Refractory Neoscytalidium dimidiatum subcutaneous infection with dual CARD9/GATA2 variants: Synergistic clearance by voriconazole and targeted hyperthermia
Ying Huang, Xin Ran, Runyan Gao, Zhi Zhang, Jitong Sun, Sifen Lu, Yaling Dai, Yuping Ran

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1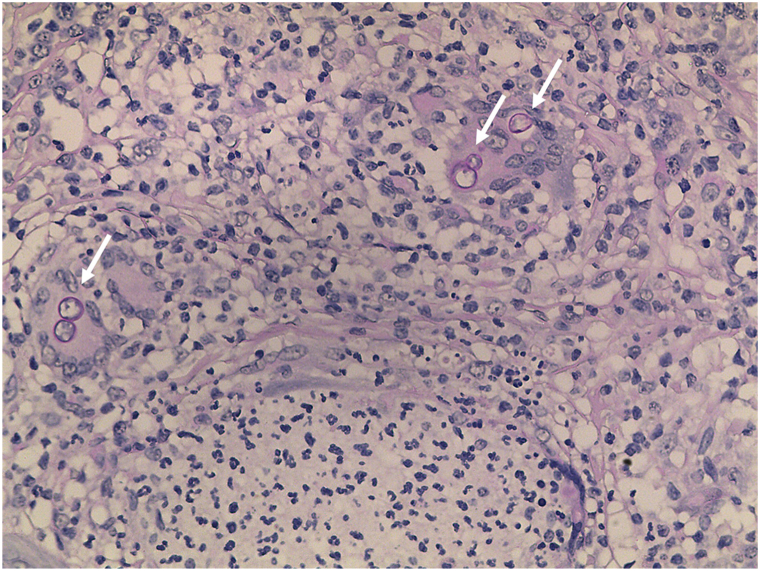 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Actinomycetales infections and treatment
To the Editor: We present a 51-year-old immunocompetent male carpenter with a 3-year history of multiple papules, nodules, and verrucous erythematous plaques on his neck, following accidental traumatic implantation of contaminated wood chips. The patient had hypertension but was otherwise healthy, with no tumors detected on screening. The lesion began as a small papule and slowly progressed. A previous diagnosis of fungal infection was made by biopsy at a local hospital, and the patient initially received oral itraconazole (200 mg/d) for 2 weeks with limited improvement.
Physical examination revealed multiple papules, nodules, and a well-demarcated erythematous plaque, measuring 8 × 4 cm on his neck. In vivo dermoscopy showed blackish-red dots on an erythematous base with yellowish scales (Supplementary Fig 1, available via Mendeley at https://data.mendeley.com/datasets/cgkjsg364m/1). Fungal culture and tissue metagenomic next-generation sequencing confirmed the diagnosis of cutaneous phaeohyphomycosis caused by Neoscytalidium dimidiatum (N dimidiatum). The patient was treated with itraconazole (400 mg/d) for 3 months, achieving satisfactory remission. Subsequently, he discontinued the treatment. He did not return to our hospital until the skin eruptions had relapsed and worsened (Fig 1) for 5 months. During the relapse, the patient resumed itraconazole therapy but showed no improvement.Fig 1. Phaeohyphomycosis presenting with multiple papules, nodules, and verrucous erythematous plaques on the neck when relapsed and worsened.
Given the chronic course and poor response, we performed whole-genome sequencing, which revealed a likely pathogenic heterozygous CARD9 variant c.1249C>T (p.Gln417∗) and a heterozygous GATA2 variant c.14C>T (p.Pro5Leu) of uncertain significance. We performed skin biopsy, tissue culture, and metagenomic next-generation sequencing again. Colonies initially appeared white, rapidly turning gray with a black reverse (Supplementary Fig 2, available via Mendeley at https://data.mendeley.com/datasets/cgkjsg364m/1). Slide culture (Supplementary Figs 3 and 4, available via Mendeley at https://data.mendeley.com/datasets/cgkjsg364m/1) and scanning electron microscopy (SEM) (Supplementary Fig 5, available via Mendeley at https://data.mendeley.com/datasets/cgkjsg364m/1) showed septate hyphae and ellipsoidal or oval-shaped, unicellular or bicellular arthroconidia in chains, which are the morphological characteristics of Neoscytalidium spp. Following dermoscopy-guided sampling of the blackish-red dots, we observed arthrospores via SEM at low and high continuous magnifications (Supplementary Fig 6, available via Mendeley at https://data.mendeley.com/datasets/cgkjsg364m/1). DNA extraction from cultured colonies identified the fungus as N dimidiatum (GenBank PQ272930). Dermoscopy-directed biopsy of the blackish-red dots showed diffuse mixed inflammatory cell infiltration in the dermis, accompanied by multinucleated giant cells (Supplementary Fig 7, available via Mendeley at https://data.mendeley.com/datasets/cgkjsg364m/1), and periodic acid-Schiff (Fig 2) and Gomori’s methenamine silver staining was positive (Supplementary Fig 8, available via Mendeley at https://data.mendeley.com/datasets/cgkjsg364m/1).Fig 2. Fungal structures (white arrow) inside multinucleated giant cells by PAS staining (×400), biopsy consistent with phaeohyphomycosis. PAS, Periodic acid-Schiff.
Antifungal susceptibility testing indicated the isolate was sensitive to voriconazole (minimum inhibitory concentration: 0.06 μg/mL) and topical luliconazole. Additionally, temperature experiment showed the isolate did not grow at 42 °C. Based on these results, treatment was switched to oral voriconazole (400 mg/d), topical luliconazole cream, and hyperthermia using an electric heating pad (>42 °C, 60 minutes, once daily). After 7 months of treatment, the lesion was almost cured (Fig 3), with dermoscopic blackish-red dots fading (Supplementary Fig 9, available via Mendeley at https://data.mendeley.com/datasets/cgkjsg364m/1). No recurrence has been observed to date.Fig 3N dimidiatum subcutaneous infection. Significant improvement after antifungal treatment. N dimidiatum, Neoscytalidium dimidiatum.
Subcutaneous infections caused by N dimidiatum are infrequently documented.1 We present a case illustrating diagnostic and therapeutic challenges in managing such infections. Susceptibility gene screening identified 2 variants, in CARD9 and GATA2, both reported to be associated with increased fungal susceptibility, providing insight into susceptibility mechanisms and guiding individualized therapy for refractory fungal infections.2, 3, 4 In previous cases, blackish-red dots have been associated with subcutaneous fungal infections.5 In this case, the dermoscopic “blackish-red dot sign” observed in situ by SEM suggests that it may serve as a marker for early identification in chronic subcutaneous fungal infections.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Garinet S.Tourret J.Barete S.Invasive cutaneous Neoscytalidium infections in renal transplant recipients: a series of five cases BMC Infect Dis 15201553510.1186/s 12879-015-1241-026586129 PMC 4653896 · doi ↗ · pubmed ↗
- 2Zhou L.Zhuang K.Qi X.Cutaneous mucormycosis and fusariosis in a Chinese woman with CARD 9 deficiency Mycopathologia 188620231093109510.1007/s 11046-023-00796-037864673 · doi ↗ · pubmed ↗
- 3Roy C.Belga S.Lavergne V.Nevill T.J.Majocchi's granuloma in a patient with GATA 2 haploinsufficiency undergoing hematopoietic stem cell transplantation Transpl Infect Dis 2412022 e 1376410.1111/tid.1376434793614 · doi ↗ · pubmed ↗
- 4Zhuansun Y.He P.Du Y.Lin L.Chen R.Li J.High frequency of GATA 2 variants in patients with pulmonary fungal disease without immunocompromised risk factors: a retrospective study J Thorac Dis 16820245180518910.21037/jtd-24-58339268106 PMC 11388249 · doi ↗ · pubmed ↗
- 5Huang Y.Ran X.Gao R.Sun J.Lu S.Ran Y.Chromoblastomycosis caused by Fonsecaea monophora: using SEM and TEM to decipher the “blackish-red dot sign” observed in dermoscopy J Dermatol 5322026 e 109e 11110.1111/1346-8138.7007241277811 · doi ↗ · pubmed ↗