Temporal trends and factors associated with live preterm births in Espírito Santo, 2012-2021
Marcone Marques da Rocha, Laércio da Silva Paiva, Lara Bourguignon Lopes, Raiza Brito Cipriano, Lucca Tamara Alves Carretta, Fernando Rocha Oliveira, Marcone Marques da Rocha, Laércio da Silva Paiva, Lara Bourguignon Lopes, Raiza Brito Cipriano, Lucca Tamara Alves Carretta

TL;DR
This study examines preterm birth trends and associated factors in Brazil's Espírito Santo state from 2012 to 2022, finding regional variations and key risk factors.
Contribution
The novel contribution is identifying regional disparities and socioeconomic factors linked to preterm births in Espírito Santo.
Findings
Prematurity rates were higher among male infants with low weight and low Apgar scores.
Maternal factors like lack of education and no prenatal care were strongly associated with preterm births.
Some regions showed increasing preterm birth rates, while others decreased, highlighting regional health inequalities.
Abstract
To analyze the temporal trend of live premature births in the State of Espírito Santo (Brazil) between 2012 and 2022 and to identify associated factors. Ecological study using secondary data from the Live Birth Information System (SINASC), covering premature births in Espírito Santo between 2012 and 2022. Prais-Winsten regression was used to assess the temporal trend of the prematurity rate, and the Prevalence Ratio (PR) was used to identify factors associated with premature birth. A higher prevalence of premature birth was observed among boys (PR=1.06) with weight <2,500 g, Apgar score at one and five minutes <7 (PR=3.10 and PR=4.05), and with the presence of congenital anomalies (PR=2.74). Among maternal factors, higher prevalences were found among mothers with no schooling (PR=1.51), without a partner (PR=1.11), aged <19 years or >35 years (PR 1.14; PR 1.32), who did not have…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
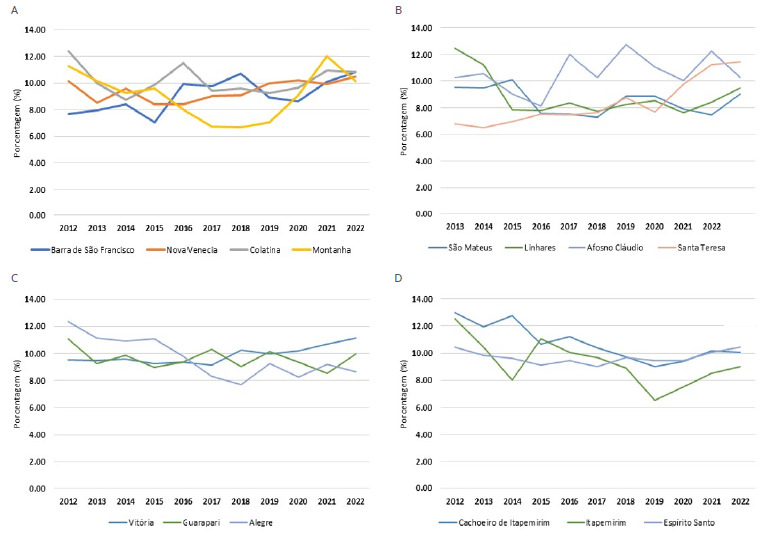 Figure 1
Figure 1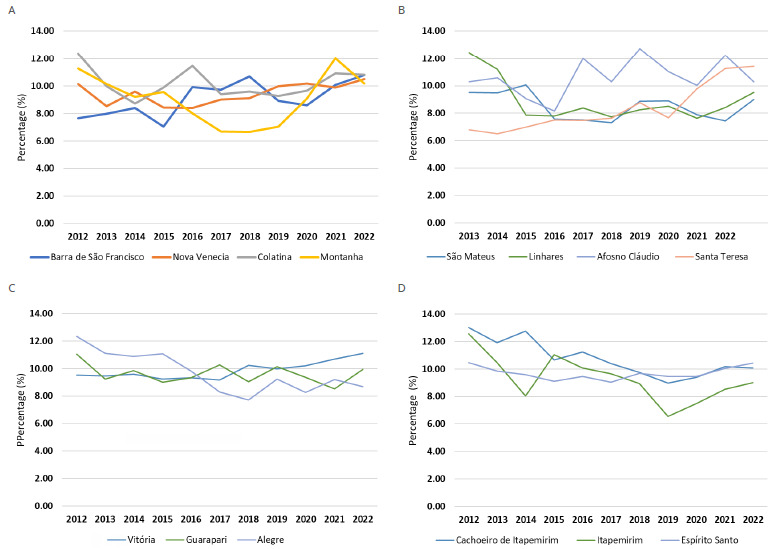 Figure 2
Figure 2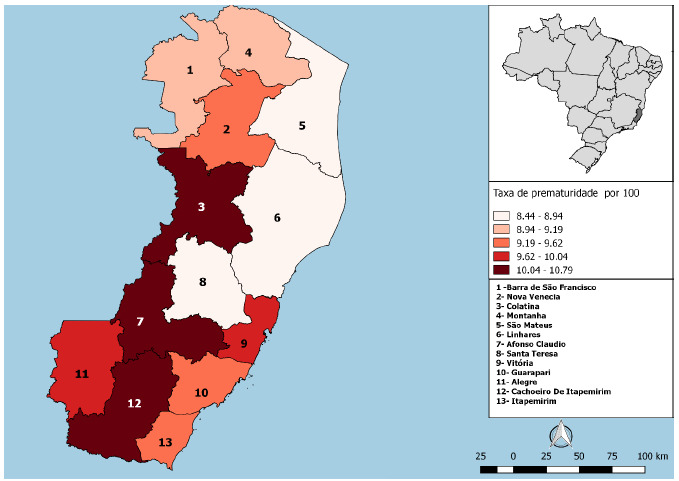 Figure 3
Figure 3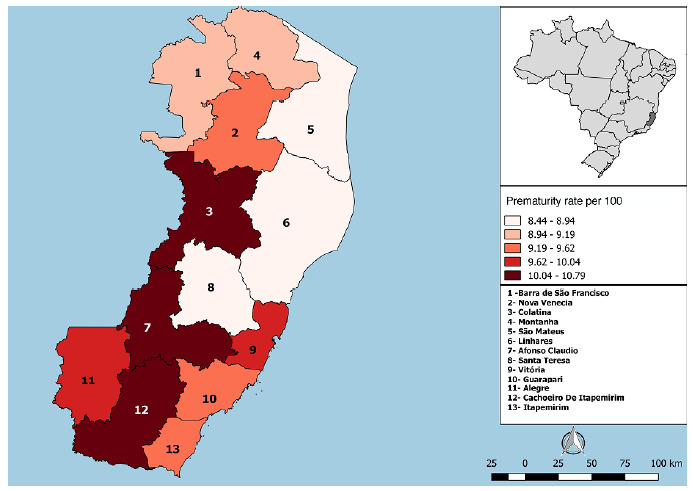 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and Neonatal Healthcare · Preterm Birth and Chorioamnionitis · Infant Development and Preterm Care
INTRODUCTION
Prematurity and its associated complications constitute a global problem that significantly affects maternal and child health and represent an important indicator of the quality of obstetric and neonatal care. Preterm births, defined as those occurring before 37 weeks of gestation, are associated with high rates of neonatal morbidity and mortality, as well as long-term developmental impairments1 ^,^ 2.
In Brazil, the analysis of temporal trends in prematurity and its associated factors in specific local contexts, such as the state of Espírito Santo (ES), is essential for addressing health inequalities and improving maternal and infant outcomes. Socioeconomic, demographic, and health service access factors may influence prematurity rates, and the identification of these factors can inform public health actions and intervention strategies3 ^,^ 4.
In this context, the present study aims to analyze, with depth and methodological rigor, the temporal trends of live preterm births in Espírito Santo between 2012 and 2022, as well as the associated factors that shape this complex phenomenon. Through a comprehensive and integrated analysis, this study seeks to contribute to the understanding and management of prematurity at birth, with implications for public health and population well-being.
METHODS
This ecological study analyzed secondary data on preterm live births (<37 weeks of gestation)5 in the state of ES, Brazil, from 2012 to 2022. The data were obtained from the Information System on Live Births (Sistema de Informações sobre Nascidos Vivos - SINASC) and included maternal and neonatal characteristics. The state of ES was selected as the study setting due to its population diversity, with an estimated population of 3,833,712 inhabitants according to the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística - IBGE)6.
SINASC is a national database of the Ministry of Health that is populated through the Live Birth Declaration (Declaração de Nascido Vivo - DNV), a mandatory document in Brazil. The system provides standardized information on the mother, pregnancy and delivery, and the newborn. It is a publicly accessible database and is widely used in epidemiological studies because it enables the monitoring of maternal and child health indicators7.
Live births are defined as the complete expulsion or extraction of the product of conception from the mother’s body, regardless of gestational age, that, after separation, breathes or shows signs of life, such as a heartbeat, umbilical cord pulsation, or voluntary muscle contraction8. The number of preterm live births refers to infants with a gestational age of less than 37 weeks who, after complete expulsion or extraction from the mother’s body, exhibit at least one sign of life5 ^,^ 8. The prematurity rate was calculated as the proportion of preterm births in relation to the total number of live births during the analyzed period9.
The information collected on live births included gender, race/color, birth weight, presence of congenital anomalies, and Apgar scores at 1 and 5 minutes. Maternal sociodemographic variables included education level, marital status, and age. Pregnancy-related information comprised the number of prenatal visits and whether this number was considered adequate (≥6 visits), according to the definition of the Ministry of Health10. The type of pregnancy and the type of delivery were also examined.
For statistical analysis, Prais-Winsten regression was used to assess temporal trends in the prematurity rate between 2012 and 2022, stratified by IBGE microregions. The slope coefficient (β), probability value (p), predictive capacity (r^2^), annual percentage change (APC), and mean APC were calculated. Prevalence ratio (PR) analyses were conducted to identify factors associated with preterm birth.
The data analyzed were public and secondary, obtained from the Information System on Live Births of the Department of Informatics of the Unified Health System (Departamento de Informática do Sistema Único de Saúde - DATASUS). Therefore, approval by a research ethics committee was not required, in accordance with Resolutions No. 466/2012 and No. 510/2016 of the National Health Council.
Data availability statement:
The entire dataset supporting the results of this study is available upon request to the corresponding author.
RESULTS
Among preterm live births, a slight predominance of males over females was observed, and most were classified as Brown, followed by White and Black. The occurrence of congenital anomalies was 2%, and the most prevalent birth weight was ≥2,500 g. Regarding neonatal vitality, 26.7% presented an Apgar score <7 at the first minute of life; however, most recovered by the fifth minute, and 7.6% remained with unsatisfactory scores (Table 1).
Table 1.Sociodemographic characteristics of mothers and live births, 2012-2022.CharacteristicsPretermTermn (%)GenderFemale27,421 (47)261,129 (48.9)Male30,919 (53)273,193 (51.1)Race/colorWhite15,092 (26.5)137,324 (25.46)Black3,856 (6.8)32,430 (6.01)Yellow200 (0.4)1,551 (0.29)Brown37,468 (65.8)352,775 (65.36)Indigenous189 (0.3)1,410 (0.26)Birth weight (g)≥2,50028,679 (49.2)516,109 (96.5)1,500-2,49922,435 (38.4)17,609 (3.3)500-1,4994,203 (7.2)283 (0.1)<5003,060 (5.2)350 (0.1)Congenital anomalyNo56,764 (98.0)527,968 (99.4)Yes1,147 (2.0)3,163 (0.6)Apgar score at 1 minute≥742,234 (73.28)483,001 (91.25)<715,400 (26.72)46,342 (8.75)Apgar score at 5 minutes≥753,250 (92.38)522,138 (98.62)<74,392 (7.62)7,315 (1.38)Education (years)None169 (0.3)936 (0.2)1 to 3 1,115 (1.9)8,011 (1.5)4 to 7 10,371 (18.0)90,979 (17.2)8 to 11 33,658 (58.6)321,445 (60.6)12 or more12,209 (21.2)108,714 (20.5)Marital statusWith partner31,830 (55.0)307,447 (58.0)Without partner25,991 (45.0)222,073 (42.0)Maternal age (years)<19 9,286 (15.9)78,945 (14.8)20 to 34 37,993 (65.1)375,498 (70.3)>35 years11,100 (19.0)79,911 (14.9)Number of prenatal visitsNone1,203 (2.1)5,895 (1.1)1 to 3 6,720 (11.6)27,340 (5.1)4 to 6 20,862 (36.0)117,837 (22.1)7 or more29,079 (50.3)381,142 (72)Prenatal care adequacyAdequate24,784 (60.6)291,055 (75.4)Inadequate15,519 (37.9)92,180 (23.9)No prenatal care611 (1.5)2,733 (0.7)Type of pregnancySingleton51,221 (87.8)528,258 (98.9)Twin7,131 (12.2)5,854 (1.1)Type of deliveryVaginal20,940 (35.9)199,652 (37.4)Cesarean section37,397 (64.1)334,398 (62.6)
Maternal age among preterm births was predominantly between 20 and 34 years; however, substantial proportions of adolescents (15.9%) and women aged 35 years or older (19.0%) were also observed, groups recognized as having higher obstetric risk. Most mothers had 8 to 11 years of schooling, and the majority had a partner. Regarding prenatal care, only half of the pregnant women attended seven or more consultations, whereas 37.9% had an inadequate number of visits and 1.5% received no prenatal care. Most pregnancies were singleton and resulted in cesarean delivery (Table 1).
Preterm infants were more frequently male than those born at term, more often classified as brown race/color, and presented lower Apgar scores at one and five minutes. Regarding maternal characteristics, higher proportions of mothers aged <19 and >35 years were observed among preterm births compared with term births; similar patterns were found for absence of a partner and lower maternal educational attainment. The frequency of fewer than seven prenatal visits and the absence of prenatal care were also higher among preterm births. Although most pregnancies were singleton in both groups, twin pregnancies were more frequent among preterm births, as was the predominance of cesarean delivery (Table 1).
The results presented in Table 2 highlight factors associated with prematurity. Male gender showed a significant association with prematurity (PR=1.06), indicating a 6% higher probability of preterm birth compared with female gender. Black, Asian, and Indigenous race/color categories presented a higher prevalence of prematurity compared with the White category, whereas Brown race/color showed a lower prevalence. Infants with birth weight <2,500 g exhibited significantly higher PRs. In addition, the presence of congenital anomalies and Apgar scores <7 at one and five minutes were strongly associated with prematurity (Table 2).
Table 2.Multivariable analysis of factors associated with prematurity among live births, 2012-2022.CharacteristicsPreterm live births2012-2022PR (95%CI)p-valueGender Female1 Male1.06 (1.05-1.08)<0.001Race/color White1 Black1.07 (1.03-1.10)<0.001Yellow1.15 (1.01-1.31)0.03Brown0.96 (0.95-0.98)<0.001Indigenous1.19 (1.04-1.36)0.01Birth weight (g) ≥2,5001 1,500-2,49910.64 (10.49-10.79)<0.001500-1,49917.79 (17.55-18.04)<0.001<50017.04 (16.77-17.32)<0.001Congenital anomaly No1 Yes2.74 (2.60-2.88)<0.001Apgar score at 1 minute ≥71 <73.10 (3.05-3.15)<0.001Apgar score at 5 minutes ≥71 <74.05 (3.95-4.15)<0.001Maternal education (years) 12 or more1 None1.51 (1.31-1.74)<0.0011 to 3 1.21 (1.14-1.28)<0.0014 to 7 1.01 (0.98-1.03)0.2898 to 11 0.92 (0.92-0.95)<0.001Marital status With partner1 Without partner1.11 (1.09-1.13)<0.001Maternal age (years) 20 to 34 1 <19 1.14 (1.12-1.17)<0.001>35 1.32 (1.30-1.35)<0.001Number of prenatal visits 7 or more1 None2.39 (2.26-2.52)<0.0011 to 3 2.78 (2.71-2.82)<0.0014 to 6 2.12 (2.08-2.15)<0.001Prenatal care adequacy Adequate1 No prenatal care2.32 (2.16-2.50)<0.001Inadequate1.83 (1.80-1.87)<0.001Type of pregnancy Singleton1 Twin6.21 (6.10-6.32)<0.001Type of delivery Vaginal1 Cesarean section1.05 (1.04-1.07)<0.001
Mothers with no formal schooling showed a higher prevalence of preterm births compared with those with 12 or more years of education; a similar pattern was observed among mothers without a partner compared with those with a partner. Maternal age <19 years or >35 years was associated with a higher prevalence ratio for prematurity, as were twin pregnancies. Regarding prenatal care, the absence of visits and a low number of prenatal visits were also associated with a higher prevalence of prematurity (Table 2).
Table 3 presents the historical trends in prematurity across the microregions of ES, while Figure 1 illustrates temporal variations over the study period, and Figure 2 provides a spatial perspective, allowing visualization of the geographic distribution of prematurity within the state. Between 2012 and 2022, the overall prematurity rate in ES remained stationary, although regional variations were observed.
Table 3.Trend analysis of the prematurity rate by Brazilian Institute of Geography and Statistics microregion, 2012-2022.Total period (2012-2022)APC (95%CI)r²p-valueTrendBarra de São Francisco2.33 (0.69-4.71)0.5170.015IncreasingNova Venecia0.93 (-0.69-2.33)0.6100.235StationaryColatina0.003 (-2.28-2.33)0.5590.666StationaryMontanha-0.69 (-6.67-4.71)0.5610.764StationarySão Mateus-1.14 (-2.28-1.62)0.4600.329StationaryLinhares-2.28 (-6.67-2.33)0.710.261 StationaryAfonso Claúdio1.39 (-0.69-2.33)0.4740.150 StationarySanta Teresa4.71 (2.33-7.15)0.6950.001 IncreasingVitoria1.39 (0.23-2.33)0.8650.013 IncreasingGuarapari-0.46 (-1.83-0.46)-0.238 StationaryAlegre-2.28 (-4.5 to -0.69)0.8270.012Decreasing Cachoeiro de Itapemirim-2.73 (-4.5 to -0.92)0.8090.005 Decreasing Itapemirim-3.39 (-6.67-0.18)0.5520.044 Decreasing Espírito santo 0.05 (-1.6-1.62)0.9150.953Stationary
Figure 1.Trend in prematurity rates across microregions of Espírito Santo according to the Brazilian Institute of Geography and Statistics (2012-2022).
Figure 2.Spatial distribution of prematurity rates in Espírito Santo from 2012 to 2022.
Some microregions, such as Barra de São Francisco, Santa Teresa, and Vitória, exhibited increasing trends in the proportion of preterm births, indicating a consistent rise throughout the historical series. In contrast, microregions such as Alegre, Cachoeiro de Itapemirim, and Itapemirim demonstrated decreasing trends. The remaining microregions showed stationary behavior, with no significant variations over the period, revealing a heterogeneous pattern within the state (Table 3; Figures 1 and 2).
DISCUSSION
The findings of this study indicate that prematurity is strongly associated with a set of biological and social factors, reinforcing its multifactorial nature11 ^,^ 12. Associations with maternal characteristics further support this perspective: the higher prevalence among mothers with lower levels of education reflects barriers to access to information and health services, while the absence of a partner suggests greater social vulnerability and reduced support during pregnancy. In addition, the higher frequency of prematurity at the extremes of maternal age reflects the influence of structural inequalities on maternal and child health and underscores the relevance of public policies targeting populations at increased risk13 ^,^ 14 ^,^ 15.
The gender distribution among preterm infants showed a predominance of males, corroborating findings reported in previous studies11 ^,^ 16. Slower development of the lungs and immune system in males, as well as the protective effect of higher estrogen levels in females, has been described as a possible explanation for this pattern17 ^,^ 18. An unequal distribution of prematurity was also observed across race/color categories, with higher prevalences among non-White groups. This pattern may be related to socioeconomic conditions, access to health services, and the quality of prenatal care19 ^,^ 20. Additionally, structural racism has been identified as a factor that limits access to resources and opportunities, thereby exacerbating health disparities21.
Preterm infants showed a significantly higher prevalence of birth weight below 2,500 g. Considering that newborns typically reach this weight at approximately 37 weeks of gestation, when they are classified as full term, this finding is expected in the context of prematurity. For a more accurate assessment of fetal growth restriction, the use of indicators such as weight-for-gestational-age Z-scores is required, as these measures can distinguish whether low birth weight results exclusively from prematurity or from intrauterine growth restriction22 ^,^ 23.
An additional relevant finding was the association between prematurity and congenital anomalies. Although most infants did not present congenital anomalies, their prevalence was higher among preterm infants, consistent with reports in the literature24 ^,^ 25. This relationship may be associated with genetic, teratogenic, and environmental factors that affect fetal development. In certain situations, the presence of an anomaly may precipitate delivery due to clinical complications that trigger spontaneous labor or require early termination of pregnancy because of maternal-fetal risk24 ^,^ 25 ^,^ 26.
Apgar scores in the first minutes after birth are an important indicator of neonatal health status. Preterm infants presented a higher proportion of Apgar scores lower than 7 at one and five minutes compared with term infants, underscoring their greater physiological vulnerability. These differences indicate that preterm infants require more intensive immediate support and specialized neonatal care, which is associated with longer hospital stays, increased healthcare costs, and a higher risk of neonatal morbidity and mortality12 ^,^ 27.
The higher frequency of cesarean deliveries and twin pregnancies among preterm births reflects the greater clinical complexity of these pregnancies and the need for intensified obstetric monitoring28. The significantly higher prevalence of cesarean sections can be explained by their indication in the presence of complications such as acute fetal distress and intrauterine growth restriction, conditions that often culminate in preterm delivery29. In twin pregnancies, increased maternal physiological burden contributes to complications such as preterm labor. Additionally, twin gestations are more frequently associated with obstetric indications for early termination of pregnancy30.
The Rio de Janeiro State Federation of Industries (Federação das Indústrias do Estado do Rio de Janeiro - FIRJAN) Municipal Development Index (Índice FIRJAN de Desenvolvimento Municipal - IFDM) assesses the level of socioeconomic development of Brazilian municipalities. In the health dimension, the IFDM incorporates indicators related to prenatal care coverage, infant mortality from preventable causes, and hospitalizations sensitive to primary care. ES was classified as having a moderate level of health development; however, only 1.3% of its municipalities reached a high level, while nearly 40% remained at a low level31.
These disparities reflect substantial heterogeneity among municipalities and the specific characteristics of local health care networks, which influence the regional variability in prematurity rates observed in this study32 ^,^ 33. The microregions of Barra de São Francisco and Santa Teresa, characterized by a predominantly rural profile and municipalities concentrated in areas of moderate or low development, exhibited increasing trends in prematurity. This pattern may be related to barriers in access to adequate prenatal care and delays in the timely referral of high-risk pregnant women34.
In Vitória, despite a high IFDM classification, the observed increase in prematurity rates may be related to the concentration of high-complexity maternity hospitals that receive high-risk pregnant women from across the state35. Conversely, microregions in southern Espírito Santo exhibited decreasing trends, which may be associated with the presence of well-structured regional hospitals and greater integration between primary care and referral services. This pattern is consistent with improvements in the health dimension of the IFDM in these municipalities; in Cachoeiro de Itapemirim, for instance, the index increased from 0.56 in 2013 to 0.70 in 202334.
Given the persistent challenges in reducing prematurity rates in Brazil, examining the quality of access to health services is particularly relevant, especially when gestational risk stratification is considered a central strategy for preventing adverse outcomes. Adequate identification of high-risk pregnant women, even within primary care, enables timely referral to specialized outpatient services, ensuring multidisciplinary follow-up and targeted interventions. Failures in these processes, whether due to underreporting of risk or barriers to accessing referral services, increase maternal vulnerability and contribute to the persistence of high rates of preterm live births12 ^,^ 36.
In this context, health education plays a central role by expanding the knowledge of pregnant women and their families regarding warning signs and the importance of adherence to prenatal care. When combined with continuous professional training and improvements in microprocesses within health services, it promotes comprehensive and continuous care. Therefore, investment in actions that strengthen individual care, while also prioritizing health network structuring and equity in access, may represent a promising approach to addressing persistently high rates of preterm births12 ^,^ 33 ^,^ 36.
The results of this study indicate that the rate of preterm live births in ES between 2012 and 2022 remained stable, despite significant regional variations that reflect distinct local contexts of vulnerability. A higher prevalence of prematurity was observed among male newborns; those classified as Black, Asian, or Indigenous race/ethnicity; infants with unsatisfactory Apgar scores; and those with congenital anomalies. Higher prevalences were also associated with lower maternal educational attainment, absence of a partner, extremes of maternal age, a reduced number of prenatal visits, and increased frequencies of twin pregnancies and cesarean deliveries.
These findings reinforce the multifactorial nature of prematurity and underscore the need for strategies that expand access to and improve the quality of prenatal care, while ensuring equity in maternal and child health. Investment in public health actions and educational programs for pregnant women plays an important role, and public policies should prioritize support for pregnant women in vulnerable situations and promote collaboration between the health and education sectors to address preventive actions in a comprehensive and coordinated manner.
This study has some limitations. The ecological study design does not allow for the inference of individual-level causality. The use of secondary data from SINASC may be subject to underreporting and incomplete data entry and does not allow for more robust analyses of associated factors, such as hierarchical modeling, in addition to the absence of relevant variables, including the quality of prenatal care. Furthermore, regional differences in data collection and recording practices may have influenced the results. Finally, contextual factors, such as local policies and broader social determinants, were not directly captured.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fernandes MM Nascimento JA Vianna RP Silva DG Cruz DF Fatores que influenciam a mortalidade infantil Arq Ciênc Saúde Unipar 20232762353236410.25110/arqsaude.v 27i 6.2023-015 · doi ↗
- 2Barros PS AquinoÉC Souza MR Mortalidade fetal e os desafios para a atenção à saúde da mulher no Brasil Rev Saúde Pública 201953121210.11606/S 1518-8787.201905300071430726493 PMC 6390672 · doi ↗ · pubmed ↗
- 3Vanderlei LC Frias PG Avanços e desafios na saúde materna e infantil no Brasil Rev Bras Saude Matern Infant 201515215716010.1590/S 1519-38292015000200001 · doi ↗
- 4Gonzaga IC Barreto IC Cardoso AR Souza MF Almeida JAG Atenção pré-natal e fatores de risco associados à prematuridade e baixo peso ao nascer em capital do nordeste brasileiro Ciên Saúde Coletiva 20162161965197410.1590/1413-81232015216.0616201527276545 · doi ↗ · pubmed ↗
- 5Instituto Brasileiro de Geografia e Estatística (IBGE) Estimativas da população residente para os municípios e para as unidades da federação brasileiros com data de referência em 1º de julho de 2022[Internet]Rio de Janeiro IBGE 2022 Jun 4, 2023 Available at: https://www.ibge.gov.br/estatisticas/sociais/populacao/9103-estimativas-de-populacao.html
- 6World Health Organization Born too soon: decade of action on preterm birth[Internet]Genebra World Health Organization 2023 Sep 3, 202598 p Available at: https://www.who.int/publications/i/item/9789240073890
- 7Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Análise de Situação em Saúde Sistema de Informações sobre Nascidos Vivos - SINASC: manual de procedimentos[Internet]Brasília Ministério da Saúde 2009 Sep 3, 2025160 p Série G. Estatística e Informação em Saúde Available at: https://bvsms.saude.gov.br/bvs/publicacoes/04_0098_M.pdf
- 8Noronha JC Lima LD Chorny AH Poz MR Gadelha P Brasil Saúde Amanhã: dimensões para o planejamento da atenção à saúde Rio de Janeiro Editora FIOCRUZ 2017