Retrospective analysis of adverse drug reaction patterns from the national monitoring system in a tertiary care hospital in China (2019–2024)
Xiao-Lei Yuan, Xiao-Yu Fang, Feng Li, Feng-Jun Wang, Qian-Qian Ma, Jun-Tao Chen, Ya-Nan Wang

TL;DR
This study analyzed adverse drug reactions in a Chinese hospital from 2019 to 2024, identifying antineoplastic drugs and intravenous administration as major risk factors.
Contribution
The study highlights antineoplastic agents and intravenous routes as significant ADR risk factors and suggests improved monitoring and protocols.
Findings
Antineoplastic agents were the most common cause of ADRs (34.2%).
Intravenous infusion was the leading administration route for ADRs (67.3%).
Pharmacists became the primary reporters of ADRs by 2024 (93.1%).
Abstract
To characterize the patterns, risk factors, and reporting trends of adverse drug reactions (ADRs) in a tertiary care hospital in China to inform targeted medication safety interventions. A single-center, retrospective analysis was conducted on 5,564 ADR reports extracted from the National Adverse Drug Reaction Monitoring System (2019–2024). Reports were assessed for causality using the WHO-UMC criteria. Descriptive statistics and chi-squared tests were employed to analyze demographics, reporting trends, causative drugs, administration routes, and clinical outcomes. The mean patient age was 62.4 years, with males slightly predominating (52.5 %). ADR reporting increased markedly over the study period, with pharmacists becoming the primary reporters (93.1 % in 2024). Intravenous infusion was the most common route (67.3 %). Antineoplastic agents were the predominant drug class implicated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
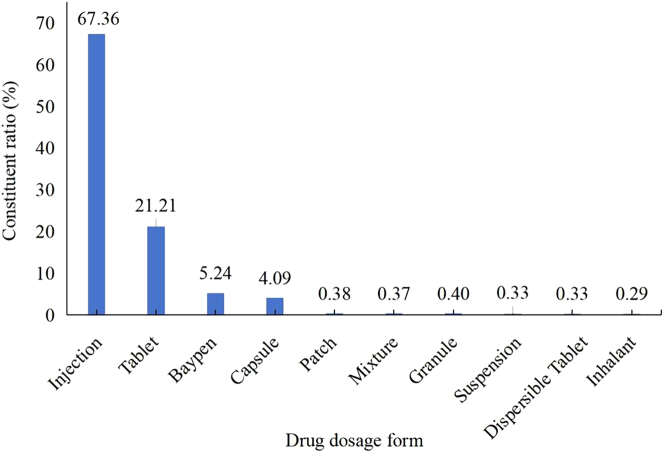 Figure 1
Figure 1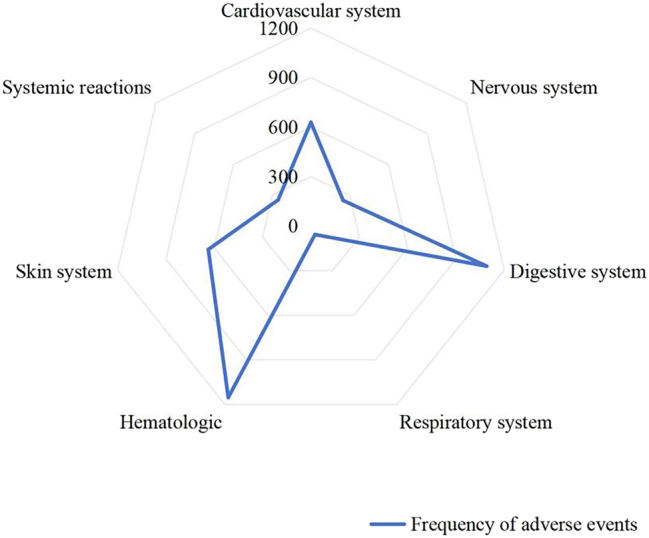 Figure 2
Figure 2| Groups | n (%) | |
|---|---|---|
| Gender | Male | 2,920 (52.48) |
| Female | 2,644 (47.52) | |
| Past ADR history | Yes | 196 (3.52) |
| No | 491 (8.82) | |
| Not quite clear | 4,877 (87.65) | |
| Special medical histories and lifestyle profiles | Smoking history | 71 (1.28) |
| Alcohol use history | 61 (1.11) | |
| Past medical history | 244 (4.39) | |
| Other | 5,188 (93.24) | |
| Year | New/Serious ADRs n (%) | Non-seriousADRs n (%) | Total n (%) |
|---|---|---|---|
| 2019 | 151 (5.60) | 369 (12.87) | 520 (9.35) |
| 2020 | 247 (9.16) | 390 (13.60) | 637 (11.45) |
| 2021 | 231 (8.57) | 807 (28.15) | 1,038 (18.66) |
| 2022 | 552 (20.47) | 589 (20.54) | 1,141 (20.51) |
| 2023 | 719 (26.66) | 430 (15.03) | 1,149 (20.65) |
| 2024 | 797 (29.55) | 282 (9.83) | 1,079 (19.39) |
| Total (n %) | 2,697 (48.47) | 2,867 (51.53) | 5,564 (100.00) |
| Age, years | Male n (%) | Female n (%) | Total n (%) |
|---|---|---|---|
| ≤18 | 64 (2.19) | 48 (1.82) | 112 (2.01) |
| 19–29 | 84 (2.88) | 76 (2.87) | 160 (2.88) |
| 30–39 | 142 (4.86) | 136 (5.14) | 278 (5.00) |
| 40–49 | 234 (8.01) | 221 (8.36) | 455 (8.18) |
| 50–59 | 508 (17.40) | 598 (22.62) | 1,106 (19.88) |
| 60–69 | 663 (22.71) | 578 (21.86) | 1,241 (22.30) |
| 70–79 | 918 (31.44) | 654 (24.74) | 1,572 (28.25) |
| ≥80 | 307 (10.51) | 333 (12.59) | 640 (11.50) |
| Total n (%) | 2,920 (52.48) | 2,644 (47.52) | 5,564 (100.00) |
| Year | Reporting sources | Total n (%) | ||
|---|---|---|---|---|
| Physician n (%) | Pharmacist n (%) | Nurse n (%) | ||
| 2019 | 6 (1.15) | 9 (1.73) | 505 (97.12) | 520 (9.35) |
| 2020 | 90 (14.13) | 198 (15.38) | 349 (54.79) | 637 (11.45) |
| 2021 | 95 (9.15) | 683 (65.80) | 260 (20.05) | 1,038 (18.66) |
| 2022 | 84 (7.36) | 1,035 (90.71) | 22 (1.93) | 1,141 (20.51) |
| 2023 | 96 (8.36) | 1,034 (89.99) | 19 (1.65) | 1,149 (20.65) |
| 2024 | 60 (5.56) | 1,004 (93.05) | 15 (1.39) | 1,079 (19.39) |
| Total n (%) | 431 (7.75) | 3,963 (71.22) | 1,170 (21.03) | 5,564 (100.00) |
| Route of administration | Number of cases n (%) |
|---|---|
| Intravenous infusion | 3,719 (67.34) |
| Oral administration | 1,498 (27.12) |
| Subcutaneous injection | 65 (1.18) |
| Intra-pump infusion | 60 (1.09) |
| Intravenous injection | 59 (1.07) |
| Intramuscular injection | 48 (0.87) |
| Inhalation | 36 (0.65) |
| Topical application administration | 25 (0.45) |
| Intra-arterial administration | 13 (0.24) |
| Hepatic arterial infusion | 9 (0.16) |
| Total | 5,523 (100.00) |
| Drug category | Number of cases n (%) | Major agents n (%) |
|---|---|---|
| Antineoplastic agents | 1,902 (34.18) | Carboplatin for Injection (185, 3.3 %), Gemcitabine Hydrochloride for Injection (132, 2.3 %), Oxaliplatin Injection (130, 2.3 %), Sintilimab Injection (115, 2.0 %), Capecitabine Tablets (114, 2.0 %), Cisplatin for Injection (112, 2.0 %), Paclitaxel Injection (108, 1.9 %), Albumin-Bound Paclitaxel for Injection (98, 1.7 %), et al. |
| Anti-infective agents | 598 (10.75) | Cefoperazone-Sulbactam for Injection (100, 1.7 %), Cefuroxime Sodium for Injection (81, 1.4 %), Ceftazidime for Injection (64, 1.1 %), Piperacillin-Tazobactam for Injection (44, 0.7 %), Ciprofloxacin Lactate and Sodium Chloride Injection (40, 0.7 %), Cefoxitin Sodium for Injection (35, 0.6 %), et al. |
| Cardiovascular agents | 524 (9.42) | Aspirin Enteric-Coated Tablets (50, 0.8 %), Rivaroxaban Tablets (32, 0.5 %), Furosemide Tablets (28, 0.5 %), Warfarin Sodium Tablets (27, 0.4 %), Rosuvastatin Calcium Tablets (26, 0.4 %), et al. |
| Neurological agents | 487 (8.75) | Sodium Aescinate Injection (84, 1.5 %), Citicoline Sodium Injection (62, 1.1 %), Betahistine Injection (47, 0.8 %), Ginkgo Diterpene Lactone Meglumine Injection (38, 0.6 %), Ginkgolide Injection (30, 0.5 %), et al. |
| Gastrointestinal agents | 332 (5.97) | Itopride Hydrochloride Dispersible Tablets (49, 0.8 %), Ranitidine Hydrochloride Injection (43, 0.7 %), Esomeprazole Sodium for Injection (28, 0.5 %), Pantoprazole Sodium for Injection (20, 0.3 %), Omeprazole Sodium for Injection (18, 0.3 %), et al. |
| Traditional Chinese medicines | 246 (4.42) | Sodium Aescinate Injection (84, 1.5 %), Ginkgo Diterpene Lactone Meglumine Injection (38, 0.6 %), Ginkgolide Injection (30, 0.5 %), et al. |
| Respiratory agents | 191 (3.43) | Doxofylline Injection (24, 0.4 %), Diprophylline Injection (24, 0.4 %), Ambroxol Injection (23, 0.4 %), Bromhexine Hydrochloride Injection (13, 0.2 %), Compound Methoxyphenamine Capsules (14, 0.2 %), et al. |
| Endocrine agents | 161 (2.89) | Metformin Hydrochloride Sustained-Release Tablets (14, 0.2 %), Ornithine Aspartate for Injection (9, 0.1 %), Letrozole Tablets (7, 0.1 %), Metformin Hydrochloride Tablets (7, 0.1 %), Miglitol Tablets (7, 0.1 %), et al. |
| Contrast media | 21 (0.38) | Iodixanol Injection (16, 0.2 %), Compound Meglumine Diatrizoate Injection (3, <0.1 %), Gadopentetate Dimeglumine Injection (2, <0.1 %) |
| Neurological agents | 1,102 (19.81) | Mannitol Injection (64, 1.1 %), Lactated Ringer’s Injection (52, 0.9 %), Lornoxicam for Injection (52, 0.9 %), Compound Amino Acid Injection (18AA) (38, 0.6 %), Compound Amino Acid Injection (18AA-II) (33, 0.5 %), et al. |
| Total | 5,564 (100.00) | Paclitaxel Injection (108, 1.9 %), Albumin-Bound Paclitaxel for Injection (98, 1.7 %), Sodium Aescinate Injection (84, 1.5 %), Ginkgo Diterpene Lactone Meglumine Injection (38, 0.6 %), Ginkgolide Injection (30, 0.5 %), et al. |
| Affected system | Clinical features | Frequency of ADRs |
|---|---|---|
| Cardiovascular | Blood pressure abnormalities, Palpitations | 629 |
| Neurological | Dizziness, Fatigue, Somnolence | 249 |
| Gastrointestinal | Nausea, Vomiting, Diarrhea | 1,091 |
| Respiratory | Dyspnea, Dry cough | 57 |
| Hematological | Bone marrow suppression, Leukopenia | 1,153 |
| Dermatological | Pruritus, Rash | 637 |
| Systemic reactions | Fever, Chills | 254 |
| Age, years | Recovery | Improvement | No improvement | Unknown | χ2 value | p-Value |
|---|---|---|---|---|---|---|
| ≤62 | 139 | 1,882 | 82 | 284 | 4.166 | 0.244 |
| >62 | 152 | 2,499 | 122 | 404 |
| ADR classification | Recovery | Improvement | No improvement | Unknown | χ2 value | p-Value |
|---|---|---|---|---|---|---|
| New/Serious ADRs | 197 | 1,976 | 122 | 402 | 100.767 | <0.001 |
| Non-Serious ADRs | 94 | 2,405 | 82 | 286 |
| Route of administration | Recovery | Improvement | No improvement | Unknown | χ2 value | p-Value |
|---|---|---|---|---|---|---|
| Intravenous infusion | 232 | 2,927 | 79 | 481 | 106.392 | <0.001 |
| Oral administration | 52 | 1,149 | 116 | 181 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmacovigilance and Adverse Drug Reactions · Patient Safety and Medication Errors · Pharmaceutical Practices and Patient Outcomes
Introduction
Adverse drug reactions (ADRs) represent a critical concern in the context of clinical medication safety. Data from the World Health Organization indicates that ADRs account for 3.7–6.5 % of hospital admissions, with an estimated 60 % of these cases considered preventable through effective risk management strategies [1]. The increasing utilization of antitumor targeted agents, biologics, and polypharmacy regimens has escalated the complexity of ADR profiles, posing significant challenges to patient safety and healthcare systems [2], 3]. Despite established national pharmacovigilance networks, significant gaps persist in the characterization of local and temporal ADR patterns within specific healthcare settings, particularly concerning high-risk medications and administration routes [4], 5]. A detailed analysis of longitudinal, hospital-based ADR data is crucial to identify institution-specific risk factors, evaluate the effectiveness of existing monitoring systems, and guide the development of targeted safety strategies [6], 7].
In the present study, 5,564 ADR cases reported between 2019 and 2024 at a tertiary care hospital were retrospectively analyzed to delineate local epidemiological patterns, identify key drug- and administration-related risk factors, and assess the evolution of reporting practices. This analysis aims to provide evidence to support enhanced surveillance, optimize clinical management protocols, and contribute to the broader pharmacovigilance knowledge base in the region.
Materials and methods
Data collection
A total of 5,564 valid ADR reports submitted between January 2019 and December 2024 were obtained from the National Adverse Drug Reaction Monitoring System. Duplicate reports were identified and removed based on patient identifier, drug name, reaction description, and report date. Incomplete reports lacking essential information (e.g., patient age, suspected drug, or ADR description) were excluded. Data cleaning involved standardizing drug names and ADR terminology according to the WHO Adverse Reaction Terminology.
Causality and severity assessment
Causality for each reported ADR was assessed by clinical pharmacists using the World Health Organization-Uppsala Monitoring Centre (WHO-UMC) criteria, categorized as certain, probable, possible, or unlikely. Only reports rated as ‘certain,’ ‘probable,’ or ‘possible’ were included. ADR severity was classified as ‘serious’ according to national guidelines if it resulted in death, was life-threatening, required hospitalization or prolongation of existing hospitalization, resulted in persistent or significant disability/incapacity, or caused a congenital anomaly/birth defect. ‘New’ ADRs referred to reactions not previously documented in the product labeling within China.
Statistical analysis
Descriptive statistics were used to analyze demographic and clinical characteristics. Categorical variables were compared using the Chi-squared (χ^2^) test. Associations between potential risk factors and ADR outcomes were examined through these bivariate analyses. A two-tailed p-value<0.05 was considered statistically significant.
Ethical approval
This retrospective study utilized anonymized adverse drug reaction data retrieved from the national reporting system and posed no risks to participants’ rights or health. As no direct patient intervention was involved and all data were de-identified, the requirement for informed consent was waived by the ethics committee. The study protocol was reviewed and approved by the Medical Ethics Committee of Jieshou People’s Hospital (Approval Number: [2025]0032). All procedures adhered to the principles outlined in the Declaration of Helsinki.
Results
Demographic and clinical characteristics of patients experiencing ADRs
The clinical characteristics of the 5,564 ADR cases are presented in Table 1. The mean patient age was 62.42 ± 16.58 years. Of the total cases, 2,920 (52.48 %) involved male patients and 2,644 (47.52 %) involved female patients. A history of prior ADRs was documented in 196 cases (3.52 %), while 196 cases (8.82 %) had no prior ADR history. In 4,877 cases (87.65 %), definitive ADR records were not available in their medical history. Specific medical histories or lifestyle risk factors were identified in 376 patients (6.78 %), while the remaining 5,188 cases (93.24 %) presented no such comorbidities or risk profiles.
Temporal distribution of ADRs
Analysis of ADR reports from 2019 to 2024 indicated a progressive increase in reporting frequency, with the highest number of cases recorded in 2023 (1,149 cases, 20.65 %). New or serious ADRs accounted for 48.47 % of all reports, with the largest proportion observed in 2024 (797 cases, 29.55 %). Non-serious ADRs comprised 51.53 % of cases, with peak occurrence documented in 2021 (807 cases, 28.15 %) (Table 2).
Age and sex distribution of patients experiencing ADRs
Demographic analysis of ADR cases indicated distinct age- and sex-related patterns. Most ADRs were reported among patients aged 60–79 years (2,813 cases, 50.55 %), with patients aged ≥60 years comprising 62.05 % of all cases. Male patients accounted for a higher proportion of ADR cases (2,920 cases, 52.48 %) compared with female patients (2,644 cases, 47.52 %), and this predominance was consistently observed across all age groups (Table 3).
Distribution of ADR reporting sources
The annual volume of ADR reports exhibited an overall upward trajectory, rising from 520 cases in 2019 to 1,149 cases in 2023, representing a 121 % increase, followed by a slight decrease to 1,079 cases in 2024. A substantial shift in reporting sources was noted during this period. In 2019, the majority of reports originated from nursing staff (97.12 %), while pharmacists contributed 1.73 %. By 2024, pharmacists represented the primary reporting source (93.05 %), followed by physicians (5.56 %) and nurses (1.39 %). This transition reflects the increasing role of pharmacists in ADR surveillance (Table 4).
Distribution of the top 10 administration routes associated with ADRs
Analysis of the main administration routes associated with ADRs indicated that intravenous infusion accounted for the highest proportion of ADRs (3,719 cases, 67.34 %), followed by oral administration (1,498 cases, 27.12 %). The incidence of ADRs associated with intravenous infusion was markedly higher compared with oral administration (Table 5).
Distribution of the top 10 dosage forms associated with ADRs
As illustrated in Figure 1, injectable formulations were most frequently implicated in ADRs (67.36 %) among the top 10 implicated dosage forms, significantly exceeding all other categories. This category was followed by tablets (21.21 %), lyophilized powders for injection (5.24 %), capsules (4.09 %), and transdermal patches (0.38 %). The remaining dosage forms accounted for progressively smaller proportions of reported ADRs, reflecting a descending pattern in ADR incidence across formulation types.
Distribution of top 10 dosage forms associated with ADRs.
Major drug categories associated with ADRs
A total of 626 distinct drug types were implicated in ADR occurrence. Antineoplastic agents accounted for the highest proportion (1,902 cases, 34.18 %), followed by anti-infective agents (598 cases, 10.75 %) and cardiovascular agents (524 cases, 9.42 %). Within these categories, platinum-based chemotherapeutics, cephalosporins, and thrombolytic agents were the most commonly reported subtypes associated with ADRs (Table 6).
Clinical features and frequency of ADRs
Hematologic adverse reactions constituted the most frequently reported ADR category, with bone marrow suppression and leukopenia as the predominant clinical manifestations. Gastrointestinal reactions, constituted the second most common category, typically presenting as nausea, vomiting, and diarrhea (Table7, Figure 2).
Radar map of clinical features of ADRs.
Impact of risk factors on ADRs outcomes
Age as a risk factor
A chi-squared (χ^2^) test was conducted to evaluate the association between age group (≤62 years vs. >62 years) and ADR outcomes. The statistical analysis indicated no significant association between age and ADR outcomes (χ^2^=4.66, p=0.244) (Table 8).
ADR type as a risk factor
The relationship between ADR classification (new/serious vs. non-serious) and clinical outcomes was examined using a χ^2^ test. A statistically significant difference was identified between ADR type and outcomes (χ^2^=100.767, p<0.001), indicating a significant association between ADR classification and clinical outcomes (Table 9).
Route of administration
A χ^2^ test was conducted to assess the association between the route of administration (intravenous infusion vs. oral) and ADR outcomes. Statistically significant differences were identified between the intravenous infusion and oral administration groups (χ^2^=106.392, p<0.001), indicating a strong association between administration routes and ADR outcomes (Table 10).
Discussion
Etiology and risk determinants of high ADR prevalence in older adult patients
Patients aged ≥60 years accounted for the majority of ADRs (62.05 %) in this cohort, a finding consistent with the high burden of age-related comorbidities (e.g., malignancies, chronic respiratory and cardiovascular diseases) in China, which necessitate the use of corresponding high-risk drug classes – antineoplastics, anti-infectives, and cardiovascular agents [8], [9], [10]. The elevated ADR susceptibility in this population is multifactorial, primarily driven by polypharmacy and multimorbidity (increasing the potential for drug-drug interactions) [11], 12], age-related pharmacokinetic decline (reduced hepatic/renal clearance leading to drug accumulation), and enhanced pharmacodynamic sensitivity to certain drug classes such as CNS agents and anticoagulants [13], 14].
Notably, multivariate analysis did not identify age as an independent predictor of serious ADR outcomes (p=0.244). This discrepancy between high incidence and non-significant outcome association may be attributed to more intensive monitoring and proactive management in geriatric care, or to limitations in outcome documentation. Thus, while age is a robust predictor of ADR occurrence, its role in determining outcome severity requires further prospective investigation.
Antineoplastic agents constituted the leading drug class (34.18 %), highlighting a critical pharmacovigilance challenge. Although novel targeted therapies often exhibit improved safety profiles, their rapid clinical adoption coupled with limited long-term real-world evidence can obscure risk recognition [15]. Mechanisms are subclass-specific: cytotoxic drugs like platinum-based agents carry narrow therapeutic indices and significant organ toxicity risks (e.g., nephrotoxicity) [16], with carboplatin being the most frequently implicated single agent in this study. Targeted therapies, such as EGFR inhibitors, are associated with mechanism-based toxicities like cutaneous reactions [17], 18].
Anti-infectives (10.75 %) and cardiovascular drugs (9.42 %) remained prominent contributors. Persistent ADR incidence from anti-infectives, despite antimicrobial stewardship efforts, suggests ongoing broad-spectrum usage patterns [19], manifesting as β-lactam hypersensitivity or fluoroquinolone-associated neurotoxicity [20]. ADRs from cardiovascular drugs, such as warfarin-related bleeding, underscore the challenges of monitoring in an aging population.
Risk amplification effect of the intravenous administration route
Intravenous infusion accounted for 67.34 % of ADR cases in this study, with elevated risk attributable to three principal mechanisms [21], 22]. First, bypassing the first-pass effect contributes to heightened systemic drug exposure and increased susceptibility to concentration-dependent toxicities. Second, excipient-mediated reactions may occur, as immediate exposure to formulation adjuvants such as polysorbate 80 can precipitate anaphylactoid responses. Third, infusion rate–related toxicity is observed when administration kinetics are not properly controlled; for example, rapid vancomycin infusion can induce red man syndrome.
Statistically significant differences in ADR outcomes were identified between intravenous and oral administration routes (p<0.001), consistent with pharmacovigilance findings reported by DeFrancesco et al. [23]. However, the observed ADR incidence associated with oral administration (27.12 %) may represent an underestimation. This underestimation is likely influenced by delayed or latent symptom onset due to gastrointestinal absorption kinetics, as well as reporting bias, resulting from patients voluntarily discontinuing medication.
Evolution and improvement of the ADR monitoring system
A consistent year-on-year increase in ADR reporting volume was observed from 2019 to 2024. Pharmacists became the primary reporting source during this period, with reporting shifting from nurses (21.03 %) to pharmacists (71.22 %). This transition reflects the growing maturity of the global pharmacovigilance network rather than a direct indication of deteriorating medication safety. Such trends contribute to earlier risk identification, optimization of medication regimens, and improvements in public health outcomes.
Future directions for ADR surveillance are expected to emphasize proactive early warning systems and precision prevention strategies, supported by RWE and AI–based predictive models [24], 25]. The key role of pharmacists represents a paradigm shift in hospital pharmacy services, characterized by several key improvements:
- (1)Enhanced multidisciplinary collaboration: Clinical pharmacists apply therapeutic drug monitoring (TDM) and pharmacogenomic (PGx) analysis to improve ADR prediction in patients receiving complex treatment regimens.
- (2)Integrated “Pharmacist–electronic heath record” systems: The use of electronic medical record triggers (e.g., abnormal liver enzyme levels [ALT>3 × ULN], Stevens–Johnson syndrome diagnostic codes) enables real-time ADR detection and targeted pharmaceutical care [26].
- (3)Precision medication safety mechanisms: Individualized prevention strategies are implemented in high-risk therapeutic areas, strengthening proactive pharmacovigilance and patient safety.
Directions for improving clinical practice
Based on the study findings, a three-pronged intervention strategy was proposed:
- (1)Pre-risk control: Establishment of pharmacogenetic testing systems for antineoplastic agents to guide dose adjustments in patients with gene polymorphisms.
- (2)Intra-risk intervention: Implementation of a “dual verification” protocol for intravenous administration, including assessment of infusion rate appropriateness during prescription review and vehicle compatibility testing during drug preparation.
- (3)Post-risk management: Development of an ADR prediction model tailored for older adult patients, integrating parameters such as creatinine clearance, serum albumin, and polypharmacy for risk assessment. Additional measures include stepwise dosing strategies, preferential use of oral formulations when clinically appropriate, and standardized infusion protocols for essential intravenous therapies [27], [28], [29].
Study limitations
This study has limitations. Its retrospective, single-center design may affect generalizability and introduces potential selection bias. Reliance on spontaneous reporting is susceptible to under-reporting and reporting bias, particularly for non-serious or oral drug-related ADRs. Although causality was assessed and multivariate adjustment performed, unmeasured confounders (e.g., precise dosing, detailed comorbidities) may persist. Furthermore, the study period encompasses the COVID-19 pandemic, which may have influenced drug utilization and reporting behaviors in unanalyzed ways. Future studies should strengthen risk management protocols for biologics and novel antineoplastic agents to address emerging ADR patterns [30].
Conclusions
This retrospective study confirms that antineoplastic agents and intravenous administration are independently associated with a higher risk of serious ADRs in a tertiary care setting. The evolving role of pharmacists as key contributors to the reporting system is a positive development for institutional pharmacovigilance. These findings advocate for targeted strategies, including intensified monitoring of high-risk drug classes, optimization of intravenous administration protocols, and the continued integration of clinical pharmacists into medication safety teams to mitigate ADR risks.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Walker LE Pirmohamed M Increasing trend in hospitalisation due to adverse drug reactions: can we stem the tide?Drug Therapeut Bull 202361879110.1136/dtb.2022.00005037193588 · doi ↗ · pubmed ↗
- 2Strobach D Pudritz Y Huttner D Retrospective analysis of adverse drug reaction enquiries to a hospital drug information service: lessons to be learned to increase in-hospital drug safety Int J Pharm Pract 2024323849110.1093/ijpp/riae 03639024519 · doi ↗ · pubmed ↗
- 3Kose E Nakagawa S Niki K Hashizume J Kawazoe T Suzuki N Pharmacist interventions for adverse drug reactions in palliative care: a multicentre pilot study Pharmazie 202378141910.1691/ph.2023.355437592417 · doi ↗ · pubmed ↗
- 4Cacabelos R Naidoo V Corzo L Cacabelos N Carril JC Genophenotypic factors and pharmacogenomics in adverse drug reactions Int J Mol Sci 2021221330210.3390/ijms 22241330234948113 PMC 8704264 · doi ↗ · pubmed ↗
- 5Malki MA Pearson ER Drug-drug-gene interactions and adverse drug reactions Pharmacogenomics J 2020203556610.1038/s 41397-019-0122-031792369 PMC 7253354 · doi ↗ · pubmed ↗
- 6Aziz T Shabbir MA Sarwar A Khan AA Zhao L Yang Z Exploring the multifaceted probiotic potential of Lactiplantibacillus plantarum NMGL 2, investigating its antimicrobial resistance profiles and bacteriocin production J Microbiol Methods 202523610717810.1016/j.mimet.2025.10717840543402 · doi ↗ · pubmed ↗
- 7Aziz T Naveed M Shabbir MA Sarwar A Khan AA Hasnain A Whole genome analysis of Tibetan kefir-derived Lactiplantibacillus plantarum 12-3 elucidates its genomic architecture, antimicrobial and drug resistance, potential probiotic functionality and safety Front Biosci (Landmark Ed)20242914710.31083/j.fbl 290414738682181 · doi ↗ · pubmed ↗
- 8Zazzara MB Palmer K Vetrano DL CarfìA Onder G Adverse drug reactions in older adults: a narrative review of the literature Eur Geriatr Med 2021124637310.1007/s 41999-021-00481-933738772 PMC 8149349 · doi ↗ · pubmed ↗