Efficacy and safety of a new cladribine-based conditioning regimen for allogeneic hematopoietic stem cell transplantation in children with relapsed or refractory acute myeloid leukemia
Wen-ting Pei, Chun-lei Liu, Xiao-ling Li

TL;DR
A cladribine-based treatment before stem cell transplants in children with hard-to-treat leukemia showed good results with few side effects and high survival rates.
Contribution
A new cladribine-based conditioning regimen for allogeneic stem cell transplants in pediatric relapsed/refractory AML is evaluated for efficacy and safety.
Findings
All 16 patients achieved successful hematopoietic reconstruction with median neutrophil and platelet engraftment times of 12 and 15 days.
The 1-year overall and disease-free survival rates were 87.5% and 87.4%, with low relapse and non-relapse mortality rates.
Mild regimen-related toxicity and manageable graft-versus-host disease were observed, with few severe complications.
Abstract
Cladribine, a synthetic analog of deoxyadenosine, exhibits potent activity against hematological malignancies. While cladribine-containing regimens combined with allogeneic hematopoietic stem cell transplantation (allo-HSCT) have been proposed as a potential strategy to improve outcomes in relapsed or refractory (R/R) acute myeloid leukemia (AML), additional clinical evidence is needed, particularly in pediatric populations. This single-center retrospective study aimed to describe the efficacy and safety of a cladribine-based conditioning regimen for allo-HSCT in children with R/R AML. Clinical data of 16 children with R/R AML who underwent allo-HSCT following a cladribine-based conditioning regimen at our hospital from October 2020 to June 2024 were analyzed retrospectively. Key outcomes included hematopoietic reconstruction, regimen-related toxicity (RRT), cumulative incidence of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
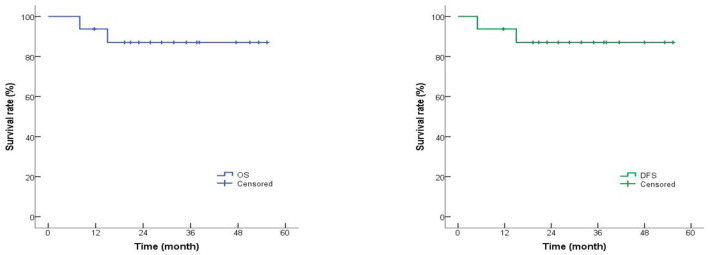 Figure 1
Figure 1|
|
|
|
|---|---|---|
| Matched | CsA + short-course MTX | 2.5 mg/(kg·d) on day 7 pre-transplantation and 3–5 mg/(kg·d) twice daily after hematopoietic reconstruction; MTX: 15 mg/(m2) on d+1, 10 mg/(m2) on d+3, +6, +11 |
| Partially matched | CsA + MMF + anti-CD25 monoclonal antibody | CsA: same as above; MMF: 300 mg/(m2) every 12 h on day 7; anti-CD25 mAb: 20 mg on d+1 and d+4 |
|
|
|
|
|
|
|
|
|
|
|
| |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Female | 15 | 46,XY | KRAS, WT1mutation | <0.01% | 6/12 | PB | 11.53 | 10.32 | 10 | 10 |
| 2 | Female | 9 | 46,XX, t(8;10;21) (q22;q26;q22) [16]/46,XX[4] | RUNX1-RUNX1T1 (+), CEBPA mutation | <0.01% | 10/10 | PB | 9.21 | 7.09 | 14 | 16 |
| 3 | Male | 4 | 46,XY, t(5;11) (q31;p15)[17]/ 46,XY[3] | MLL-AF9 (+) | <0.01% | 8/10 | PB | 8.34 | 6.13 | 13 | 17 |
| 4 | Male | 2 | 45,X,-Y, t(8;21) (q22;q22) | RUNX1-RUNX1T1 (+), PTPN11 mutation | <0.01% | 6/12 | PB | 8.21 | 6.74 | 15 | 21 |
| 5 | Male | 9 | 46,XY, del(11)(q23) | MLL-ENL (+) | <0.01% | 7/12 | BM+PB | 10.13 | 7.16 | 11 | 15 |
| 6 | Male | 11 | 46,XY, t(8;21) (q22;q22) | RUNX1-RUNX1T1 (+), C-KIT mutation | 0.07% | 10/10 | PB | 11.44 | 7.28 | 13 | 14 |
| 7 | Female | 5 | 46,XX | FLT3, PTPN11, KRAS mutation | <0.01% | 8/10 | PB | 9.13 | 6.01 | 16 | 25 |
| 8 | Male | 6 | 46,XY, inv(16)(p13.1q22) | WT1, CBFB-MYH11 mutation | <0.01% | 6/12 | BM+PB | 9.37 | 7.62 | 14 | 15 |
| 9 | Male | 8 | 46,XY | MLL-AF9 (+), BRAF mutation | 0.03% | 6/12 | PB | 9.97 | 6.45 | 11 | 12 |
| 10 | Male | 9 | 46,XY,t(7;11) (q36;q22), t(8:21)(q22;q22) | MLL-PTD (+), WT1 mutation | <0.01% | 7/12 | PB | 9.73 | 6.92 | 12 | 16 |
| 11 | Female | 5 | 45,X,-X, der(11) t(11;18)(q14;q23), +18 | KRAS, TET-2 mutation | <0.01% | 6/12 | PB | 8.91 | 7.20 | 11 | 14 |
| 12 | Male | 9 | 46,XY, t(1;11)(p32;q23) [13]/47, idem,+9[7] | MLL-AF11 (+), WT1, EV11 mutation | <0.01% | 7/12 | PB | 9.30 | 7.55 | 12 | 15 |
| 13 | Female | 7 | 46,XX,t (8;21)(q22;q22) | RUNX1-RUNX1T1 (+), TET2 mutation | 0.12% | 6/12 | BM+PB | 10.11 | 7.34 | 12 | 15 |
| 14 | Female | 10 | 46,XX | PTPN11, WT1 mutation | <0.01% | 6/12 | PB | 9.59 | 6.16 | 12 | 17 |
| 15 | Male | 12 | 46,XY | WT1, CEBPA, FLT3-ITD mutation | <0.01% | 7/12 | BM+PB | 10.28 | 7.32 | 13 | 13 |
| 16 | Male | 10 | 46,XY | KRAS, WT1 mutation | <0.01% | 6/12 | PB | 9.47 | 6.63 | 11 | 14 |
|
|
|
|---|---|
| Male | 10 (62.5) |
| Female | 6 (37.5) |
| Age (years), median (range) | 8.3 (2–15) |
| Relapsed | 6 (37.5) |
| Refractory | 10 (62.5) |
| Matched | 2 (12.5%) |
| Partially matched | 14 (87.5%) |
| MNC dose (× 108/L), median (range) | 9.67 (8.21–11.53) |
| CD34+ dose (× 106/L), median (range) | 7.12 (5.74–10.32) |
|
|
|
|
|---|---|---|
| Oral cavity | 3 | 0 |
| Heart | 0 | 0 |
| Liver | 2 | 0 |
| Lung | 0 | 0 |
| Kidney | 0 | 0 |
| Gastrointestinal tract | 0 | 0 |
| Bladder | 0 | 0 |
| Central nervous system | 0 | 0 |
|
|
|
|
|
|---|---|---|---|
| I/II | 5 | 31.25 | Skin only |
| III | 3 | 18.75 | Gastrointestinal tract |
| IV | 0 | 0 | – |
| Total aGVHD | 8 | 50 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myeloid Leukemia Research · Hematopoietic Stem Cell Transplantation · Acute Lymphoblastic Leukemia research
Introduction
1
Acute myeloid leukemia (AML), characterized by abnormal hematopoietic stem cell proliferation and differentiation suppression, accounts for approximately 20% of childhood leukemia cases, and recent clinical studies have reported an overall 5-year survival (OS) rate exceeding 70% in pediatric AML (1). In contrast, the prognosis for relapsed/refractory AML (R/R-AML) remains poor, with only 20%−30% event-free survival (EFS) (2). Allogeneic hematopoietic stem cell transplantation (allo-HSCT) emerges as a promising therapeutic avenue, aiming at a curative approach (3). However, post-transplant relapse remains the most important factor affecting patient survival (4). The intensive conditioning regimens have a stronger anti-leukemia effect, which can eliminate more residual leukemia cells, thus reducing the relapse rate after transplantation. Currently, the widely adopted intensive conditioning regimen is the busulfan (Bu) plus cyclophosphamide (Cy)-based approach, with alternative regimens including Cy plus total body irradiation, fludarabine plus Bu, cytarabine-based, and mitoxantrone-based regimens (5).
Cladribine, a synthetic analog of deoxyadenosine utilized for hematological malignancies, can increase the sensitivity of residual abnormal cells to chemotherapy drugs, consume DNA methyltransferase donors to induce apoptosis, and induce a significant lymphocyte-depleting effect. Furthermore, cladribine induces apoptosis in non-dividing cells, contributing to a stronger suppressive effect on malignant clones (6, 7). Its application extends to a rescue therapy for R/R-AML. In search of an effective intensive conditioning regimen for R/R-AML, we attempted to add cladribine to the classic conditioning regimen, aiming to enable AML patients to achieve maximal complete remission (CR) and minimal residual disease (MRD) negativity before allo-HSCT to achieve greater transplantation benefit. Recently, cladribine for allo-HSCT in AML has shown certain prospects and has been mainly used in adult populations. Only a small number of studies have suggested that cladribine plus BuCy may serve as an intensive conditioning regimen for children with R/R AML, and the sample size of these studies is relatively small. This retrospective analysis of 16 children with R/R-AML aims to provide preliminary clinical data on the efficacy and safety of a cladribine-based conditioning regimen, acknowledging the study's limitations.
Materials and methods
2
Study design and patient selection
2.1
In this retrospective study, 16 patients with R/R AML between October 2020 and June 2024 were enrolled. Inclusion criteria comprised: (1) diagnosis of R/R AML following the Guidelines for Diagnosis and Treatment of Acute Myelogenous Leukemia (Relapse/Refractory) in China (2017) (8); (2) age ≤ 18 years; (3) underwent allo-HSCT with a cladribine-based conditioning regimen; and (4) complete clinical and laboratory data, including pre-transplant flow-cytometry MRD results. Exclusion criteria included: (1) concurrent solid tumor or other malignant hematologic disease and (2) incomplete clinical records. Clinical data collected included baseline characteristics, transplantation details, hematopoietic reconstruction, complication prophylaxis, and post-transplant outcomes.
Cladribine-based conditioning regimen
2.2
The cladribine-based conditioning regimen was administered as follows, with dosing scheduled by days −11 to −1 (pre-transplant): cladribine 5 mg/(m^2^·d) on days −11 to −9, cytarabine 2 g/(m^2^·d) on days −11 to −9, Bu 3.2 mg/(kg·d) on days −8 to −6, etoposide 300 mg/(m^2^·d) on days −5, rabbit antithymocyte globulin (ATG) 2.5 mg/(m^2^·d) (HLA-matched donors)/(7.5–8.5) mg/(m^2^·d) (HLA-partially matched donors) on days −5 to −2, and Cy 40 mg/(kg·d) on days −4 to −2. For patients with central nervous system (CNS) leukemia, lomustine (CCNU) 250 mg/(m^2^·d) was added on days −11. The regimen-related toxicity (RRT) was assessed according to Bearman criteria, which included cardiac, pulmonary, hepatic, renal, bladder, oral mucosa, gastrointestinal, and CNS.
Graft versus host disease (GVHD) prophylaxis
2.3
GVHD prophylaxis regimens were stratified by HLA matching status, as detailed in Table 1. GVHD grading and diagnosis were performed in accordance with the 2014 NIH Consensus Development Project criteria for cGVHD and the modified Glucksberg criteria for aGVHD—diagnosis was based on clinical symptoms, physical examination findings, and organ-specific laboratory/imaging evidence, with no strict 100-day post-transplant cutoff for distinguishing aGVHD and cGVHD (9). aGVHD was defined by acute-phase inflammatory manifestations in target organs (skin, gastrointestinal tract, and liver) with no chronic fibrotic changes; cGVHD was defined by chronic fibrotic or sclerotic manifestations in target organs, which may occur de novo or follow aGVHD. The severity of aGVHD and cGVHD was graded according to the above consensus criteria (grade I–IV for aGVHD; limited or extensive for cGVHD).
Infection prophylaxis
2.4
The specific regimens were as follows: pre-transplantation, both donors and recipients are tested for antibodies to cytomegalovirus (CMV), EB virus (EBV), and herpes simplex virus (HSV) pre-transplantation; ganciclovir for preventing viral infections; and oral cephalosporin antibiotics and gentamicin for the elimination of intestinal infection. Post-transplantation, posaconazole for preventing fungal infections and acyclovir for preventing viral infections. After hematopoietic reconstruction, trimethoprim-sulfamethoxazole is used to prevent Pneumocystis jirovecii infection.
Infections were defined as clinical infections requiring intravenous antimicrobial treatment or laboratory-confirmed pathogenic infection (excluding asymptomatic viral reactivation). CMV infection was categorized as CMV DNAemia (positive CMV DNA without clinical symptoms) or CMV disease (DNAemia plus organ-specific symptoms).
Transplantation efficacy
2.5
The first of three consecutive days in which the absolute neutrophil count was >0.5 × 10^9^/L was defined as neutrophil engraftment. The time of platelet reconstitution was defined as the first of seven consecutive days in which platelets were >20 × 10^9^/L without transfusion support, which was defined as platelet engraftment (10). Pre-transplant MRD was detected by multicolor flow cytometry (MFC), with a positivity threshold of ≥0.01%. Bone marrow (BM) morphology, minimal residual disease (MRD), and short tandem repeat polymorphism (STR) were performed on day 30 post-transplantation to detect engraftment and remission status. The above detection was monitored at months 1, 2, 3, 4, 5, 6, 9, and 12 post-transplantation, every 3 months in the second year, and every 6 months thereafter for 5 years. CR was defined as morphologic remission (<5% BM blasts). Relapse was defined as morphologic evidence of leukemia in the bone marrow or any extramedullary site, or MRD positivity (≥0.01%) with clinical progression.
Follow-up
2.6
The endpoint for follow-up was 30 June 2024. Overall survival (OS) was defined as the time from transplantation to death due to any cause or censored at last follow-up. Disease-free survival (DFS) was defined from allo-HSCT to relapse, death from any cause, or last follow-up (censored). Non-relapse mortality (NRM) was defined as death after transplantation due to treatment-related side effects or complications, rather than the recurrence of the primary disease.
Ethical statement
2.7
This study was conducted in accordance with good clinical practice guidelines and the Declaration of Helsinki. The study protocol was approved by the local ethics committee, which waived the requirement for obtaining informed consent due to the retrospective nature of the study.
Statistical analysis
2.8
Quantitative data with normal distribution were expressed as mean ± standard deviation (SD); non-normal data as median (range). Hematopoietic reconstruction time, RRT incidence, and infection profiles were described using descriptive statistics. OS and DFS were estimated by the Kaplan–Meier method with 95% confidence intervals (95% CI). Cumulative incidence of GVHD was calculated using competing risk analysis (competing event: death without GVHD). A two-sided P-value of <0.05 was considered statistically significant. Analyses were performed using IBM SPSS Statistics 26.0 and R (programming language for statistical computing) 4.2.0.
Results
3
Patient characteristics and hematopoietic reconstruction
3.1
The median age of the 16 patients was 8.3 (2–15) years, with 10 males (62.5%) and six females (37.5%). Six (37.5%) patients were diagnosed with relapsed AML, and 10 (62.5%) with refractory AML. All patients achieved CR pre-transplant; flow-cytometry MRD detection showed 13 cases (81.25%) with MRD negativity (<0.01%) and 3 cases (18.75%) with MRD positivity (0.03%−0.12%). Fourteen (87.5%) patients had negative fusion genes; among four patients with RUNX1-RUNX1T1 positivity, two had transcript levels >0.05% pre-transplant (case 6: 0.32%; case 13: 0.76%), and both were MRD positive by MFC.
Twelve (75.0%) patients underwent peripheral blood stem cell (PBSC) transplantation, and 4 (25.0%) received bone marrow stem cells plus PBSC transplantation. HLA was partially matched in 14 (87.5%) patients and matched in the remaining 2 (12.5%) patients. The median mononuclear cell (MNC) and CD34+ cells were 9.67 (8.21–11.53) × 10^8^/kg and 7.12 (5.74–10.32) × 10^6^/kg, respectively.
After allo-HSCT, all patients achieved hematopoietic reconstruction, with a median time of 12 (10–16) days for neutrophil reconstitution and 15 (10–25) days for platelet reconstitution. Morphology and MRD of the bone marrow indicated the CR state at 30 days post-transplantation, as detailed in Tables 2, 3.
RRT and GVHD
3.2
Table 4 provides a detailed RRT occurrence. Five (31.3%) patients experienced grade I/II RRT, including three cases in the oral cavity and two cases in the liver. It mostly occurred within 2 weeks of the conditioning regimen, and could be effectively improved after symptomatic treatment. No grade III/IV RRT and no adverse reactions resulting in death related to the conditioning regimen in the patients were reported.
The cumulative incidence of aGVHD was 50.0% (8/16 patients), with severity grading as shown in Table 5; no grade IV aGVHD was observed. Among the 15 patients evaluable for cGVHD (1 lost to follow-up before cGVHD assessment), the cumulative incidence was 26.7% (4/15 patients); the cGVHD manifestations included three cases of limited local skin cGVHD and one case of ocular keratoconjunctivitis sicca (limited cGVHD). No hepatic vein occlusion disease was reported in any patients.
Infection prophylaxis
3.3
A total of five (31.3%) patients experienced infections, with the virus as the main pathogen. One case of BK virus and one case of BK combined with bacteria were included, all of whom developed grade II hemorrhagic cystitis. During follow-up, three cases of CMV DNAemia (no clinical symptoms, resolved with ganciclovir). No EBV viremia, sepsis, or fatal infections were observed.
Survival
3.4
The median follow-up time was 28.03 (11.67–55.34) months. Up to the last follow-up, 14 patients (87.5%) survived, and two patients (12.5%) died. One death was due to disease relapse (relapse rate: 6.3%, 95% CI: 0.8%−29.1%), and the other was confirmed as bronchiolitis obliterans syndrome (BOS) induced by pulmonary extensive cGVHD (NRM: 6.3%, 95% CI: 0.8%−29.1%); this pulmonary cGVHD case had no prior aGVHD and presented de novo fibrotic changes in the lungs at 6-month post-transplant.
Using the Kaplan–Meier method, the 1-year OS rate was 87.5% (95% CI: 65.2%−96.4%), and the 1-year DFS rate was 87.4% (95% CI: 64.9%−96.3%; Figure 1). The two patients with pre-transplant RUNX1-RUNX1T1 positivity (cases 6 and 13) had negative fusion gene transcripts and MRD negativity 1-month post-transplant, with no relapse at the last follow-up.
Overall survival (OS) and disease-free survival (DFS) rates of R/R AML patients. The 1-year OS rate was 87.5% (95% CI: 65.2%−96.4%), and the 1-year DFS rate was 87.4% (95% CI: 64.9%−96.3%).
Discussion
4
Conditioning regimen of allo-HSCT on R/R AML
4.1
R/R AML is clinically challenging to treat due to its short survival, multiple complications, and difficulty sustaining complete remission. Although novel anti-AML drugs have improved re-induction remission rates in some patients, the long-term efficacy remains unsatisfactory. Allo-HSCT is currently the only curative treatment for R/R AML, especially for patients with primary drug resistance or early recurrence, as it can eradicate leukemia cells via pre-transplant conditioning and post-transplant graft-versus-leukemia (GVL) effect. Myeloablative conditioning (MAC) exerts a stronger GVL effect but is associated with higher GVHD and transplant-related mortality; reduced-intensity conditioning (RIC) reduces transplant-related mortality but fails to lower GVHD and leukemia relapse rates (11). The coexistence of GVHD and GVL is a major clinical challenge, and balancing pre-transplant toxicity and GVL effect is the core of optimizing conditioning regimens. Scott et al. (12) conducted a long-term follow-up of the BMT CTN 0901 trial and found that RIC for AML/MDS had lower transplant-related mortality but inferior DFS compared with MAC, suggesting that MAC should be the first choice for AML/MDS patients with good performance status. This finding supports our use of a cladribine-based intensified MAC regimen for pediatric R/R AML.
Cladribine-based conditioning regimen: direct comparison with published studies
4.2
Hematopoietic reconstruction
4.2.1
Our study showed that all 16 pediatric patients achieved hematopoietic reconstruction, with median neutrophil and platelet engraftment times of 12 and 15 days, respectively. This result is comparable and slightly superior to published adult studies: Xiao et al. (13) reported median neutrophil and platelet engraftment times of 14 and 13 d in 23 adult R/R AML patients with cladribine + BuCy conditioning; Shi et al. (14) reported median neutrophil and platelet engraftment times of 13 d and 28 d in adult AML patients with a cladribine-containing regimen for auto-HSCT. The slightly faster neutrophil engraftment in our pediatric cohort may be related to the immature hematopoietic microenvironment in children, which has a stronger regenerative capacity, and the optimal stem cell infusion dose in our study.
RRT and GVHD
4.2.2
The incidence of I/II grade RRT in our study was 31.3%, with no III/IV grade RRT. This is significantly lower than the 69.6% I/II grade CRRT incidence reported in adult R/R AML patients with cladribine + BuCy conditioning (13). In terms of organ-specific toxicity, our hepatic toxicity incidence (12.5%) was similar to the 27.3% grade I/II liver CRRT in adult studies, and no gastrointestinal RRT was observed (vs. 100% gastrointestinal CRRT in adult studies) (14), which may be due to the optimized dosing schedule of cladribine and cytarabine in our regimen, reducing cumulative gastrointestinal mucosal damage.
For GVHD, the cumulative incidence of aGVHD in our study was 50.0% (grade III: 18.75%, no grade IV), and cGVHD was 26.7%—these rates are consistent with the range of adult studies (aGVHD: 16.7%−50.0%; cGVHD: 13.0%−44.4%) (14, 15). Notably, our study used the 2014 NIH criteria for GVHD diagnosis (excluding the 100-day cutoff), and the only cGVHD-related death was confirmed as BOS, a severe manifestation of pulmonary cGVHD that is rare in pediatric cohorts. This highlights the need for long-term monitoring of pulmonary function in pediatric patients after allo-HSCT. One case of ocular cGVHD in our study was diagnosed as keratoconjunctivitis sicca, the most common ocular manifestation of cGVHD, which is consistent with adult clinical findings (14, 15).
Infections
4.2.3
Post-transplant infection incidence in our study was 31.3%, with viral pathogens as the main cause. This rate is lower than the reported infection incidence in adult cladribine-based conditioning studies (≥50%) (13, 15). No fatal infections or sepsis were observed, which may be attributed to strict pre-transplant donor/recipient viral screening, standardized anti-infective prophylaxis, and milder RRT in our pediatric cohort (reducing the duration of neutropenia). The three cases of asymptomatic CMV DNAemia were all resolved with ganciclovir, indicating that the anti-viral prophylaxis regimen is effective for pediatric patients.
Survival outcomes
4.2.4
Our pediatric cohort achieved a 1-year OS rate of 87.5%, 1-year DFS rate of 87.4%, and NRM of 6.3%. These results are markedly superior to adult R/R AML studies with cladribine-based conditioning: Xiao et al. (13) reported 1-year OS/2-year OS of 74.7%/64.0% and 1-year/2-year EFS of 66.3%/53.1%; Sun et al. (15) reported a 2-year OS of 61.4% and NRM of 9.1%; Tong et al. (16) reported a 1-year OS of 85.6% and 1-year RFS of 73.8%. The superior survival in our study may be due to two factors: (1) cladribine has higher transport efficiency in pediatric cells via human equilibrative and concentrative nucleoside transporters, leading to a stronger anti-leukemia effect (17). (2) All our patients achieved morphologic CR pre-transplant, with 81.25% MRD negative, and the three MRD-positive patients all achieved MRD negativity post-transplant, reducing the relapse risk. In addition, the low NRM (6.3%) in our study is related to mild RRT and low severe infection incidence, further improving survival outcomes.
RUNX1-RUNX1T1 fusion gene positive
4.3
Translocation t (8;21) (q22; q22) (RUNX1-RUNX1T1) accounts for 10%−15% of pediatric AML and is a favorable cytogenetic subtype in de novo AML (18). However, RUNX1-RUNX1T1-positive patients with additional adverse prognostic factors (e.g., c-kit and TET2 mutations) have a poor prognosis, and allo-HSCT can significantly improve their survival (19). Tarantino et al. (20) reported that additional cytogenetic abnormalities and RIC are associated with increased relapse risk in RUNX1-RUNX1T1-positive AML patients undergoing allo-HSCT. In our study, two RUNX1-RUNX1T1-positive patients with additional mutations (c-KIT/TET2) and pre-transplant MRD positivity achieved negative fusion gene transcripts and MRD negativity 1-month post-transplant with the cladribine-based MAC regimen, with no relapse at the last follow-up. This result is better than the reported relapse rate of 20%−30% in high-risk t (8;21) pediatric AML (19), suggesting that the cladribine-based intensified MAC regimen can effectively eliminate residual leukemia cells in high-risk RUNX1-RUNX1T1-positive pediatric R/R AML. However, the small number of such patients in our study (n = 4) means that more clinical data are needed to confirm this conclusion.
Study limitations
4.4
This study has several critical limitations: (1) single-center retrospective design with a small sample size (n = 16), leading to limited statistical power and potential selection bias; (2) lack of a control group (e.g., historical controls treated with standard BuCy), precluding definitive conclusions about efficacy superiority; (3) no multivariate analysis (removed due to inappropriate application with n = 16 and two events); and (4) limited generalizability due to single-arm design and differences in patient populations compared to literature. Future prospective multi-center randomized controlled trials are needed to validate these findings.
Conclusion
5
In this small single-center retrospective study, the cladribine-based conditioning regimen was associated with successful hematopoietic reconstruction, mild RRT, manageable infections, and promising survival outcomes in children with R/R AML, even in partial patients with pre-transplant MRD positivity and high-risk genetic subtypes (e.g., RUNX1-RUNX1T1 with additional mutations). The regimen also effectively induced MRD negativity in post-transplant bone marrow and reduced relapse risk in pediatric patients. However, due to the study's limitations (small sample size, single-center, no control group), claims of improved OS or reduced relapse rates compared with the standard BuCy regimen are unwarranted. The regimen warrants further investigation in larger prospective controlled trials to confirm its efficacy and safety in pediatric R/R AML, and long-term monitoring of pulmonary cGVHD (e.g., BOS) is recommended for pediatric patients after allo-HSCT.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Du M Chen W Liu K Wang L Hu Y Mao Y . The global burden of leukemia and its attributable factors in 204 countries and territories: findings from the global burden of disease 2019 study and projections to 2030. J Oncol. (2022) 2022:1612702. doi: 10.1155/2022/161270235509847 PMC 9061017 · doi ↗ · pubmed ↗
- 2Ruan M Liu LP Zhang AL Quan Qi B Liu F Liu TF . Improved outcome of children with relapsed/refractory acute myeloid leukemia by addition of cladribine to re-induction chemotherapy. Cancer Med. (2021) 10:956–64. doi: 10.1002/cam 4.368133491298 PMC 7897947 · doi ↗ · pubmed ↗
- 3Heuser M Ofran Y Boissel N Brunet Mauri S Craddock C Janssen J . Acute myeloid leukaemia in adult patients: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2020) 31:697–712. doi: 10.1016/j.annonc.2020.02.01832171751 · doi ↗ · pubmed ↗
- 4Lee CJ Savani BN Mohty M Gorin NC Labopin M Ruggeri A . Post-remission strategies for the prevention of relapse following allogeneic hematopoietic cell transplantation for high-risk acute myeloid leukemia: expert review from the acute leukemia working party of the European society for blood and marrow transplantation. Bone Marrow Transplant. (2019) 54:519–30. doi: 10.1038/s 41409-018-0286-230104717 · doi ↗ · pubmed ↗
- 5Zhang XH Chen J Han MZ Huang H Jiang EL Jiang M . The consensus from the Chinese Society of Hematology on indications, conditioning regimens and donor selection for allogeneic hematopoietic stem cell transplantation: 2021 update, J. Hematol Oncol. (2021) 14:145. doi: 10.1186/s 13045-021-01159-234526099 PMC 8441240 · doi ↗ · pubmed ↗
- 6Fissolo N Calvo-Barreiro L Eixarch H Boschert U Espejo C Montalban X . Immunomodulatory effects associated with Cladribine treatment. Cells. (2021) 10:3488. doi: 10.3390/cells 1012348834943995 PMC 8700070 · doi ↗ · pubmed ↗
- 7Mushtaq MU Harrington AM Chaudhary SG Michaelis LC Carlson KB Abedin S . Comparison of salvage chemotherapy regimens and prognostic significance of minimal residual disease in relapsed/refractory acute myeloid leukemia. Leuk Lymphoma. (2021) 62:158–66. doi: 10.1080/10428194.2020.182100932951486 · doi ↗ · pubmed ↗
- 8Leukemia & Lymphoma Group Chinese Chinese Society of Hematology Chinese Medical Association. The guidelines for diagnosis and treatment of acute myelogenous leukemia (relapse/refractory) in China. Zhonghua Xue Ye Xue Za Zhi. (2017) 38:183–4. doi: 10.3760/cma.j.issn.0253-2727.2017.03.00228395439 PMC 7348378 · doi ↗ · pubmed ↗