Inside the black box: Refining programme theory in the PriDem dementia care study
Sarah Griffiths, Emily Spencer, Louise Robinson, Greta Rait

TL;DR
This paper shows how refining the theory behind a dementia care program helps improve its effectiveness and scalability in primary care settings.
Contribution
The study provides a structured exemplar of program theory refinement after feasibility testing in dementia care.
Findings
Improved review processes and staff training were confirmed as key mechanisms for enhancing dementia care.
New mechanisms like mapping local services and using dementia review templates were identified as important for implementation.
Role ambiguity and capacity concerns were found to impede successful implementation.
Abstract
Refining programme theory following feasibility testing is a critical but rarely reported step in the development of complex interventions, creating a ‘black box’ in implementation science. This lack of transparency limits understanding of how and why interventions work and constrains effective scale-up and adaptation. This challenge is particularly salient in post-diagnostic dementia support, which is often fragmented in primary care, with limited guidance on how system-level interventions can be implemented and adapted in real-world settings. The PriDem programme developed a flexible, primary care-led intervention to improve post-diagnostic dementia support, involving Clinical Dementia Leads (CDLs) working with general practices to strengthen care systems. Programme theory was articulated in a logic model, to guide a feasibility implementation study, which demonstrated intervention…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
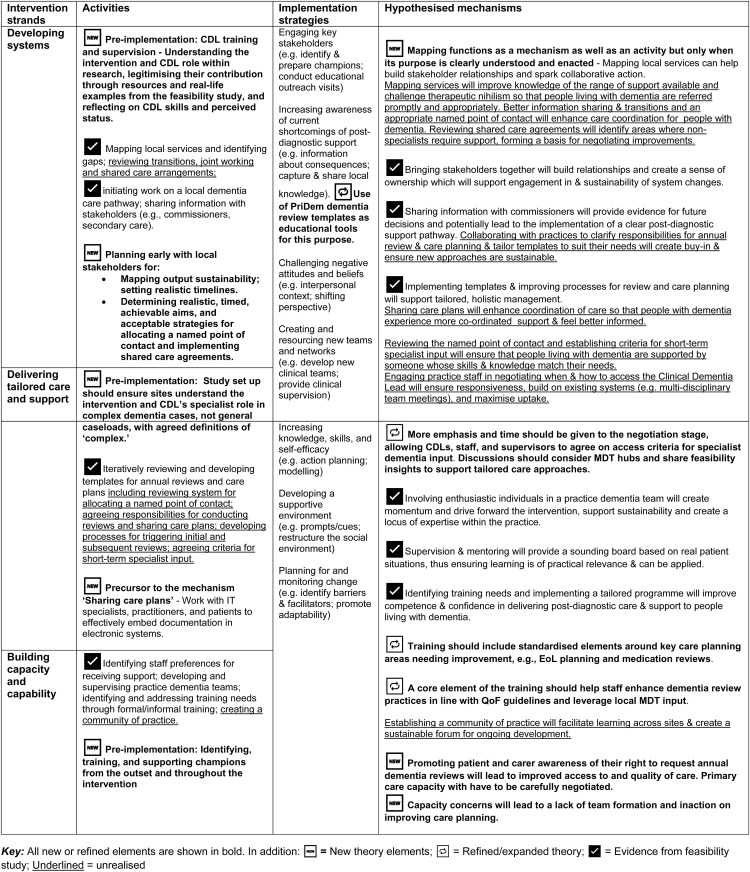 Figure 1
Figure 1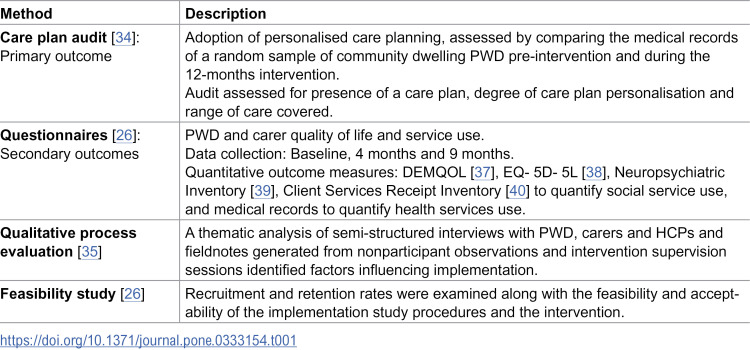 Figure 2
Figure 2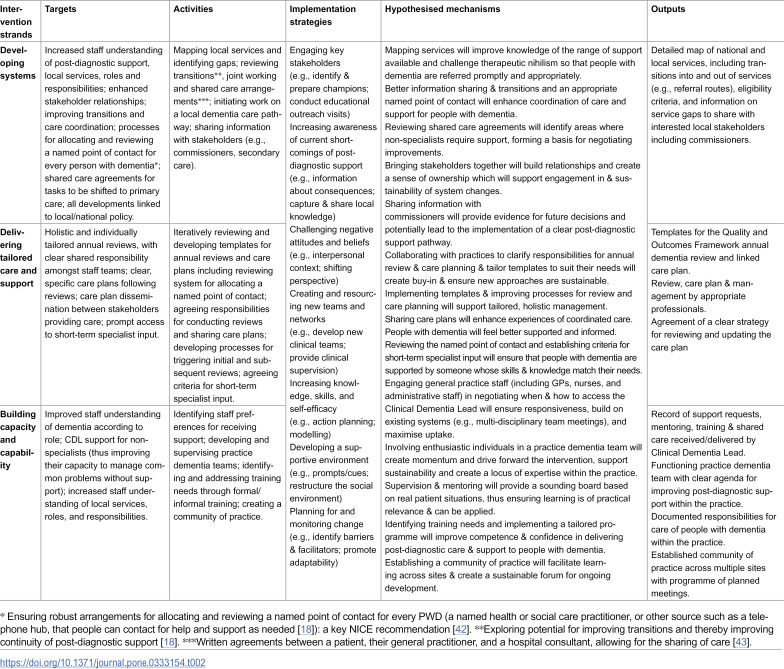 Figure 3
Figure 3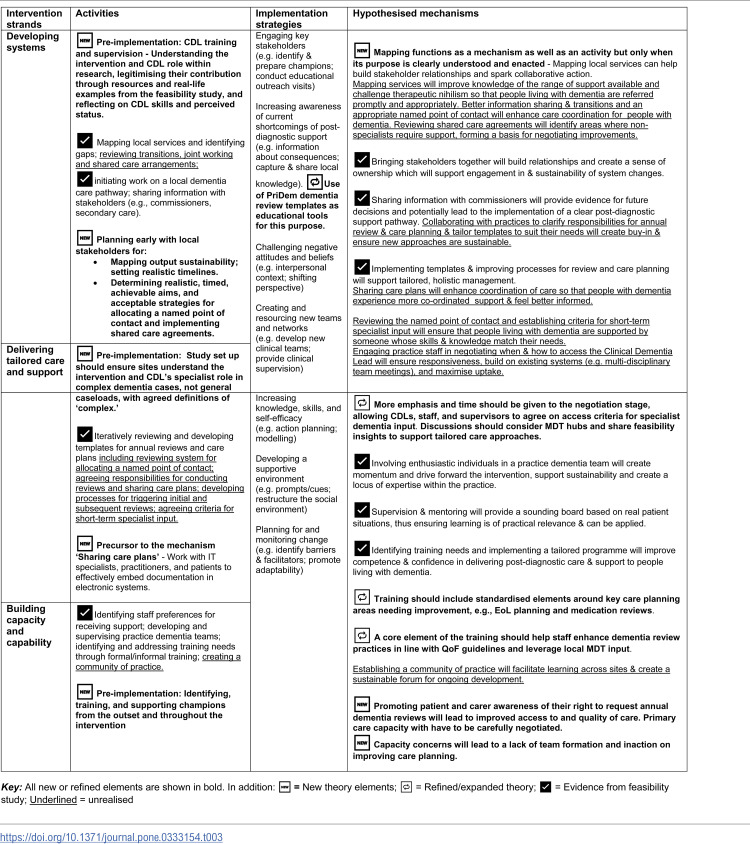 Figure 4
Figure 4- —Alzheimer's Society UK
- —Alzheimer's Society UK
- —Alzheimer's Society UK
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Policy Implementation Science · Mental Health and Patient Involvement · Dementia and Cognitive Impairment Research
Introduction
Dementia is a progressive condition impairing memory, communication, and emotional regulation [1]. It is estimated that over 900,000 people in England and Wales are affected, with projections reaching 1.7 million by 2040 and care costs rising from £34.7 to £94.1 billion [2,3]. Traditionally led by secondary care, post-diagnostic support is often inadequate, unaffordable, and poorly integrated [4,5]. International policy [6–8] and research [9–12], increasingly advocate for primary care coordination to enhance service access and quality of life for people with dementia (PWD) and their carers [13].
The PriDem research programme (2018–2023) co-developed a primary care-led intervention with PWD, carers, and professionals to improve post-diagnostic dementia care. Adaptable to individual practice needs, the intervention involved Clinical Dementia Leads (CDLs); health professionals with dementia expertise, supporting primary care teams to strengthen their care delivery systems, provide tailored and holistic care and support, and build capability and capacity (including bespoke training) within the primary care workforce. Guided by evidence reviews [14–16] and qualitative research [17,18], the intervention aimed to create local systems-level change [19], with indirect benefits for PWD and carers [20].
Implementing dementia care interventions is complex, requiring staff time reallocation, workload adjustments, and organisational support [21,22]. A well-developed programme theory supports evaluation by identifying implementation barriers, facilitators, and sustainability strategies [22,23]. To guide implementation, a logic model (S1 File in S1 Text) was developed; a visual map of our programme theory [23], to address challenges in post-diagnostic care, including inconsistent annual dementia reviews and care planning [24,25]. Following guidance on complex intervention evaluation [23], we then modelled the intervention, conducting a feasibility implementation study to assess change mechanisms and contextual factors [26].
Intervention development best practice involves reflecting on feasibility findings to refine programme theory and guide intervention uptake [22]. However, there is limited transparent reporting on this process of reflecting on and iterating programme theory [27], making it difficult to evaluate how and why programmes are adapted over time, and creating a ‘black box’ effect [28,29]. This article provides an example of how feasibility findings can be used to reflect on and refine programme theory.
Aims
Present an exemplar of using feasibility implementation findings to reflect on intervention programme theory.
- Hypothesise refinements to PriDem intervention theory, to inform a large-scale implementation study.
Methods
Design
A 15-month multi-site, mixed methods feasibility implementation study, was informed by implementation research design tool ImpRes [30] and StaRI reporting standards [31]. A ‘Hybrid Effectiveness-Implementation’ design [32] was adopted, whereby the primary aim was to determine the impact of the implementation strategies, and a secondary aim was to assess outcomes. The current paper reports a secondary, theory-focused qualitative analysis drawing on data generated within this feasibility implementation study. Detailed information on methods and intervention development has been reported extensively elsewhere [20,26,33–35]. This article follows Standards for Reporting Qualitative Research (SRQR – see S2 File in S1 Text) [36].
Ethics
Ethical approval for the study was obtained from the Health Research Authority and Wales REC 4 of the National Research Ethics Service (21/WA/0267). As part of the approved procedure, written or verbal informed consent was obtained for all study participants. Where verbal consent was obtained, this was audio recorded, witnessed and documented in writing by a researcher. The document and audio file were stored on a secure university data management system.
Setting and participants
Seven general practices were recruited, three in the Southeast and four in the Northeast of England. From practice patient lists and staff, 60 community dwelling PWD, 51 carers and 26 healthcare professionals (HCPs) were recruited between 18^th^ March 2022 and 15^th^ May 2023. Two CDLs, with nursing backgrounds, delivered the intervention over 12 months, one per region, working with practices. They followed an intervention manual, received bespoke PriDem training, clinical supervision from a dementia nurse specialist, and regular sessions with the supervisor and research team.
Original study overview
The PriDem feasibility implementation study comprised four main elements (Table 1).
Table 1: PriDem feasibility implementation study elements and data collection.
We have previously reported findings from these elements, summarised in S3 File in S1 Text.
Current study analysis
This paper revisits the programme theory outlined in the initial logic model following feasibility testing. While intended outcomes remain unchanged, the focus here is on the underlying theory, specifically, how outcomes are expected to be achieved. It examines three overlapping intervention components, referred to in the logic model as strands, each with key targets, activities to be led by CDLs, implementation strategies [41], and hypothesised mechanisms of change (Table 2).
Table 2: PriDem Programme Theory – Three intervention strands, with associated targets, activities, implementation strategies, hypothesised mechanisms and outputs.
We synthesised previously published findings with new insights from feasibility study data, using a fresh analytic lens: exploring how this combined evidence could refine intervention theory in the logic model. Data sources included qualitative interviews, fieldnotes, supervision notes, and researcher reflections, with full details of these sources reported elsewhere [33,35].
In line with established guidance, we used the logic model represented in Table 2 as a living framework for theory refinement [46]. Guided by established approaches to qualitative analysis for evaluating, expanding, and refining theory [44,45], we conducted a deductive thematic analysis, in which coding and theme development were informed by pre-existing theory [44]. The logic model served as a coding framework, and the theory was subsequently adapted based on mismatches, newly identified mechanisms, and negative cases.
Theory refinement process
Decisions about refining the programme theory and logic model were made by the core research team (SG, ES, LR, GR). The process was iterative and collective: interpretations were discussed in regular analytic meetings. Consensus was sought regarding whether theoretical elements should be retained, refined, or newly proposed. Where interpretations differed, discussions returned to the data and the original programme theory to assess explanatory coherence and plausibility.
Findings are presented below. Previously published findings from the PriDem study are cited where necessary for context and to justify proposed refinements to the logic model. Novel insights that have not appeared in prior published work are supported by quotations from the data.
Findings
Findings are presented by intervention strand (‘Developing Systems,’ ‘Delivering tailored care and support’ and ‘Building capacity and capability’). Key activities, implementation strategies, mechanisms and intended outputs for each strand are shown in Table 2. We conclude this section by incorporating findings within relevant areas of the original logic model (Table 3).
Table 3: Hypothesised refinements to the PriDem logic model.
Developing systems
This strand addressed gaps in infrastructure supporting primary care-led post-diagnostic dementia care. Insights from this strand suggest refinements to the intervention theory, as follows.
Mapping as an evolving intervention mechanism.
• Initial uncertainty: mapping as a poorly understood activity
An early activity undertaken by CDLs was to map locally available post-diagnostic dementia services, with the intended aim of identifying gaps in provision, informing commissioners and primary care teams, and supporting dementia care pathway development. However, CDLs initially struggled to understand the purpose and remit of this mapping activity. Some were uncertain whether mapping was a clinical task, a research exercise, or an administrative function, which undermined confidence and delayed progress.
‘It kind of made sense as a research nebulous document - but how it would translate clinically into practical tasks…the mapping was really daunting for me. I didn’t really have, I thought, the skills to do it.’ (Interview PROF-01: CDL)
CDLs also questioned the value of mapping, assuming that primary care teams already knew available services or that directories already existed. This uncertainty was compounded by their ambiguous position within a research-led intervention, which affected perceived legitimacy and authority when contacting services:
‘Why am I…doing something I have no skills and no remit to do, I’ve got no authority. These people are wondering who’s this person who’s a researcher…ringing me to ask me personal stuff about my service, so I don’t have a remit, authority, managerial line for all these organisations.’ (Interview PROF-01: CDL)
In response, CDLs often relied on prior clinical experience to make sense of the task. While this familiarity initially increased confidence, it also risked narrowing understanding of the mapping activity’s specific purpose within the intervention. For example, whilst relationship building is integral to carrying out the mapping exercise, one CDLs framed mapping primarily as a relationship-building exercise rather than as a structured intervention designed to generate tangible outputs and inform system-level change:
‘I think it’s been quite easy to understand the service mapping because that is something that I’ve done before in other roles….to see what is in the local community and to develop links and relationships with the services. So that’s relatively easy.’ (Interview PROF-04: CDL)
This partial understanding functioned as a negative mechanism, whereby assumptions of familiarity limited learning about the distinctive aims and outputs required, contributing to variability in early mapping efforts and delays in progress.
• Mapping in practice: from activity to mechanism
As the intervention progressed, mapping evolved from a misunderstood activity into a mechanism that actively enabled engagement, coordination, and system-level action. Beyond producing a service map, the process of contacting organisations, gathering information, and feeding back findings facilitated relationship-building, shared awareness, and collaborative problem-solving.
For one CDL, mapping functioned as a relational mechanism that connected organisations previously working in silos and prompted joint action:
‘… it’s putting organisations in contact with each other because they’re all working in silos…saying, look….you’re running an education group for carers, the council already have three years’ experience doing that. Why don’t you talk to each other.… mapping turned out to be a good mechanism to engage.’ (Interview PROF-01: CDL)
In this case, mapping enabled identification of service gaps, supported improved referral routes to dementia advisors, and highlighted system issues affecting service transitions and emergency care demand. Outputs included a detailed service map shared with primary care teams and commissioners, alongside a condensed ‘desktop directory’ for GPs. Mapping also provided a platform for CDL involvement in commissioner-led care pathway planning, reinforcing its role as a mechanism for system-level engagement.
However, mapping was enacted differently across sites. One CDL worked with an existing public-facing website to improve the accessibility and quality of dementia information, responding to strong preferences from primary care practitioners:
‘When [CDL] first started, myself…all different [staff] kept saying, go to [website] for [City]…So [CDL]…worked with them to make sure the dementia information was up to scratch, helped them write some bits…and then brought that back to the GPs.’ (Interview PROF-13 GP)
While this approach supported community-facing information sharing, it risked missing detail on NHS and social care services. In this context, the CDL relied more heavily on research evidence, rather than mapping itself, as a mechanism to influence strategic development, particularly in relation to an emerging regional dementia strategy.
Taken together, these findings demonstrate that mapping functioned both as an intervention activity and as a mechanism, but only when its purpose was clearly understood and actively enacted. Early confusion and assumptions of familiarity constrained its effectiveness, while later engagement revealed its potential to facilitate relationships, shared understanding, and coordinated system change. Future implementation should explicitly support CDLs to understand both the intended outputs of mapping and the mechanisms through which it can drive collaborative change.
New pre-implementation activity - CDL training and supervision.
Although we developed and delivered a tailored CDL training and supervision programme, including a practitioner manual, this support for CDLs was not included in our original theory. However, early pre-implementation activities, such as training, are often essential components of a logic model, helping to build readiness, and increase the chances of effective implementation [46]. Insights from our feasibility study highlight the need to add pre-implementation activities to our theory, including training and supervision.
Training and supervision need to help CDLs understand the intervention and their role within a research project and highlight the importance of avoiding assumptions around key activities such as mapping, as shown above.
‘[Clinical supervisor] warns against assuming people know what’s available. Do they refer appropriately, or default to familiar options? Even if staff seem knowledgeable, don’t assume. The map helps ensure timely, informed referrals—practice teams are the key audience. Not all answers lie in existing directories.’ (Intervention supervision notes)
Through intervention supervision, an introductory leaflet for stakeholders was co-developed by CDLs, researchers and the intervention supervisor (senior clinician providing oversight and support to CDLs), explaining the project, the CDL role and the mapping, and highlighting benefits for stakeholders. This simple resource helped establish CDL legitimacy and could be included in future training.
Concrete ‘real life’ examples from our feasibility study can be used in future training and supervision to show how the intervention works in practice. Training could also explore CDL skills, perceived status, and roles (e.g., factfinder, influencer) as mechanisms supporting outcomes.
New activity – Planning early with local stakeholders for.
• Mapping output sustainability
The sustainability of service mapping was a concern for both CDLs.
‘If I create a directory, it’s as current as it is the day I’ve written it.’ (Interview PROF-04: CDL)
By the intervention’s end, a local services map was available on an NHS trust website in one of the regions, with discussions underway to integrate it into general practice systems. However, concerns about ongoing maintenance arose, with social prescribers (primary care–based staff who link patients to community and voluntary sector services) suggested for oversight. The CDL was unable to support this due to the time-limited nature of the intervention.
These findings highlight the need to explicitly incorporate sustainability planning into the programme theory. Accordingly, we propose adding a new activity to the logic model: planning early with local stakeholders for mapping output sustainability and setting realistic timelines.
• Allocating a named point of contact and shared care agreements
There was limited progress on influencing systems for allocating and reviewing a named point of contact for every person with dementia, despite PWD and carers welcoming the idea.
‘I just think you might feel a bit more held.’ (Interview C-01: Carer)
CDLs raised the need for named points of contact, but capacity and time constraints hindered system development. Although Dementia advisors and social prescribers were considered for the role, this was not implemented in either region.
The issue of shared care agreements (formal arrangements outlining roles and responsibilities across services) was raised in CDL training:
‘[The CDL’s Clinical Supervisor] advised shared care agreements tend to be medication focused rather than around other interventions. Key questions will be do people know the shared care agreement exists, resource issues, how concerns/queries are raised when using it.’ (Researcher reflections on CDL training)
However, shared care agreements were not identified as a development priority in either region. Reviewing named point of contact systems and shared care agreements was not achievable within the scope of a 12-month intervention.
For future implementation, early stakeholder consultation could help define realistic, time-bound goals and suitable strategies.
Delivering tailored care and support
This strand aimed to strengthen post-diagnostic dementia support by addressing gaps in holistic care, the use of standardised templates to structure dementia reviews, and anticipatory care planning. Implementation challenges informed theory refinement, with key learning points outlined below.
Refined Implementation strategy - Use of PriDem dementia review templates as educational tools.
Our theory included raising stakeholder awareness of gaps in post-diagnostic support, originally proposed to happen through case note reviews at two time points. Due to staff capacity issues, CDLs struggled to implement this [34]. Instead, an adaptable PriDem resource pack with review templates (see S4 File in S1 Text), developed early in the study by researchers, proved effective educational tools. CDLs modelled their use by conducting reviews with patients, demonstrating the value of a holistic MDT approach.
‘[I said] to the GPs “Oh look, I tried this, and then I could embed the tools into that patient’s notes.” So, it was a like a hook for a GP to say, “I like that review. That was really good.” And then, “Oh but…I couldn’t spend an hour on one patient. Oh but …the receptionist does this bit and the… social prescriber could do that bit…and then maybe I could do my bit.” …So that was…a way for me to say, “Look, this is going to help you because no one’s going to be doing extra work.’ (Interview PROF-01: CDL)
Talking through the template was a vehicle for planning new approaches to team working:
‘It’s been really helpful trying to work with [CDL] on the skill mix of… a community team, … [CDL]’s given us the template and tried to help us with the staff mix. And then we’ve looked at what we’ve actually got on the ground and how we can adjust our team to try and accomplish that template as best we can.’ (Interview PROF-18: GP)
A future theory iteration should incorporate use of PriDem dementia review templates as educational tools within the range of available implementation strategies.
Refined mechanism – Engaging practice staff in negotiating when and how to access the CDL.
CDLs were expected to hold a small caseload of complex dementia cases, offering short-term specialist input and modelling good practice. This was to be guided by negotiated criteria with general practice staff (Table 2). In reality, defining the CDL clinical role proved complex, with little evidence of effective negotiation. Some staff viewed CDLs as an extra resource for managing the full dementia caseload, rather than as agents of systemic change [35]. One CDL addressed this by directing referrals to an existing MDT, with a different but related specialty to dementia, using its established referral processes and multidisciplinary discussion as a means of promoting learning that can be applied in practice.
.‘I utilised the [specialist MDT] infrastructure and said, can you refer via [them]?...it’s a good place for me to…work out what their needs are then take that back to the [specialist MDT] and demonstrate the PriDem [approach]… and all the GPs are sitting there. So, then they take that learning for the next patient they see.’ (Interview PROF-01: CDL)
This aligns with our mechanism of negotiating referral criteria, which incorporates building on existing systems, however, the approach lacked flexibility when there was an urgent need, and did not allow for proactive, timely, and tailored input.
‘One of the GPs raised a patient she had seen recently with complex needs, who had bitten her husband while in the surgery waiting room. CDL suggested referring the patient to the [specialist MDT]…for a meeting in one week. Researcher reflection: This seems like a missed opportunity…a patient who could use quick input with a dementia-specific focus…This seems the exact sort of complex case that we envisaged the CDL taking on.’ (Observation of practice meeting)
Lack of negotiation in this case led to both the CDL and practice staff feeling unsupported.
CDLs often expressed uncertainty in supervision, around the amount of direct patient contact expected as part of their roles and the definition of a complex case. Whilst not formally defined, this was described by the supervisor as follows:
‘It would be like be when there is perhaps lots of co-morbid conditions and there’s perhaps challenging relationships, or there’s a lack of engagement.’ (Interview PROF-15: CDL Supervisor)
To address these issues, more emphasis and time could be given to the negotiation stage, where CDLs, practice staff and supervisors agree processes and criteria for accessing specialist dementia input, in a framework within which CDLs also feel supported by the practices and satisfied in their work.
Contextual infrastructure such as existing MDTs could be discussed, in terms of whether and how they can support specialist dementia input. As part of our study, some practices developed innovative approaches to delivering tailored care and support, such as One Stop Shop MDT dementia review clinics [35,47]. Future implementation can include sharing these innovations with CDLs and practice staff as illustrative case studies, thereby supporting care delivery decision-making.
New pre-implementation activity - Study set up.
Effective negotiation depends on a clear understanding of the intervention’s purpose, which some general practice staff lacked [35]. Future implementation studies should build in more time for educating practice staff and CDLs about the intervention’s nature and the CDL role, fostering a shared understanding. These activities should be included in pre-implementation activities.
Refined mechanism - Identifying training needs and implementing a tailored programme: Targeting specific areas of care.
Although the feasibility study showed improvements in care planning [26], some areas of care saw less change in representation within care plans, such as medication reviews, and end of life (EoL) planning [34]. Given the need to minimise polypharmacy [48] and the challenges of timing EoL discussions [49] future iterations of the intervention could target these specific areas through the mechanism of CDL-led staff training.
New mechanism – Promoting patient and carer awareness.
PWD and carers are typically unaware of their entitlement to an annual review [34]. While their role in care delivery was not part of our intervention theory, raising patient awareness of their rights could be a powerful mechanism for improved care, empowering patients and carers to request holistic reviews. This would require careful negotiation of primary care capacity to support increased uptake and provision. We saw evidence of buy-in from some staff, who anticipated that spending more time improving review quality would offer long-term efficiency gains, by enhancing anticipatory care [47].
New activity – Precursor to the mechanism ‘Sharing care plans’.
Our logic model proposes that sharing care plans between practitioners, PWD and carers enhances care coordination. However, this rarely occurred, largely due to the lack of integrated electronic record systems [34]. The PriDem care plan template was not shared with patients as was intended, with practitioners reporting that recording care plans on IT systems as well as creating patient-friendly versions was too burdensome:
‘The [PriDem care plan template]…we didn’t really use…it’s a really nice concept, but not logistically achievable to document on your own computer system, which is your Medico-Legal note…and then…create a written care plan.’ (Interview PROF-06: GP)
Intervention theory should include activities to support care plan sharing, involving collaboration with primary care IT specialists, practitioners, and patients to embed documentation in electronic systems effectively.
Building capacity and capability
This strand tackled key challenges in primary care dementia support, such as limited training, inconsistent specialist input, and low staff confidence. We identified the following theory refinements.
New pre-implementation activity – Identifying, training, and supporting champions.
Champion identification was a key implementation strategy, with champions proving instrumental in driving meaningful change and supporting programme theory. However, not all practices were able to identify champions, highlighting the need for early identification and sustained support during pre-implementation and beyond. In one practice, running One Stop Shop MDT clinics helped sustain a dementia team:
‘Running the one stop shops has probably been one of the key ways of maintaining that… there’s a kind of focus for the team to come together… building an interest and upskilling going forward.’ (Interview PROF-06: GP)
This team continued beyond the study, independent of CDL input, driven by committed champions. Strong leadership and a shared purpose, beyond simply improving dementia care, helped the team thrive. This aligns with the need for ‘clear agendas’ (Outputs, Table 1).
New mechanism – Capacity concerns limiting team formation and care planning.
While our theory acknowledges capacity as a contextual factor, new insights suggest it also acts as a mechanism that can hinder team formation and care planning. Although the PriDem approach aimed to optimise existing resources [26], limited staff capacity and lack of funding were major concerns in some practices.
CDLs often engaged champions informally, but staff were reluctant to create formal teams due to workload concerns.
‘The perception is that this would be a big task… it would probably need some sort of resourcing to make it attractive.’ (Interview PROF-02: GP)
One CDL noted that calling groups ‘dementia teams’ was counterproductive, as it implied extra work. Instead, they engaged individuals based on enthusiasm and availability, without explicitly labelling them as a team. This helps explain the discrepancy between the CDL’s perception that practice dementia teams were operating and the fact that those involved did not identify themselves as team members, indicating differing understandings of what constituted a ‘team’ within the intervention.
Capacity concerns also affected care planning. Despite progress in care planning, time constraints limited holistic reviews. Many practitioners were unaware that the Quality and Outcomes Framework (QoF) guidelines [50], an annual incentive program for GP practices in England, proposed up to 30 minutes for dementia reviews.
‘How do you integrate that into a normal 10-minute appointment?’ (Interview PROF-13: GP)‘They’ve got 10-minute appointments, got to try and cram in as much as they can and for a dementia review, it takes much longer.’ (Interview PROF-20: Social Prescriber)
These challenges suggest that without adequate time, team structures and awareness of guidelines, long-term sustainability and quality care planning are at risk.
Refined mechanism - Identifying training needs and implementing a tailored programme: Training should help staff enhance dementia review practices in line with QoF guidelines and leverage local MDT input.
To mitigate challenges outlined in this strand, we propose that CDL-led staff training and awareness initiatives should go beyond skill-building to include strategies for refining dementia review approaches based on current QoF guidelines, MDT support, and leadership-driven team cohesion.
Refining the logic model.
Table 3 integrates findings into the logic model, indicating which theoretical elements were supported, newly proposed, refined or expanded and which remained unrealised due to the limitations of the study timeline or lack of staff capacity.
Discussion
We have presented a detailed reflection on the feasibility implementation of the PriDem intervention, offering critical insights for refining programme theory and informing future large-scale implementation. Findings highlight challenges of translating theory into practice, including role clarity, training, and system integration. This supports guidance emphasising iterative theory refinement in developing complex interventions [23].
Theory components confirmed, refined, and newly identified
Many original theory elements were supported. For example, enthusiastic individuals drove momentum, templates and improved review processes enhanced care plan personalisation, and staff training increased confidence and competence in care delivery.
In addition, we identified new theoretical components and refined existing ones. Mapping emerged not only as a planned activity but also as a mechanism for interdisciplinary collaboration and service improvement; an intervention diffusion effect (the largely unplanned spread and uptake of an intervention through social and organisational networks over time, beyond its initial development or evaluation context) [51,52]. Templates, beyond standardising holistic care, functioned as educational tools to challenge therapeutic nihilism and support team-based planning. This contributes to primary care knowledge sharing literature [53] by highlighting the need to tailor resources in ways that feel relevant and acceptable to users.
Our refined programme theory includes negative mechanisms; factors that actively hindered implementation. For instance, CDL uncertainty about mapping delayed progress, while unclear roles and perceived lack of role legitimacy limited early stakeholder engagement. These mechanisms, absent from the original theory, reveal active processes disrupting outcomes, thereby strengthening the logic model’s explanatory power for future implementation, by making unintended and constraining consequences of intervention delivery visible, as advocated in evaluation theory [54].
Capacity constraints and organisational readiness evidenced in the findings through staff workload pressures, leadership engagement, role clarity, and supporting infrastructure, were influential contextual factors, but our analysis suggests these also function as mechanisms, shaping staff engagement, care planning practices, and sustainability potential. This highlights the need for implementation theory to incorporate not just resource realities but also how actors make sense of, enact, or resist those realities in practice, as emphasised in normalisation process theory [55]. Future studies could apply empirical evidence on resistance to change, to better understand behavioural responses to implementation demands [56] and examine the contextual and cultural conditions that enable sustained change, including the selection of appropriate behaviour change strategies [57].The role of CDLs in negotiating their clinical input emerged as an area needing refinement. While the logic model assumed joint planning of referral processes, this proved challenging. There is a need for clearer role negotiation processes, underpinned by supportive structures such as existing MDTs and primary care digital systems. Role clarity and decision-space (defined here as the scope of autonomy and authority available to CDLs within local systems) have previously been identified as key determinants of implementation success [58,59] with lack of clarity a key source of team friction.
Implications for future implementation
Our findings advocate for the inclusion of pre-implementation activities in programme theory [46], including CDL training and supervision, study set up activities focused on ensuring understanding of the intervention, and early champion identification. Individuals with a commitment to dementia care and strong leadership qualities, such as persuasiveness and collaboration, can help overcome resistance, break down silos, and foster implementation success when supported from the outset [60]. We have previously highlighted the importance of embedding CDLs in practices through physical space and visible presence [26]. Strategies to achieve this should be part of pre-implementation negotiations with practices. Sustained engagement of stakeholders to jointly set realistic goals and timelines is essential for future success of implementing aspects such as allocating named points of contact and sharing care plans. Engagement of stakeholders responsible for IT systems and workforce development is important for supporting activities such as care plan sharing and MDT-based reviews.
The revised logic model (Table 3) identifies aspects yet unrealised, such as strategies for shared care agreements and establishing a community of practice. This will help guide future inquiry and consequent theory iteration. Given the variable success of dementia practice teams, future implementation might consider dementia support teams across a wider area spanning primary, social and secondary care within a locality. This could prove a powerful mechanism for improving those aspects yet unrealised, as well as supporting the sharing of care plans between services.
Although our original theory did not account for the role of patients or carers in service delivery, given the systems-level approach, through conversations with research participants, we began to see the potential in empowering people with dementia and their carers to actively request a holistic dementia review and care plan. This led us to hypothesise that such an approach could help improve access to and quality of care. It also opens the possibility of evaluating the impact of a patient awareness-raising mechanism.
Future large-scale implementation and effectiveness studies will be important not only to test refined mechanisms but also to streamline the logic model by identifying which components are essential and which can be removed. Ahead of future implementation, it will also be essential to incorporate current contextual factors and national guidelines, particularly those outlined in the government’s 10-Year Dementia Plan [8] and the wider Health Plan for England [61], which both highlight a strategic shift toward community-based, integrated care models to better support people with dementia.
Strengths and limitations
We address a recognised gap in implementation science, where theoretical assumptions are often underreported or insufficiently tested, contributing to the ‘black box’ problem in complex interventions [28,29]. Our synthesis draws on multiple data sources – qualitative interviews, fieldnotes, supervision notes, and researcher reflections – viewed through a logic model lens. This strengthens the revised programme theory and supports its potential transferability to other primary care-based dementia interventions.
While no new empirical data are presented, the article integrates feasibility findings to reflect on theory development. As such, insights are context and time specific, and some original theoretical components remain unrealised, speculative, and flagged for future research, either due to the short-term nature of the intervention, or limited capacity within the workforce.,. Despite these limitations, the paper offers a strong example of iterative theory development, promoting greater transparency and reproducibility in designing and implementing complex health interventions.
Conclusion
This study demonstrates the value of systematically reflecting on and iterating programme theory in complex intervention research. Our analysis bridges the ‘black box’ of intervention delivery and theory refinement, offering a transparent model for others seeking to optimise dementia care or similarly complex interventions. By adapting theory to practice-informed insights, we enhance the likelihood of effective, scalable, and sustainable implementation in primary care-led dementia support.
Supporting information
S1 TextS1 File. PriDem Logic Model. S2 File. Standards for Reporting Qualitative Research (SRQR) Checklist. S3 File. Summary of evaluation findings already shared. S4 File. Adaptable PriDem resource pack with review templates.(ZIP)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1NHS. About dementia: dementia guide 2020. https://www.nhs.uk/conditions/dementia/about/
- 2Chen Y, Bandosz P, Stoye G, Liu Y, Wu Y, Lobanov-Rostovsky S, et al. Dementia incidence trend in England and Wales, 2002–19, and projection for dementia burden to 2040: analysis of data from the English Longitudinal Study of Ageing. The Lancet Public Health. 2023;8(11):e 859–67.10.1016/S 2468-2667(23)00214-1PMC 1095898937898518 · doi ↗ · pubmed ↗
- 3Wittenberg R, Hu B, Barraza-Araiza L, Rehill A. Projections of older people with dementia and costs of dementia care in the United Kingdom, 2019–2040. London: London School of Economics. 2019.
- 4Bourne J. Improving services and support for people with dementia. National Audit Office. 2007.
- 5Morse A. Improving dementia services in England—an interim report. London: National Audit Office. 2010.
- 6Kane MTG. Dementia 2015: aiming higher to transform lives. London: Alzheimer’s Society. 2015.
- 7Long S, Benoist C, Weidner W. World Alzheimer Report 2023: Reducing dementia risk: never too early, never too late. London: Alzheimer’s Disease International. 2023.
- 8DHSC. Health Secretary announces 10-year plan for dementia. 2022. https://www.gov.uk/government/news/health-secretary-announces-10-year-plan-for-dementia