 2021, Ling W 2015, Zhang W F 2023, Zhu S Q 2023, Li Y C 2021, Sun J G 2023, Zhong L 2023, Liu H J 2016 |
| CO12 (Ovary) | 8/19 | Ling W 2015, Wan X 2022, Zhu S Q 2023, Zuo J 2011, Gan L 2012, Li Y C 2020, Li Y C 2021, Li L N 2015, Li Q Q 2017, Liu H J 2016, Liu Y 2018, Ma J J 2017 |
| CO13 (Stomach) | 5/19 | Zhang W F 2023, Sun J G 2023, Zhong L 2023, Zhuang M D 2023, Liu H J 2016 |
| TF4 (Shenmen) | 4/19 | Zhang W F 2023, Zhu S Q 2023, Gan L 2012, Liu H J 2016 |
| TG3 (Hypothalamus) | 4/19 | Wan X 2022, Li L N 2015, Li Q Q 2017, Liu Y 2018, Ma J J 2017 |
| LO1 (Hunger Point) | 4/19 | Gan L 2012, Li Y C 2020, Li Y C 2021, Sun J G 2023, Zhong L 2023, Zhuang M D 2023 |
| CO17 (Sanjiao) | 4/19 | Gan L 2012, Li Y C 2020, Li Y C 2021, Li Q Q 2017 |
| TG1 (Pituitary Gland) | 3/19 | Wan X 2022, Li L N 2015, Ma J J 2017 |
| CO11 (Internal Genitalia) | 3/19 | Sun J G 2023, Zhong L 2023, Zhuang M D 2023 |
| HX5 (Edge of Tragus) | 2/19 | Zhang W F 2023, Zhu S Q 2023 |
| CO7 (Large Intestine) | 2/19 | Li Y C 2020, Li Y C 2021 |
| AT3 (Brain Point) | 1/19 | Liu H J 2016 |
| Bilateral Auricular Concha | 1/19 | Zhang S K 2024 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian function and disorders · Olfactory and Sensory Function Studies · Acne and Rosacea Treatments and Effects
Introduction
The global prevalence of polycystic ovary syndrome (PCOS) among women of reproductive age reportedly ranges from 6% to 25% (1, 2), with the current prevalence in China reaching 7.8%, representing a 65% increase over the past decade (3). This rising trend highlights the growing public health burden associated with PCOS and underscores the urgent need for effective management strategies (4–6).
Current treatments for PCOS primarily focus on symptom management (7). However, the chronic nature of PCOS and the potential for adverse effects associated with these treatments highlight the ongoing need for complementary therapies that may offer improved patient well-being and long-term adherence (8–11).
In recent years, complementary and alternative therapies, such as herbal medicine (12), mind–body interventions including yoga and meditation (13, 14), acupuncture (15), and auricular therapy (AT) (16), have gained increasing research attention as approaches for managing PCOS. Notably, the 2018 and 2023 International Evidence-Based Guidelines report marked variation in care and low-to-moderate certainty of evidence for many interventions, highlighting the need for further rigorous evaluation of adjunctive, patient-centered strategies that may address metabolic risk and psychological well-being (6, 17).
AT, which involves stimulating specific points on the ear, has a long history in traditional Chinese medicine (TCM) and is now being investigated within a modern scientific framework (18). The French physician Paul Nogier first proposed the “inverted fetus” somatotopic map of the auricle in the 1950s, which laid the foundation for the standardization and global dissemination of AT (19, 20). It is now understood that the auricle is the area on the body surface that reflects the vagus nerve (VN), suggesting that AT may exert its therapeutic effects through vagal modulation, a mechanism increasingly recognized for its role in regulating metabolic and endocrine function (18, 21). Its mechanisms of action are believed to involve modulation of the autonomic nervous system and interactions with the neuroendocrine and neuroimmune systems (22–24).
Clinically, AT is commonly used as an umbrella term for interventions that stimulate auricular points, including auricular acupuncture and auricular acupressure (e.g., ear seeds or press pellets). Such modalities have been reported in PCOS-related trial protocols (25) and described in recent TCM consensus documents (26). In parallel, transcutaneous auricular vagus nerve stimulation (ta-VNS), which targets auricular regions innervated by the VN, has been explored as a neuromodulatory approach with potential relevance to the endocrine–metabolic and psychological features of PCOS, prompting further investigation into auricular-based interventions (18).
The potential benefits of AT in PCOS management are multifaceted. It has been investigated for its ability to regulate sex hormone levels (27, 28), improve insulin resistance (IR) (25), and alleviate associated symptoms such as weight gain (29) and depression (30). Beyond its therapeutic effects on these key outcomes, AT may offer distinct advantages compared to conventional treatments, such as oral contraceptives and insulin sensitizers, as well as other complementary therapies, including conventional acupuncture. These advantages include a greater safety profile (31, 32), non-invasiveness, and cost-effectiveness (33), which may contribute to improved patient compliance (34) and treatment adherence. While several studies have reported favorable outcomes of AT in treating PCOS (35, 36), the current evidence remains fragmented, and a comprehensive understanding of its efficacy and safety is lacking. Importantly, available RCTs are heterogeneous in intervention implementation and trial contexts, including differences in AT modalities, comparators, and outcome assessments (25, 37), and in some trials AT has been evaluated in combination with other interventions, such as adjuncts to lifestyle management (37) and, in some studies, as an adjunct to pharmacotherapy (38), which complicates interpretation and may contribute to inconsistent findings across outcomes.
However, existing evidence on AT for PCOS remains fragmented and heterogeneous—making it difficult to draw clear conclusions regarding its effectiveness and safety across clinically relevant outcome domains. Moreover, although a protocol for a systematic review of AT in PCOS was published in 2020 (16), an up-to-date quantitative synthesis incorporating the expanding RCT evidence base and summarizing both effectiveness and safety across clinically relevant domains remains warranted.
Therefore, the objective of this systematic review and meta-analysis was to synthesize existing evidence and clarify the effectiveness and safety of AT in treating PCOS, with analyses organized by co-intervention type and outcome domain where appropriate.
Materials and methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 Statement (39). The study protocol was registered prospectively with the Open Science Framework (OSF) (DOI: 10.17605/OSF.IO/VBPSM). Ethical approval was not required for this study.
Eligibility criteria
Studies were considered eligible for inclusion if they met the following criteria:
(a) Study design: Parallel assignment randomized controlled trials (RCTs).(b) Population: Patients diagnosed with PCOS, provided the diagnosis met established criteria, according to those outlined by the 2003 Rotterdam Consensus Workshop of the European Society of Human Reproduction and Embryology and the American Society of Reproductive Medicine (40).(c) Intervention: Studies investigating the use of AT for the management of PCOS, including studies where AT was used as a standalone intervention or as an adjunctive therapy combined with conventional or complementary interventions. The specific AT methods considered were ear-point pressure seeds and electrical stimulation of the auricular VN.(d) Outcome measures: Trials that provided sufficient data for effect size estimation in the meta-analysis regarding clinical, hormonal, or metabolic outcomes.
The exclusion criteria were as follows: (a) non-randomized studies, animal studies, reviews, protocols, case reports, and conference abstracts. In the case of duplicate studies, the most comprehensive or recent version was selected; (b) women with other underlying conditions, such as congenital adrenal hyperplasia, Cushing’s syndrome, thyroid hormone abnormalities, hyperprolactinemia, ovarian/adrenal tumors, or any severe medical, neurological, or psychiatric conditions, were excluded.
Data sources and search strategy
Two reviewers (XL and SX) independently performed a comprehensive search of the following electronic databases from their inception until December 22, 2024: PubMed, Embase, Web of Science, the Cochrane Library, China National Knowledge Infrastructure (CNKI), Wanfang Database, China Science and Technology Journal Database (VIP), and the Chinese Biomedical Literature Database (CBM). The searches were conducted without language restrictions. The search strategies were developed using a combination of keywords and controlled vocabulary (e.g., Medical Subject Headings (MeSH) in PubMed and Emtree in Embase) where available.
The detailed search strategy for PubMed was as follows:
“Ear acupuncture”[MeSH Terms] OR “auricular acupuncture”[MeSH Terms].“ear”[tiab] OR “ear acupuncture”[tiab] OR “auricular therapy”[tiab] OR “auricular acupuncture”[tiab] OR “auricular acupressure”[tiab] OR “auricular acupoints”[tiab] OR “auricular point-sticking”[tiab] OR “auricular point pressing with bean”[tiab].#1 OR #2.“Polycystic ovary syndrome”[MeSH Terms] OR “Stein–Leventhal Syndrome”[MeSH Terms].“Polycystic ovary syndrome”[tiab] OR “polycystic ovarian syndrome”[tiab] OR “Stein–Leventhal syndrome”[tiab] OR “polycystic ovary disease”[tiab] OR “syndrome and polycystic ovary”[tiab] OR “PCOS”[tiab].#4 OR #5.#3 AND #6.
The complete search strategies for each database are provided in Supplementary Material S1.
Selection process
Two reviewers (XL and SX) independently screened titles and abstracts for eligibility and performed deduplication using EndNote 2025. Full texts of the selected studies were then reviewed, and reasons for exclusion were systematically documented. Disagreements between the two reviewers were resolved by discussion and consensus. If no consensus could be reached, a third reviewer (YL) was consulted. The study selection process is illustrated in Figure 1.
Literature screening process and results.
Data collection
Two reviewers (XL and SX) independently extracted the following parameters from each included study: basic information (first author, publication year, and country), participant characteristics (region, sample size, mean age, and body mass index (BMI)), PCOS diagnostic criteria, AT characteristics (method, frequency, and duration), control treatment characteristics (method, frequency, and duration), clinical outcome parameters, and safety outcomes including adverse events. Any disagreements were resolved through discussion and consensus or, if necessary, by consulting with a third reviewer (YL). In cases where information was missing or unclear, attempts were made to contact the corresponding authors via email. Since no responses were received, all analyses were conducted based on the available published data.
Risk of bias assessment
Two reviewers (XL and SX) independently assessed the risk of bias in the included studies using the Cochrane Risk of Bias tool (RoB 2.0) for randomized trials, as recommended in the Cochrane Handbook for Systematic Reviews of Interventions (version 6) (41). The following seven domains were evaluated: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other sources of bias. Each domain was rated as having a low, high, or unclear risk of bias. Discrepancies between the reviewers were resolved through discussion and consensus with a third reviewer (YL).
Statistical analysis
We conducted all meta-analyses following the statistical methods outlined in the Cochrane Handbook for Systematic Reviews of Interventions (version 6). A random-effects model was prespecified as the primary analytical approach for all outcomes to account for anticipated clinical and methodological heterogeneity across studies (e.g., differences in AT protocols, co-interventions, and treatment durations) using Review Manager (RevMan, version 5.3). This approach was applied irrespective of the observed magnitude of statistical heterogeneity. Statistical significance was defined as two-tailed P ≤0.05.
Continuous variables were summarized as mean differences (MDs) with 95% confidence intervals (CIs) or standardized mean differences (SMDs) with 95% CIs for outcomes measured using different scales. Categorical variables were reported as risk ratios (RRs) with 95% CIs; odds ratios (ORs) were used as an alternative when the event rates were low.
Statistical heterogeneity was assessed using chi-square test (with P < 0.10 indicating statistical significance) and the I² statistic. I² values were interpreted as follows: 0%–40% represented low heterogeneity, 30%–60% moderate heterogeneity, 50%–90% substantial heterogeneity, and 75%–100% considerable heterogeneity. When I² values were close to 0%, fixed-effect and random-effects models are mathematically equivalent and yield nearly identical pooled estimates; therefore, the use of a random-effects model in such cases does not materially influence the direction or magnitude of the results, as discussed in methodological guidance comparing fixed- and random-effects models (42). Consistent results were observed when fixed-effect models were applied as sensitivity analyses (Supplementary Figure 1).
To explore potential sources of heterogeneity and further evaluate the effects of AT on PCOS, subgroup analyses (e.g., based on specific AT methods, control interventions, or treatment durations) were performed. Publication bias was assessed using funnel plots for outcomes with at least 10 included studies, with Egger’s or Begg’s tests conducted as appropriate. We also performed sensitivity analyses to examine the robustness of the findings by removing one study at a time and restricting the analysis to studies with a low risk of bias. Forest plots were constructed to visualize the magnitude and direction of treatment effects.
Assessment of the certainty of the evidence using the GRADE approach
The certainty of the evidence for all outcomes considered critical or important for clinical decision-making was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach, as recommended by the GRADE Working Group (43).
Two reviewers (XL and SX) independently assessed the certainty of evidence for each outcome. The certainty was initially considered “high” and subsequently downgraded based on evaluations in five key domains: risk of bias (as assessed by RoB 2.0), inconsistency (heterogeneity), indirectness, imprecision, and publication bias. Any disagreements between the two reviewers were resolved through consensus or, if necessary, by consulting a third reviewer (YL). The overall certainty of the evidence for each outcome was ultimately classified as high, moderate, low, or very low. The results, including the estimated effects and their corresponding certainty ratings, are summarized in the Summary of Findings (SoF) tables.
Results
Study selection
The study selection process is illustrated in Figure 1. A systematic search identified 504 studies, of which 359 remained after duplicates were removed. During screening of titles and abstracts, 69 studies were deemed potentially relevant, and their full texts were retrieved for further assessment. Subsequently, a total of 47 studies were excluded for the following reasons: non-RCTs (n = 6), failure to meet the intervention criteria (n = 37), and lack of outcome data (n = 4). In total, 18 RCTs met the eligibility criteria and were included in the systematic review and meta-analysis.
Study characteristics
The primary characteristics of the included studies are summarized in Tables 1, 2 provides a summary of auricular acupoint application in the included studies. This systematic review included 18 RCTs (1,231 participants) from mainland China, published between 2011 and 2024. The mean age of participants ranged from 15.89 to 36.89 years, with a mean BMI ranging from 21.37 to 29.52 kg/m² across the studies. Intervention durations ranged from 1 to 6 months.
The studies investigated various intervention types: AT combined with a TCM formula versus a TCM formula alone (n = 6) (44–49), AT plus metformin versus metformin alone (n = 6) (38, 50–54), AT plus acupuncture versus acupuncture alone (n = 5) (55–59), and AT plus lifestyle modification versus lifestyle modification alone (n = 1) (60).
The pre-specified primary outcome was BMI. Secondary outcomes included WHR, LH, LH/FSH ratio, T, FBG, FINS, HOMA-IR, SAS, and SDS. For safety assessments, data on any reported adverse events were systematically extracted and reported.
Assessment of risk of bias
All 18 included studies were RCTs. Regarding bias arising from the randomization process, 12 studies provided details on sequence generation methods (45, 47–57), while the remaining six did not specify their methods. Allocation concealment was not reported in five studies (38, 44, 52, 58, 59), leading to an unclear risk of bias for this sub-domain. For bias due to missing outcome data, five studies reported participant dropouts without providing reasons for all participants, which resulted in a high-risk rating for this domain (48, 50, 52, 53, 57). Information regarding blinding of participants and personnel (related to bias due to deviations from intended interventions) and blinding of outcome assessors (related to bias in measurement of the outcome) was largely absent across all studies. Similarly, details concerning measurement accuracy for objective outcomes or the transparency of selective outcome reporting were insufficient or not reported. Consequently, the risk of bias due to deviations from intended interventions, measurement bias in the outcome, and bias in the selection of reported result domains was generally judged as “unclear” across most studies due to a lack of information. The risk of bias graph and summary are presented in Figure 2.
Quality of bias assessment of the included studies.
Synthesis of results
A total of 18 randomized RCTs, comprising 1,231 women with PCOS, were included in this meta-analysis. The analyses were performed separately for four distinct comparison groups to assess the adjunctive effect of AT. The pooled results for the primary and secondary outcomes are presented below.
Effects of AT combined with the TCM formula versus the TCM formula alone on the primary outcome
Data for this outcome were available from four trials involving 240 women. A random-effects model was applied to the analysis. AT combined with the TCM formula may improve BMI compared to the TCM formula alone (MD: –0.82, 95% CI: –1.60 to –0.03, P = 0.04, I² = 0%, moderate-certainty evidence, Figure 3).
Forest plot displaying the effects of auricular therapy on BMI.
Effects of AT combined with the TCM formula versus the TCM formula alone on secondary outcomes
The pooled analysis revealed that AT combined with a TCM formula could reduce SAS (MD: –3.81, 95% CI: –6.26 to –1.36, P = 0.002, I² = 0%, moderate-certainty evidence, Figure 4) and SDS (MD: –4.22, 95% CI: –7.74 to –0.69, P = 0.02, I² = 41%, moderate-certainty evidence, Figure 5) compared to TCM formula alone.
Forest plot displaying the effects of auricular therapy on SAS.
Forest plot displaying the effects of auricular therapy on SDS.
For other secondary outcomes, the evidence was inconclusive. The analysis showed uncertain effects on WHR (MD: –0.02, 95% CI: –0.08 to 0.04, P = 0.56, I² = 91%, low-certainty evidence, Figure 6) or T levels (MD: –0.03, 95% CI: –0.07 to 0.01, P = 0.10, I² = 45%, moderate-certainty evidence, Figure 7). Similarly, there was no evidence of an effect on LH levels (MD: –0.52, 95% CI: –1.41 to 0.37, P = 0.25, I² = 66%), the LH/FSH ratio (MD: –0.11, 95% CI: –0.29 to 0.08, P = 0.26, I² = 72%), FBG (MD: –0.07, 95% CI: –0.46 to 0.31, P = 0.70, I² = 63%), FINS (MD: –0.58, 95% CI: –2.37 to 1.21, P = 0.52, I² = 3%), or HOMA-IR (MD: –0.27, 95% CI: –0.99 to 0.46, P = 0.47, I² = 52%) (Figures 8, 9, 10–12).
Forest plot displaying the effects of auricular therapy on WHR.
Forest plot displaying the effects of auricular therapy on T.
Forest plot displaying the effects of auricular therapy on LH.
Forest plot displaying the effects of auricular therapy on LH/FSH.
Forest plot displaying the effects of auricular therapy on FBG.
Forest plot displaying the effects of auricular therapy on FINS.
Forest plot displaying the effects of auricular therapy on HOMA-IR.
Effects of AT combined with metformin versus metformin alone on primary outcome
Data for the primary outcome were available from five trials involving 327 women. The pooled results revealed that AT combined with metformin could reduce BMI compared to metformin alone (MD: –0.77, 95% CI: –1.23 to –0.31, P < 0.001, I² = 83%, low-certainty evidence, Figure 3).
Effects of AT combined with metformin versus metformin alone on secondary outcomes
Regarding secondary outcomes, the pooled results revealed that combination therapy could reduce WHR (MD: –0.03, 95% CI: –0.05 to –0.02, P < 0.001, I² = 71%, moderate-certainty evidence, Figure 6) and resulted in a reduction of LH levels (MD: –0.81, 95% CI: –1.05 to –0.57, P < 0.001, I² = 24%, high-certainty evidence, Figure 8). However, there was no evidence of an effect on the LH/FSH ratio (MD: –0.18, 95% CI: –0.39 to 0.02, P = 0.09, I² = 74%, low-certainty evidence, Figure 9), T levels (MD: –0.04, 95% CI: –0.12 to 0.04, P = 0.34, I² = 81%, low-certainty evidence, Figure 7), or FBG levels (MD: –0.14, 95% CI: –0.36 to 0.08, P = 0.21, I² = 91%, low-certainty evidence, Figure 10). Furthermore, we found no clear evidence that the combination therapy affected FINS levels (MD: –0.83, 95% CI: –1.68 to 0.01, P = 0.05, I² = 95%, low-certainty evidence, Figure 11) or HOMA-IR (MD: –0.27, 95% CI: –0.55 to 0.02, P = 0.07, I² = 97%, low-certainty evidence Figure 12).
No data were available to determine the effects of AT combined with metformin on SAS or SDS.
Effects of AT combined with acupuncture versus acupuncture alone on the primary outcome
Data for the primary outcome were available from a single trial involving 58 women. This study revealed that AT combined with acupuncture could reduce BMI compared to acupuncture alone (MD: –3.21, 95% CI: –5.09 to –1.33, P < 0.001, moderate-certainty evidence, Figure 3).
Effects of AT combined with acupuncture versus acupuncture alone on secondary outcomes
Regarding secondary outcomes, the pooled analysis showed that the combination of AT and acupuncture could reduce LH levels (MD: –0.80, 95% CI: –1.16 to –0.43, P < 0.001, I² = 12%, high-certainty evidence, Figure 8) and HOMA–IR (MD: –0.10, 95% CI: –0.16 to –0.05, P < 0.001, I² = 0%, high-certainty evidence, Figure 12). A single trial consistently suggested that this combination could reduce the LH/FSH ratio (MD: –1.39, 95% CI: –1.76 to –1.02, P < 0.001, moderate-certainty evidence, Figure 9). However, evidence from a single trial found was uncertain regarding the effect on WHR (MD: –0.03, 95% CI: –0.33 to 0.27, P = 0.84, low-certainty evidence, Figure 6) and found no evidence of an effect on FINS levels (MD: –2.02, 95% CI: –4.23 to 0.19, P = 0.07, low-certainty evidence, Figure 11).
Due to a lack of reported data, the effects of AT on T and FBG levels, as well as on SAS/SDS, remain indeterminate.
One study investigated the effectiveness of auricular VN electrical stimulation combined with lifestyle intervention for improving negative emotions in patients with PCOS. In this study, 60 patients with PCOS were randomized into an intervention group (n = 30) that received both auricular VN electrical stimulation and lifestyle intervention and a control group (n = 30) that received lifestyle intervention alone. Both interventions were administered over a 1-month period. The study reported improvements in the intervention group compared to the control group regarding anxiety (SAS scores) and depression (SDS scores) as well as TCM symptom scores, glucose metabolism indicators (FINS, FBG, and HOMA-IR), and inflammatory markers (IL-1, IL-6, and TNF-α) (all P < 0.05).
Overall risk of bias
The overall risk of bias across the included studies was judged as moderate to high, primarily due to insufficient reporting of key methodological details. Concerns regarding selection bias were noted. Although all 18 studies were described as randomized, six did not specify the method of sequence generation, and five provided no information on allocation concealment, leaving these studies at an unclear risk. A significant deficiency was the universal lack of information on blinding. No study adequately described the blinding of participants, personnel, or outcome assessors. This resulted in a high or unclear risk of performance bias and detection bias across all trials. Attrition bias was a concern in five studies that reported dropouts without providing an adequate explanation for all missing participants, leading to a high-risk judgment in this domain. Finally, insufficient detail regarding selective outcome reporting was a common issue, making it challenging to assess the risk of bias in reporting. Due to this widespread lack of information, many domains were frequently rated as having an “unclear risk of bias”. A detailed summary of the risk of bias assessment for each study is presented in Figure 2.
Reporting biases
The risk of reporting bias was high or unclear across all studies, given that no trial provided evidence of a pre-registered study protocol. The absence of accessible protocols made it challenging to verify whether the reported outcomes were consistent with a predefined analysis plan, raising concerns about potential selective reporting and outcome switching.
The potential for publication bias was also assessed. Due to the small number of studies (<10) in most meta-analyses, the use of funnel plots to detect asymmetry was not feasible for most outcomes. For the few outcomes where analysis was possible, visual inspection of the funnel plots suggested some asymmetry, which may indicate publication bias. However, these findings should be interpreted with caution, as the statistical power to detect true bias was limited.
These identified risks of bias were considered in the GRADE assessment and contributed to the downgrading of the certainty of evidence for several outcomes.
Certainty of the evidence
The certainty of the evidence for all outcomes was evaluated using the GRADE approach. The overall certainty ranged from high to low across the comparisons, with downgrading primarily due to serious risk of bias, inconsistency across studies, and potential publication bias.
A comprehensive summary of these GRADE assessments, detailing the reasons for each rating, is presented in the Summary of Findings table (Supplementary Table 1).
Robustness of findings
Sensitivity analyses were performed to assess the robustness of our findings. Despite the methodological limitations identified in the included studies, excluding studies with a high risk of bias did not substantially alter the overall direction or magnitude of the pooled estimates. This finding suggests a certain level of consistency and reliability in the therapeutic effect despite the overall low-to-moderate certainty of the evidence.
Discussion
Emerging evidence highlights PCOS as a neuroendocrine condition (61, 62), with its pathogenesis closely linked to dysregulation of the hypothalamic–pituitary–ovarian (HPO) axis, hypothalamic–pituitary–adrenal (HPA) axis, and, increasingly, autonomic nervous system (ANS) dysfunction (63). This growing recognition of the ANS’ role underscores the complexity of PCOS etiology and suggests that interventions targeting the nervous system may hold therapeutic potential (64–67).
To the best of our knowledge, this systematic review and meta-analysis is the first to systematically evaluate the efficacy and safety of AT for managing PCOS. Given the limited evidence available for AT as a standalone treatment, our analysis focused on AT as an adjunctive therapy combined with other interventions.
Our findings demonstrated that AT, when used in combination with conventional or complementary treatments, showed beneficial effects on anthropometric, hormonal, metabolic, and psychological outcomes. BMI showed improvement across all three intervention groups, while WHR was reduced when AT was combined with metformin. The LH levels were reduced when AT was combined with metformin and acupuncture, and the LH/FSH ratio decreased in the AT combined with acupuncture group. Besides that, HOMA-IR was reduced in the AT combined with acupuncture group. Psychological outcomes, as assessed by SAS and SDS, also showed significant improvement when AT was combined with TCM formulas.
Despite these promising findings, the results of this study should be interpreted with caution. Our analysis revealed several methodological limitations across the included RCTs, which may compromise the reliability and validity of the findings. Specifically, most studies were characterized by small sample sizes, inadequate reporting of key methodological details (such as allocation concealment and blinding), and a high risk of selective reporting bias. These issues were the primary reasons for the downgrading of evidence certainty as assessed by the GRADE approach. Across different outcomes, the certainty of evidence ranged from low to high, reflecting serious concerns regarding risk of bias, inconsistency, and potential publication bias in the primary studies. These factors reduce confidence in the estimated effects of AT for PCOS.
In addition, considerable heterogeneity was observed across the included studies. A random-effects model was employed to minimize its impact, and subgroup and sensitivity analyses were conducted. The subgroup analyses were performed based on different intervention methods, and RCTs with small sample sizes or a high risk of bias were temporarily excluded from the primary analysis to assess the robustness of the findings. The sensitivity analyses indicated that excluding these studies did not substantially alter the overall results; accordingly, they were retained in the final meta-analysis.
Nevertheless, heterogeneity persisted despite these efforts and may be attributed to several factors. Initially, some trials lacked sufficient information on participant characteristics, such as BMI and age, thereby limiting accurate subgroup stratification. Second, repeated subgroup analyses may increase the likelihood of type I errors, potentially leading to false-positive findings. More importantly, substantial heterogeneity was observed in certain outcome comparisons, particularly when AT was combined with different co-interventions—for example, the heterogeneity for BMI outcomes was minimal when AT was combined with the TCM formula (I² = 0%), whereas marked heterogeneity emerged when AT was combined with metformin (I² = 83%). This discrepancy suggests that the observed heterogeneity is likely driven by variations in the co-interventions combined with AT and thus contributes substantially to between-study variability. In addition, the included studies varied considerably in terms of baseline disease severity, intervention duration, concurrent medication use, and specific AT protocols (e.g., auricular acupuncture versus auricular acupressure, stimulation frequency, and point selection). Such heterogeneity in clinical characteristics and trial design may be further amplified in the context of adjunctive therapy. These methodological inconsistencies likely contributed to the observed variability and should be carefully considered when interpreting the findings of this meta-analysis. Moreover, this review included only studies published in Chinese, which may have introduced language and publication bias, thereby limiting the generalizability and strength of the conclusions.
An increasing body of evidence suggests that dysfunction of the ANS, particularly increased sympathetic activity alongside reduced parasympathetic activity, may contribute to PCOS development and progression (64–67). Under normal physiological conditions, the sympathetic and parasympathetic systems operate in a dynamic balance to maintain homeostasis. Disruption of this balance has been associated with various disorders involving autonomic dysregulation, including neurological, metabolic, inflammatory, cardiovascular, and psychiatric conditions (68). Over the years, several studies have indicated that women with PCOS exhibit increased sympathetic activity, and a complex bidirectional relationship may exist between sympathetic overactivity and endocrine or metabolic disturbances (64, 69–71). These observations have led to the hypothesis that therapeutic strategies aimed at reducing sympathetic activity or enhancing parasympathetic function, thereby restoring sympathovagal balance, may be beneficial in managing PCOS-related symptoms (18).
AT integrates the theoretical foundations of TCM with modern neuroanatomical understanding, with its core mechanism believed to involve the stimulation of the auricular branch of the VN (ABVN). The auricle is the peripheral body region innervated by the ABVN (72, 73), as illustrated in Figure 13. It is now understood that the ABVN projects to key nuclei in the brainstem, including the nucleus tractus solitarius (NTS) and the dorsal motor nucleus (DMN) of the vagus, forming the neuroanatomical basis of the auricle–vagal reflex (74). This anatomical arrangement provides a plausible rationale for modulating physiological functions through the targeted stimulation of specific auricular acupoints.
Auricular acupoints and the distribution area of the auricular vagus nerve. (A) Numbers 1 through 10 correspond to the locations of auricular acupuncture points used in the articles, as depicted on the national standard auricular map. Specifically, the auricular points for numbers 1, 2, 3, 4, 5, 6, 7, 8, 9, and 10 are as follows: CO11 (internal genitalia), TF4 (shenmen), CO7 (large intestine), AT4 (subcortex), CO17 (sanjiao), TG2 (endocrine), CO12 (liver), CO13 (spleen), CO4 (stomach), and CO10 (kidney). (B) The gray-shaded area represents the region innervated by the ABVN.
In the context of PCOS, the commonly used auricular points, such as TG2 (endocrine), TF4 (shenmen), CO11 (internal genitalia), and CO10 (kidney), are located within the ABVN-innervated regions of the auricle (75). Details on the selection of auricular acupoints and their frequency patterns when combined with other interventions are provided in Table 2.
The anatomical distribution of the auricular acupoints is depicted in Figure 13. It has been proposed that ta-VNS targeting these regions may activate central vagal pathways, potentially contributing to autonomic regulation and systemic homeostasis (76). Findings from the present meta-analysis suggest that AT, particularly ta-VNS, may play a role in alleviating autonomic dysfunction in PCOS by modulating the ABVN–NTS/DMN axis. While the exact mechanisms remain fully elucidated, preliminary evidence supports the involvement of multiple integrative pathways, warranting further investigation.
From a mechanistic perspective, the therapeutic effects of AT may be mediated through multiple integrative pathways. The underlying schematic diagram is potentially shown in Figure 14.
Potential mechanisms of auricular therapy in treating PCOS via vagal nerve stimulation.
First, AT may modulate the central regulation of ovarian function, thereby improving sex hormone imbalance. Gerendai et al. proposed that a neural circuit may exist between the ovaries and the central nervous system (CNS), whereby the ovaries receive afferent input from the CNS through the superior ovarian nerve (SON), ovarian plexus nerve, and VN and transmit signals back to the CNS through the SON and the celiac–superior mesenteric ganglia, while also responding to afferent vagal input (77, 78). Growing evidence suggests that afferent fibers of the VN may modulate the secretion of gonadotropins by acting on the hypothalamus, thereby modulating hypothalamic control over ovarian function (79, 80). These findings suggest that VNS plays a significant role in regulating ovarian physiology. Although the precise mechanisms by which AT affects ovarian function remain unclear, future studies should explore whether AT modulates the pulsatile secretion of gonadotropin-releasing hormone (GnRH) in the hypothalamus, thereby improving the function of the HPO axis and alleviating the dysregulated LH secretion commonly observed in PCOS.
Second, a key pathophysiological mechanism of PCOS is IR. The VN is widely known to play a vital role in maintaining glucose homeostasis, a process central to IR development. Afferent signals from the ABVN transmit nutritional information to the medulla’s dorsal vagal complex, activating vagal efferent pathways that regulate hepatic gluconeogenesis (81). Furthermore, AT has been shown to improve IR by promoting early-phase insulin secretion and enhancing hepatic insulin sensitivity (82). Therefore, by targeting the vagal pathway, AT may offer a novel approach to directly address IR, a core endocrine abnormality in PCOS.
Third, AT appears to exert anti-inflammatory effects, primarily through the cholinergic anti-inflammatory pathway (CAP) and the splenic sympathetic anti-inflammatory pathway (SSAP) (83–85). There is a growing consensus suggesting that PCOS is characterized by chronic low-grade inflammation, with elevated levels of pro-inflammatory cytokines such as interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and C-reactive protein contributing to IR and metabolic dysfunction (86–88). In the CAP, vagal signaling stimulates enteric neurons to release acetylcholine (ACh), which binds to α7 nicotinic ACh receptors (α7nAChR) on macrophages, thereby downregulating the expression of these PCOS-associated pro-inflammatory cytokines. In the SSAP, vagal modulation of visceral sympathetic nerves promotes ACh secretion from T cells, which similarly acts on α7nAChR to inhibit nuclear factor kappa B signaling, a key pathway in PCOS-related inflammation. By targeting these inflammatory pathways, AT may help break the cycle of inflammation-induced IR and hormonal dysregulation that perpetuates PCOS symptoms.
Fourth, AT may contribute to metabolic regulation and weight management, addressing key pathophysiological features of PCOS. Obesity affects 50%–80% of PCOS patients and exacerbates IR, hyperandrogenism, and reproductive dysfunction. Evidence suggests that AT can reduce postprandial ghrelin levels and suppress appetite, increase basal metabolic rate, and promote visceral fat consumption, effects that target the metabolic dysfunction characteristic of PCOS (89–94).
Fifth, emerging evidence suggests that AT may potentially help alleviate psychological symptoms commonly observed in patients with PCOS, including depression and anxiety, though the underlying mechanisms and clinical efficacy require further investigation. Proposed mechanisms may involve modulation of neural activity and connectivity in depression-related brain regions (95), inhibition of neuroinflammatory sensitization (95), promotion of hippocampal neurogenesis (96), and regulation of the gut–microbiota–brain axis (97).
In summary, AT demonstrates broad therapeutic potential in managing PCOS through its multi-target and multi-mechanism regulatory effects. Its neurophysiological basis provides a preliminary foundation for further clinical application. Although preliminary evidence supports the effectiveness of AT in treating PCOS, the underlying neurobiological mechanisms remain to be fully elucidated. Future studies should systematically investigate the multi-level neural regulatory pathways involved, particularly by utilizing advanced neuroimaging techniques such as functional magnetic resonance imaging and diffusion tensor imaging, to explore how ta-VNS modulates brain networks, neural circuits, and neurotransmitter metabolism.
Future research directions should prioritize two critical domains. First, mechanistic investigations must elucidate whether ta-VNS modulates hypothalamic GnRH pulsatility to restore HPO axis function and normalize LH secretion patterns in PCOS. This hypothesis warrants an investigation of central neuroendocrine pathways and their downstream effects on ovarian function, potentially establishing AT as a precision neuromodulation therapy targeting the core pathophysiology of PCOS.
Second, the standardization and optimization of AT protocols demand immediate attention. Future studies must establish evidence-based parameters, including optimal acupoint selection (e.g., TF4 (shenmen), TG2 (endocrine)), stimulation intensity (typically 2–4 mA for electroacupuncture), frequency specifications (10–100 Hz), treatment duration (20–30 min per session), intervention cycles (8–12 weeks), and maintenance protocols. Besides that, determining patient-specific factors such as BMI-adjusted dosing, phenotype-specific acupoint combinations, and biomarker-guided treatment timing will advance AT toward precision medicine applications.
Indeed large-scale, multicenter RCTs employing these standardized protocols are essential to establish clinical efficacy and safety profiles. These trials should incorporate rigorous dose–response analyses, long-term follow-up assessments, and investigation of AT synergies with conventional PCOS therapies. Such a comprehensive research framework will facilitate AT’s evolution from empirical practice to evidence-based, mechanism-driven therapeutic strategy, ultimately expanding treatment options for diverse PCOS phenotypes.
Conclusions
This systematic review and meta-analysis demonstrated that AT could serve as a beneficial adjunctive treatment for PCOS management. Our findings indicated that AT reduced BMI and improved LH, LH/FSH ratio, HOMA-IR, and anxiety and depression scores. No serious adverse events were reported; however, this finding requires cautious interpretation due to potential underreporting and limited follow-up periods in primary studies.
Several methodological limitations constrain these conclusions, including small sample sizes, heterogeneity in intervention protocols, and limited study duration. These limitations necessitate larger, well-designed RCTs with standardized protocols to establish AT’s long-term efficacy and safety profile in PCOS management.
Future research priorities should include mechanistic investigations of AT’s neuromodulatory pathways, particularly whether transcutaneous VN stimulation modulates hypothalamic GnRH plasticity and the function of the HPO axis. Moreover, standardization of treatment parameters, including optimal acupoint selection, stimulation intensity, frequency, and treatment duration, is essential for clinical translation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Iervolino M Lepore E Forte G LaganàAS Buzzaccarini G Unfer V . Natural molecules in the management of polycystic ovary syndrome (PCOS): an analytical review. Nutrients. (2021) 13. doi: 10.3390/nu 13051677, PMID: 34063339 PMC 8156462 · doi ↗ · pubmed ↗
- 2Mimouni NEH Paiva I Barbotin AL Timzoura FE Plassard D Le Gras S . Polycystic ovary syndrome is transmitted via a transgenerational epigenetic process. Cell Metab. (2021) 33:513–30.e 8. doi: 10.1016/j.cmet.2021.01.004, PMID: 33539777 PMC 7928942 · doi ↗ · pubmed ↗
- 3Yang R Li Q Zhou Z Qian W Zhang J Wu Z . Changes in the prevalence of polycystic ovary syndrome in China over the past decade. Lancet Reg Health West Pac. (2022) 25:100494. doi: 10.1016/j.lanwpc.2022.100494, PMID: 35669932 PMC 9162959 · doi ↗ · pubmed ↗
- 4Joham AE Boyle JA Zoungas S Teede HJ . Hypertension in reproductive-aged women with polycystic ovary syndrome and association with obesity. Am J Hypertens. (2015) 28:847–51. doi: 10.1093/ajh/hpu 251, PMID: 25542625 · doi ↗ · pubmed ↗
- 5Joham AE Norman RJ Stener-Victorin E Legro RS Franks S Moran LJ . Polycystic ovary syndrome. Lancet Diabetes Endocrinol. (2022) 10:668–80. doi: 10.1016/s 2213-8587(22)00163-2, PMID: 35934017 · doi ↗ · pubmed ↗
- 6Teede HJ Misso ML Costello MF Dokras A Laven J Moran L . Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum Reprod. (2018) 33:1602–18. doi: 10.1093/humrep/dey 256, PMID: 30052961 PMC 6112576 · doi ↗ · pubmed ↗
- 7Choudhari R Tayade S Tiwari A Satone P . Diagnosis, management, and associated comorbidities of polycystic ovary syndrome: A narrative review. Cureus. (2024) 16:e 58733. doi: 10.7759/cureus.58733, PMID: 38779261 PMC 11110474 · doi ↗ · pubmed ↗
- 8Cowan S Lim S Alycia C Pirotta S Thomson R Gibson-Helm M . Lifestyle management in polycystic ovary syndrome - beyond diet and physical activity. BMC Endocr Disord. (2023) 23:14. doi: 10.1186/s 12902-022-01208-y, PMID: 36647089 PMC 9841505 · doi ↗ · pubmed ↗