Intractable Nausea as the Initial Presentation of Neuromyelitis Optica
Shu Jun Tan

TL;DR
A rare neurological condition was misdiagnosed due to persistent nausea and vomiting, highlighting the importance of considering NMOSD in such cases.
Contribution
This case report highlights NMOSD as an under-recognized cause of intractable nausea and vomiting.
Findings
NMOSD can present with persistent vomiting and nausea due to brainstem involvement.
Diagnosis was confirmed through MRI and detection of AQP4 IgG antibodies.
Treatment with steroids and tocilizumab led to significant improvement in symptoms.
Abstract
Neuromyelitis optica spectrum disorder (NMOSD) is an autoimmune condition of the central nervous system, primarily involving the optic nerves and spinal cord. Patients typically present with visual disturbance, limb weakness or sensory deficits, and bladder dysfunction. However, atypical and nonspecific presentations may occur, including persistent nausea and vomiting due to involvement of the area postrema. We report the case of a 26-year-old female patient who presented with a one-month history of intractable vomiting, associated with epigastric discomfort (worse prior to vomiting), reduced appetite, and significant weight loss of approximately 7-8 kg over one month. She had been admitted two times prior to presentation, with extensive investigations that were unremarkable. During admission, she also reported blurred vision and was noted to have horizontal nystagmus. Brain MRI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
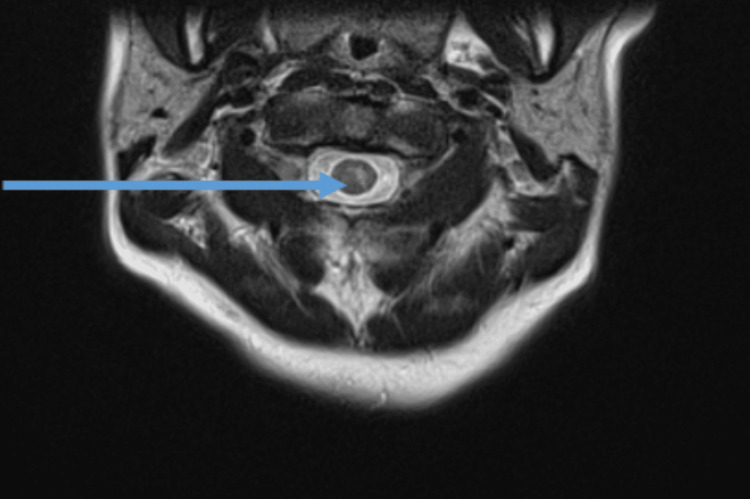 Figure 1
Figure 1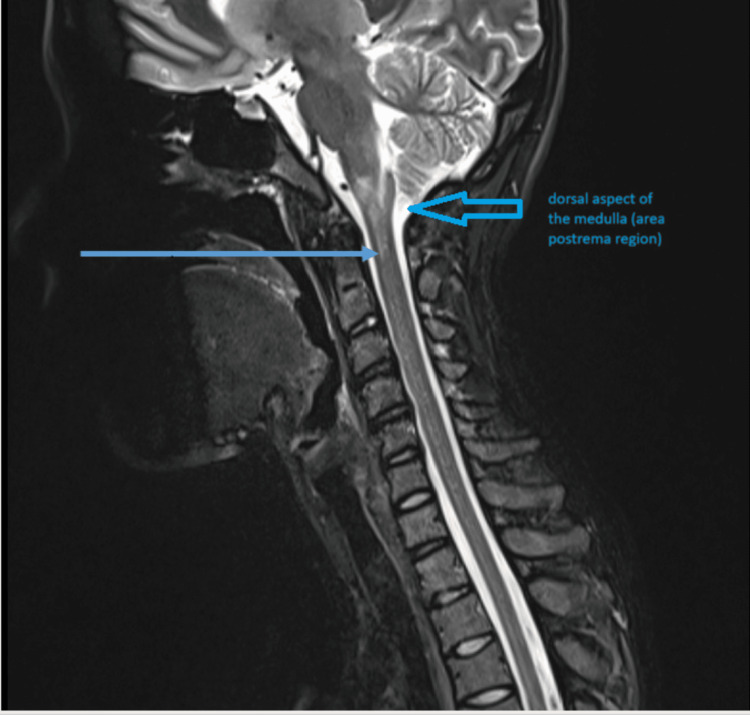 Figure 2
Figure 2| Parameter | Results | Units | References |
| White blood cell | 5.22 | 109/L | 4-11 |
| Neutrophil | 46.0 | % | 40-75 |
| Lymphocytes | 45.0 | % | 20-45 |
| Monocytes | 9.0 | % | 2-10 |
| Eosinophils | 0.0 | % | 0-6 |
| Basophil | 0.0 | % | 0-1 |
| Hemoglobin | 13.4 | g/dL | 11.5-16 |
| Platelets | 239 | 109/L | 140-450 |
| Glucose | 5.1 | mmol/L | 3.3-7 (fasting) |
| Potassium | 3.2 | mmol/L | 3.3-5.1 |
| Sodium | 135 | mmol/L | 135-150 |
| Calcium | 9.7 | mg/dL | 8.4-10.2 |
| Magnesium | 0.91 | mmol/L | 0.65-1.05 |
| Phosphate | 4.1 | mg/dL | 2.7-4.5 |
| Chloride | 96 | mmol/L | 96-109 |
| Bicarbonate | 20 | mmol/L | 21-32 |
| Urea | 30 | mg/dL | 10-50 |
| Creatinine | 0.64 | mg/dL | 0.50-1.60 |
| Bilirubin, total | 0.8 | mg/dL | <1.5 |
| Total protein | 8.6 | g/dL | 6.0-8.3 |
| Albumin | 4.6 | g/dL | 3.4-5.1 |
| Globulin | 4.0 | g/dL | 1.9-3.6 |
| Alb/Glo ratio | 1.1 | 1.2-2.5 | |
| Alkaline phosphatase | 43 | U/L | 39-117 |
| AST/SGOT | 22 | U/L | Up to 35 |
| ALT/SGPT | 19 | U/L | Up to 35 |
| GGT | 26 | U/L | 7-32 |
| C-reactive protein | <0.6 | mg/L | <5.0 |
| Amylase, serum | 98 | U/L | 28-100 |
| Thyroid-stimulating hormone (TSH) | 1.38 | µIU/mL | 0.27-4.20 |
| Free T4 | 1.57 | ng/dL | 0.93 - 1.71 |
| B12 | 483 | pmol/L | 145-569 |
| Folate | 13.50 | nmol/L | 8.83-60.80 |
| Parameter | Results | Units | Reference |
| Erythrocyte sedimentation rate | 7 | mm/hr | 0-20 |
| Antinuclear antibody | 1:320 (nucleolar, speckled) | <1:80 | |
| ANCA | Negative | Negative | |
| MOG IgG | Negative | Negative | |
| AQP4 IgG | Positive | Negative |
| Feature | NMOSD | Multiple sclerosis | MOGAD |
| Typical age of onset | 32-41 years | 20-40 years | Young adults and children |
| Sex predilection | Female | Female | Nil |
| Key antibody | AQP4-IgG-positive | Seronegative | MOG-IgG positive |
| Initial presentation | Optic neuritis, transverse myelitis, and area postrema syndrome | Optic neuritis, sensory deficits, and motor weakness | Optic neuritis, ADEM-like illness |
| Optic neuritis | Often bilateral | Often unilateral | Often bilateral |
| Brain involvement | Areas of high AQP4 expression | Predominantly white matter | Predominantly grey matter |
| Brainstem involvement | Common | Uncommon | Rare |
| Vomiting/hiccups | Common | Rare | Uncommon |
| Spinal cord involvement | Longitudinally extensive transverse myelitis, commonly in the cervical region | Short segment, patchy lesions | Often lower thoracic or conus involvement |
| MRI lesions characteristics | Long, continuous lesions | Multiple discrete lesions | Poorly demarcated lesions |
| Relapse pattern | Relapsing with stepwise disability | Relapsing remitting | Relapsing with better recovery |
| Response to multiple sclerosis treatment | May worsen the disease | Beneficial | Variable |
| Long-term treatment | Immunosuppression | Disease-modifying therapies | Immunosuppression |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Sclerosis Research Studies · Fibromyalgia and Chronic Fatigue Syndrome Research · Peripheral Neuropathies and Disorders
Introduction
Vomiting is a common and nonspecific symptom that is most frequently attributed to gastrointestinal, metabolic, or infectious etiologies [1]. Consequently, neurological causes are often overlooked, particularly in the absence of early focal neurological signs [2]. This may result in repeated hospital admissions, extensive gastrointestinal investigations, and delays in diagnosis. However, persistent or intractable vomiting can represent an atypical manifestation of central nervous system pathology, especially when associated with evolving neurological deficits. The emergence of features such as nystagmus [3], sensory impairment, weakness, or gait instability should prompt urgent neurological evaluation and appropriate neuroimaging. Early recognition of these red flag signs is critical, as timely diagnosis allows for the prompt initiation of disease-modifying therapy, which may significantly improve neurological outcomes and reduce long-term disability [4].
From a neurological perspective, vomiting may arise from relatively benign conditions such as migraine or vestibular disorders, but it may also indicate more serious pathology requiring urgent intervention, including raised intracranial pressure or disorders affecting the lower brainstem. In particular, involvement of the area postrema located in the dorsal medulla can lead to intractable nausea and vomiting [5].
Neuromyelitis optica spectrum disorder (NMOSD) is an autoimmune inflammatory condition of the central nervous system that predominantly affects the optic nerves and spinal cord, with less frequent involvement of the brainstem [6]. Patients classically present with optic neuritis, manifesting as acute visual loss or painful eye movements, and transverse myelitis, which may result in pain, weakness, sensory disturbances, and bowel or bladder dysfunction. Brainstem involvement, especially affecting the area postrema, may cause intractable hiccups, nausea, and vomiting, while hypothalamic involvement has been associated with hypersomnolence or narcolepsy [7].
Our case highlights an uncommon but clinically important presentation of NMOSD, emphasizing the need to consider central nervous system pathology in patients with persistent vomiting and evolving neurological features. Documenting this case aims to raise awareness of area postrema syndrome as a diagnostic clue, reduce delays in diagnosis, and underscore the importance of early immunotherapy in improving neurological outcomes.
Case presentation
A 26-year-old woman presented to our institution in March 2025 with a one-month history of persistent nausea and vomiting, which had begun in February 2025 and was associated with generalized weakness. Her symptoms initially started with one week of nausea, followed by nonbilious, nonbloody vomiting. The vomiting was nonprojectile, involved small volumes of fluid, occurred predominantly at night, and was associated with epigastric discomfort. She denied fever, diarrhea, constipation, or other changes in bowel habits. There was no history of headache, visual disturbance, or focal neurological symptoms at initial presentation. She also reported no recent travel or sick contacts.
Prior to this admission, she had two previous hospitalizations during which she underwent extensive investigations, including abdominal imaging and upper gastrointestinal endoscopy, and was diagnosed with dyspepsia. Over the preceding month, she also reported anorexia and unintentional weight loss of approximately 7-8 kg.
She had no significant past medical history. On physical examination, she was afebrile, and her abdomen was soft and nontender, with no organomegaly or other abnormal findings. Neurological examination was initially normal on presentation.
Laboratory investigations were performed to evaluate for systemic causes (Table 1). There was no evidence of infection. Electrolyte levels were within normal limits, except for mild hypokalemia attributed to ongoing vomiting. Renal, hepatic, and thyroid function tests were normal.
Subsequently, three days into her hospitalization, she reported blurring of vision and an unsteady gait. Neurological examination revealed horizontal nystagmus, impaired proprioception in the right foot, and bilateral lower limb weakness with Medical Research Council (MRC) grade 4-/5 power, more pronounced on the right. Sensory examination demonstrated reduced distal sensation in the digits of both upper limbs. She also had impaired standing balance. Based on these findings, the initial differential diagnoses included Wernicke’s encephalopathy, multiple sclerosis (MS), NMOSD, and myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD). An MRI brain with contrast was performed (Figure 1).
MRI brain: areas of altered signal-T2 hyperintensity with possible restricted diffusion in the brainstem and cervicomedullary junction, along the floor of the fourth ventricleMRI: magnetic resonance imaging
An MRI cervical spine was performed (Figure 2).
MRI spine: T2 hyperintense signal across the cervical medullary junction measuring nearly 2.7 cm in the craniocaudal extent centered along the floor of the fourth ventricle and in the central cordMRI: magnetic resonance imaging
With concerns of transverse myelitis noted on the MRI, an autoimmune screen was performed (Table 2).
The patient was ultimately diagnosed with NMOSD and was promptly treated with pulsed methylprednisolone followed by intravenous tocilizumab, resulting in gradual improvement of her neurological deficits. Following discharge, she has been under regular multidisciplinary follow-up involving neurology, ophthalmology, physiotherapy, and occupational therapy at 2-3 monthly intervals. At follow-up, she remains relapse-free on maintenance tocilizumab, with no new lesions identified on interval MRI.
Discussion
Vomiting is a common and usually benign clinical presentation with a broad differential diagnosis, encompassing infectious, gastrointestinal, metabolic, cardiac, drug-related, and neurological causes [1]. While many etiologies are self-limiting, certain conditions require urgent recognition and intervention, including bowel obstruction, mesenteric ischemia, diabetic ketoacidosis, brainstem stroke, and disorders associated with raised intracranial pressure [8]. Failure to identify these conditions early may result in significant morbidity and mortality.
Demyelinating diseases of the central nervous system represent an important yet frequently under-recognized cause of persistent or intractable vomiting, particularly as neurological manifestations may evolve insidiously and appear later in the disease course. Disorders within this group include MS, NMOSD, MOGAD, and acute disseminated encephalomyelitis (ADEM) [8-9]. As a result, patients may initially undergo repeated gastrointestinal evaluations before a neurological etiology is considered, contributing to diagnostic delay.
NMOSD occurs more commonly in females, with a median age of onset between 32 and 41 years, and predominantly affects the optic nerves and spinal cord, with less frequent involvement of the brainstem [10]. When the brainstem is involved, patients may develop area postrema syndrome. The area postrema, located in the dorsal medulla, plays a critical role in the vomiting reflex and is particularly susceptible in NMOSD due to the absence of a blood-brain barrier and high expression of aquaporin-4 (AQP4) water channels [11]. Consequently, patients, especially those with AQP4-IgG seropositivity, may present with intractable hiccups, nausea, and vomiting, which may precede more classical neurological manifestations such as optic neuritis or transverse myelitis.
Our patient fulfilled the diagnostic criteria for NMOSD based on her clinical presentation with brainstem involvement, characteristic neuroimaging findings, and seropositivity for AQP4 immunoglobulin G (AQP4-IgG). Distinctive imaging features of NMOSD include longitudinally extensive spinal cord lesions and involvement of brain regions with high AQP4 expression. As demonstrated in this case, anatomical involvement of different regions of the central nervous system results in varied clinical manifestations; brainstem involvement led to cranial nerve dysfunction, impaired balance, and persistent nausea and vomiting [12]. The predilection of NMOSD for the area postrema reflects its high AQP4 expression, rendering this region uniquely vulnerable in this disease subtype [13].
NMOSD, MOGAD, and MS share overlapping clinical features, most notably optic neuritis, which is a common presenting manifestation across all three conditions. However, these disorders can be differentiated based on characteristic clinical and radiological features. Optic neuritis in MS typically presents unilaterally, whereas NMOSD and MOGAD more commonly present with bilateral involvement. NMOSD preferentially affects regions of the central nervous system with high AQP4 expression, while MS predominantly involves cerebral white matter, and MOGAD more frequently affects grey matter structures [14].
Spinal cord involvement also differs between these conditions. NMOSD is characteristically associated with longitudinally extensive, continuous cervical spinal cord lesions, while MS typically demonstrates multiple short-segment lesions. In contrast, MOGAD more commonly involves the lower thoracic spinal cord or conus medullaris [14]. These key distinguishing features are summarized in Table 3 [12].
Wernicke’s encephalopathy was another important differential diagnosis, as it classically presents with a triad of ophthalmoplegia, ataxia, and confusion secondary to thiamine deficiency [15]. It is commonly seen in individuals with chronic alcohol use or nutritional deficiency, which was a consideration in this case, given the patient’s one-month history of reduced oral intake and significant weight loss. The pattern of involvement on imaging also differs from NMOSD, which usually affects the medial thalami, mammillary bodies, and periaqueductal gray matter. A trial of intravenous thiamine administered early during admission did not result in clinical improvement, making this diagnosis less likely [16].
Management of NMOSD involves acute treatment with high-dose intravenous corticosteroids, with escalation to plasmapheresis in refractory cases, followed by long-term immunosuppressive therapy to reduce relapse risk and prevent irreversible neurological disability [17]. Early recognition of atypical presentations, such as intractable vomiting due to area postrema involvement, is therefore essential to facilitate timely diagnosis and improve long-term outcomes.
Conclusions
Although vomiting is often benign and self-limiting, persistent, unexplained, or recurrent symptoms should prompt consideration of serious underlying causes. Neurological etiologies, particularly demyelinating disorders involving the brainstem, are an important but frequently under-recognized cause of intractable vomiting. Area postrema syndrome may represent the earliest manifestation of NMOSD and can precede classic features such as optic neuritis or transverse myelitis. Failure to recognize vomiting as a neurological red flag can lead to repeated hospital presentations, unnecessary gastrointestinal investigations, and delays in neuroimaging, specialist referral, and immunotherapy. This case underscores the importance of a broad differential diagnosis, multidisciplinary evaluation, and early recognition to prevent irreversible neurological injury and improve patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1AGA technical review on nausea and vomiting Gastroenterology Quigley EMM Hasler WL Parkman HP 2632861202001 https://www.gastrojournal.org/article/S 0016-5085%2801%2987973-7/fulltext 1120873610.1053/gast.2001.20516 · doi ↗ · pubmed ↗
- 2Adams and Victor’s Principles of Neurology. 11th Edition Ropper AH Samuels MA Klein J Prasad S New York (NY)Mc Graw-Hill Education 2019 https://neurology.mhmedical.com/book.aspx?bookid=1477
- 3Medical and nonstroke neurologic causes of acute, continuous vestibular symptoms Neurol Clin Edlow JA Newman-Toker DE 699716332015 https://pmc.ncbi.nlm.nih.gov/articles/PMC 9116936/2623128110.1016/j.ncl.2015.04.002PMC 9116936 · doi ↗ · pubmed ↗
- 4Autoimmune demyelinating diseases of central nervous system (CNS)Mimics and Red Flags of Multiple Sclerosis Uher T 2597 Cham Springer 2025 https://link.springer.com/chapter/10.1007/978-3-031-98945-2_2
- 5A neurologist’s view of nausea and vomiting Nausea and Vomiting: Mechanisms and Treatment. Advances in Applied Neurological Sciences Parkes JD 160166 Berlin Springer 31986 https://link.springer.com/chapter/10.1007/978-3-642-70479-6_12#citeas
- 6Neuromyelitis optica spectrum disorder (NMOSD): clinical features and diagnosis 1 2026 Glisson CC 2025 https://www.uptodate.com/contents/neuromyelitis-optica-spectrum-disorder-nmosd-clinical-features-and-diagnosis
- 7Neuromyelitis optica: what is it, causes, diagnosis, and more Elsevier 2 2026 Lily Guo MDMD 2026 https://www.osmosis.org/answers/neuromyelitis-optica
- 8Demyelinating disorders of the central nervous system Textbook of Clinical Neurology (Third Edition) Pirko I Noseworthy JH 11031133 Philadelphia (PA)WB Saunders 2007 https://pmc.ncbi.nlm.nih.gov/articles/PMC 7158368/