Beyond direct-acting antiviral therapy: Characterizing mental health conditions and depressive symptoms among patients recently treated for hepatitis C
Sarah E. Kelly, Adedayo Ajidahun, Shannon Bytelaar, Erin Ding, Christina Fulton, Marianne Harris, Grace Sykes, Jessica Ly, Rolando Barrios, Mark W. Hull, Julio S. G. Montaner, Kate Salters

TL;DR
This study finds that many hepatitis C patients recently treated with DAAs also have mental health issues, suggesting a need for integrated mental health care.
Contribution
The study highlights the high prevalence of undiagnosed depressive symptoms and psychiatric disorders among HCV patients post-treatment.
Findings
48% of participants had significant depressive symptoms.
55% reported a history of psychiatric disorders.
Depressive symptoms were linked to recent healthcare barriers.
Abstract
The uptake of hepatitis C virus (HCV) treatment, including among under-served populations, has improved significantly in the Direct Acting Antiviral (DAA) era. However, it is unclear whether patients undergoing HCV treatment are receiving adequate support to engage in healthcare for other concurrent conditions. We sought to characterize psychiatric disorders and depressive symptomatology among a cohort of patients recently treated for HCV. We conducted a secondary analysis using data from the Preservation of Sustained Virologic Response (Per-SVR) study, a prospective cohort of individuals who achieved sustained virologic response (SVR) following DAA treatment in British Columbia, Canada. After confirming SVR through receipt of an undetectable HCV viral load test within three months post-treatment, participants were enrolled in the study and completed interviewer-administered surveys.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
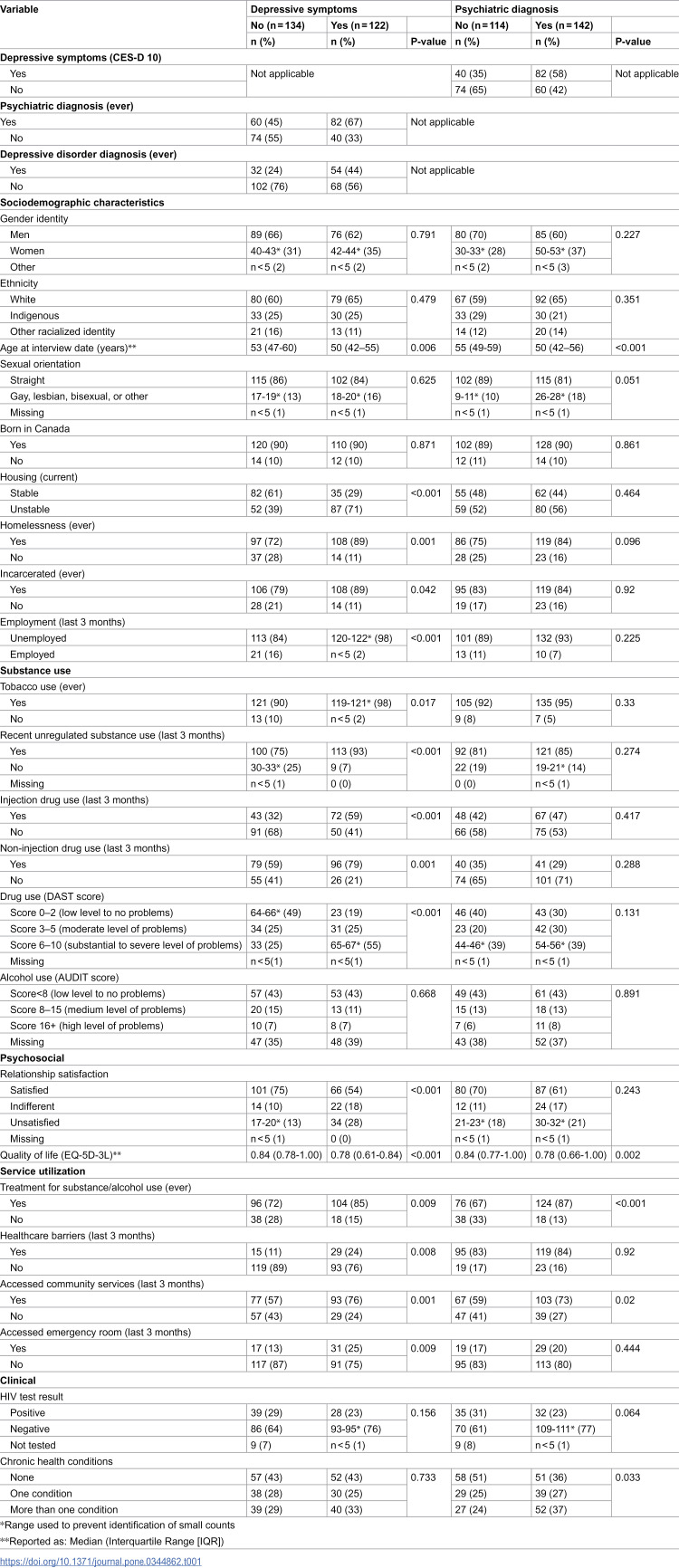 Figure 1
Figure 1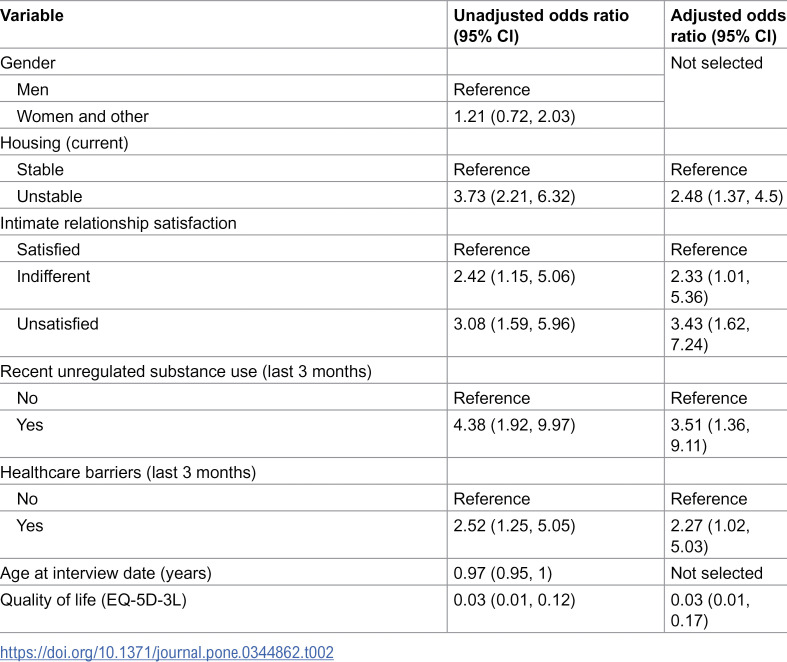 Figure 2
Figure 2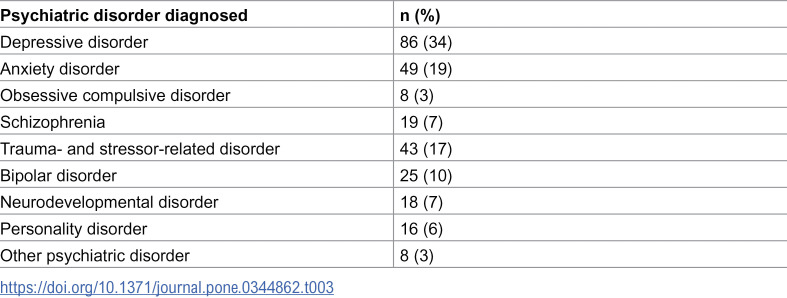 Figure 3
Figure 3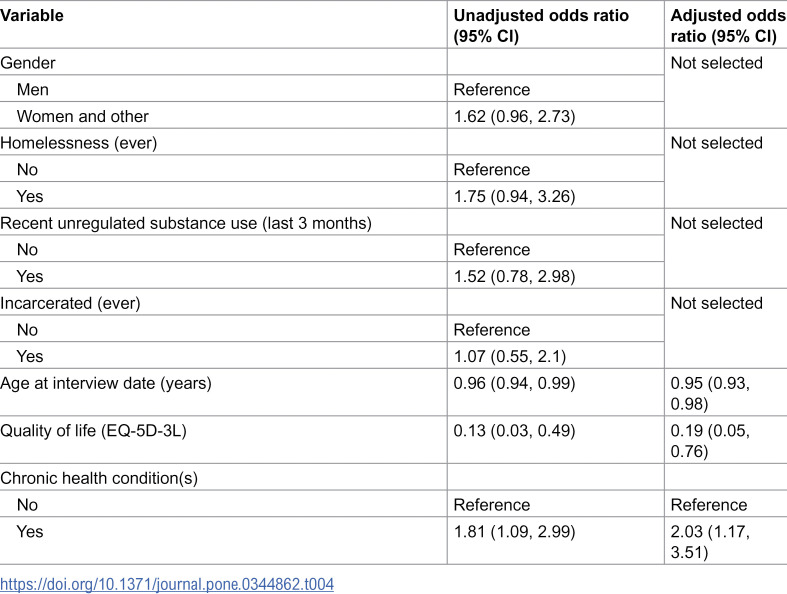 Figure 4
Figure 4- —http://dx.doi.org/10.13039/501100004726Ministry of Health, British Columbia
- —http://dx.doi.org/10.13039/501100015631Merck Canada
- —http://dx.doi.org/10.13039/501100005247University of British Columbia
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis C virus research · Diabetes Management and Education · Cardiac Health and Mental Health
Introduction
Hepatitis C virus (HCV) is a bloodborne viral infection causing inflammation of the liver [1]. Left untreated, HCV can cause severe liver damage, cancer, and even death [1]. In Canada, HCV causes more years of life lost due to premature death and disability than any other communicable disease [2]. Communities that face structural marginalization, such as people who inject drugs (PWID), incarcerated individuals, and Indigenous Peoples, continue to be disproportionately affected by HCV [3, 4]. These communities, known as priority populations, are more likely to engage in behaviours that elevate the risk of HCV due to intersecting factors such as systemic racism, poverty, and built environment [5, 6]. These same populations most vulnerable to HCV are also disproportionately affected by other health issues, particularly psychiatric disorders [7–9].
HCV is curable, with over 95% of patients achieving sustained virologic response (SVR) through the administration of direct-acting antivirals (DAAs) [1]. However, PWID and other priority populations face numerous obstacles to accessing HCV treatment, including stigma and gaps in continuity of care [10]. Despite these barriers, increasing rates of treatment uptake and SVR achievement have been observed among priority populations in the DAA era [11–13]. Nonetheless, rising rates of HCV treatment among under-reached populations do not necessarily indicate that care for comorbid conditions is also being provided, and HCV reinfection remains a concern.
There is evidence that HCV-affected populations experience a high burden of psychiatric comorbidity [14–18]. This has significant implications for HCV elimination targets, as untreated mental health may elevate the risk of HCV reinfection [19, 20]. Emerging evidence suggests that integrating HCV treatment with mental health counselling may reduce reinfection risk, although more research is needed [19,20]. Without additional care and support for comorbid psychiatric conditions, these individuals remain vulnerable to HCV reinfection post-treatment.
While HCV treatment has become increasingly available in Canada, it remains unclear whether patients undergoing treatment are receiving adequate support to engage in care for concurrent conditions. Coordinated post-treatment care for people living with concurrent psychiatric conditions is essential to reduce rising reinfection rates and improve overall health outcomes [19, 20]. Characterizing psychiatric comorbidities among HCV-affected populations is critical to determine the current threshold of psychiatric care delivery and to inform an integrated approach to care. With these implications in mind, this study aims to describe and assess psychiatric diagnoses and depressive symptoms among a cohort of patients recently treated for HCV.
Methods
Study design, recruitment, and data collection
This paper is a secondary analysis of data collected from the Preservation of Sustained Virologic Response (Per-SVR) study baseline survey. The Per-SVR study is a prospective observational cohort study based in British Columbia (BC), Canada. The research objectives of the Per-SVR study were to understand HCV reinfection patterns, to determine the threshold of risk behaviour that is protective against HCV reinfection, and to evaluate the impact of HCV treatment on healthcare costs and service utilization. Between April 2017 and December 2024, individuals having successfully been treated for HCV using DAAs in BC within the previous three months were recruited into the Per-SVR study. Potential participants were recruited through hospitals, clinics, pharmacies, community organizations, supervised consumption sites, and through community outreach efforts, such as study posters. Individuals were eligible to participate in the study if they had an undetectable HCV plasma viral load post-DAA treatment (i.e., achieved SVR), provided that this treatment was completed less than 12 weeks prior to the first study visit. Prior to enrolment in the study, undetectable viral load was confirmed through laboratory data. Physician enrolment forms were used to confirm the date of DAA treatment completion and other treatment information such as course of treatment and medication dispensed. Participants were required to be 19 years of age or older, to be able to communicate in English, and to reside in BC.
The Per-SVR study protocol and informed consent form have been approved by the University of British Columbia–Providence Health Care Research Ethics Board (H16-00225). The approved informed consent form contains a section reserved for the documentation of oral consent. Written consent was obtained for the majority of participants. Oral consent was obtained over the phone for participants who did not live within reasonable proximity to any of the study locations. After providing informed consent, potential participants completed a screening visit to assess study eligibility and received a cash honorarium (40 CAD) upon the completion of each study visit. As we were still in the data collection phase at the time of this analysis, only baseline data was used.
Questionnaires were administered as one-on-one interviews either in-person at various study locations (i.e., specialty clinics, community clinics, hospitals, etc.) or over the phone. Interview questions collected quantitative sociodemographic, behavioural, psychosocial, clinical, and service utilization data. This questionnaire was developed for use in the Per-SVR study. Not all questions were relevant for the purposes of this analysis. As such, not all questions were included.
Study sample and sample characteristics
This analysis includes baseline data from all Per-SVR study participants who completed a baseline study visit between April 1^st^, 2017 and August 1^st^, 2023.
Outcome measures of interest
The primary outcome measure was self-reported lifetime diagnostic history of psychiatric disorders at baseline. Psychiatric disorders were defined using the Diagnostic and Statistical Manual of Mental Disorders (5^th^ ed.; DSM-5) diagnostic criteria [21]. Psychiatric disorders included depressive disorder, anxiety disorder, obsessive-compulsive disorder (OCD), schizophrenia, trauma- and stressor-related disorders, bipolar disorder, neurodevelopmental disorders, personality disorders, and other psychiatric disorders [21]. After hearing a list of common disorders, participants were asked to name any psychiatric disorders that they could recall being clinically diagnosed with, including disorders outside of those listed. Psychiatric diagnoses were not verified through medical records.
The secondary outcome measure was depressive symptomatology. Depressive symptoms were identified using the validated 10-item Center for Epidemiologic Studies-Depression (CES-D 10) scale [22]. This tool has been validated among a population of people living with HIV in BC with a high proportion of PWID and other marginalized groups [22]. This scale assesses acute depressive symptoms within the previous week. A CES-D 10 score of 10 or above was considered indicative of significant depressive symptoms, while a CES-D 10 score below 10 was considered to indicate absence of significant depressive symptoms [22]. Thus, participants with scores ≥10 were considered to have depressive symptoms and participants with scores <10 were considered not to have depressive symptoms. Scores were calculated post-interview.
Explanatory variables
The explanatory variables of interest included self-reported baseline sociodemographic characteristics, alcohol- and substance use-related behaviours, psychosocial factors, service utilization information, and clinical data. Sociodemographic characteristics included age (median); ethnicity (white, Indigenous, other racialized identity); gender identity (men, women, other); sexual orientation (straight, gay, lesbian, bisexual, other); birthplace (Canada, other); housing (stable, unstable); and employment (employed, unemployed). Although the original questionnaire allowed for a larger variety of responses, these variables were collapsed to ensure sufficient power for analyses. The Alcohol Use Disorders Identification Test (AUDIT) screening tool and the Drug Abuse Screening Test (DAST) screening tool were used to measure alcohol use-related problems, substance use-related problems, and other variables [23]. Psychosocial factors included quality of life and relationship satisfaction. Quality of life scores were derived from the European Quality of Life 5 Dimensions 3 Level Version (EQ-5D-3L) descriptive system [24]. A scoring algorithm specific to the Canadian context was used to calculate a standardized score measuring the respondent’s quality of life in relation to their health status [25]. Service utilization variables included healthcare barriers as well as the use of harm reduction services, health services, and other services. Healthcare barriers included poor treatment by healthcare professionals, long waitlists, limited hours, discrimination, difficulty keeping appointments, no attachment to primary care, and other barriers. Clinical data included lifetime diagnostic history of chronic diseases or chronic health conditions as well as human immunodeficiency virus (HIV) serologic status. Chronic health conditions included heart and vascular conditions such as high cholesterol and coronary artery disease; endocrine-related conditions such as diabetes; respiratory conditions such as asthma and chronic bronchitis; digestive conditions such as stomach ulcers; musculoskeletal conditions such as arthritis; cancer; and other chronic conditions such as chronic liver disease, blood disorders, or chronic pain.
Statistical analysis
Descriptive statistics were used to characterize the dataset. Factors associated with depressive symptoms and psychiatric diagnoses were assessed in bivariable analyses. Chi-square test or Fisher’s exact test were used for categorical variables, and Wilcoxon’s rank sum test was used for continuous variables. Logistic regression was used to assess both the probability of having depressive symptoms at baseline and the probability of receiving any previous psychiatric diagnosis. Unadjusted odds ratio (OR) and 95% confidence interval (CI) were calculated for each variable. Variables were selected for the logistic regression model a priori, and were included regardless of statistical significance in bivariable analyses. We included demographic characteristics, potential confounders, and other covariates, which were selected based on previous literature. Conceptually overlapping variables were evaluated (e.g., housing and homelessness), and only one variable from such groupings was retained. Models were performed on the complete dataset. The final multivariable model was selected using a modified backward model selection method, which is based on Akaike information criterion (AIC) and Type III p-value, with the least significant variable dropped until the final model had the optimum (minimum) AIC [26]. Adjusted odds ratio (AOR) and 95% CI were reported for the selected variables. The overall alpha level for statistical significance was set at 0.05. SAS version 9.4 (SAS, North Carolina, United States) was used for all analyses.
Results
Descriptive characteristics
Between April 1^st^, 2017 and August 1^st^, 2023, 272 eligible participants completed a baseline study interview. After excluding 16 participants due to incomplete data, such as no available CES-D 10 score, 256 participants were included in the analytic sample. The majority (n = 159, 62%) of participants were white and 165 (64%) self-identified as men. The median age at baseline was 51 years (interquartile range [IQR]: 44–58; range 22–85 years). Healthcare barriers, including poor treatment by healthcare professionals, long waitlists, and other barriers, were experienced by 44 (17%) participants. Additional baseline sociodemographic, psychosocial, clinical, and behavioural characteristics are summarized in S1 Table.
Depressive symptoms and psychiatric conditions
The prevalence of psychiatric disorders and depressive symptoms are reported in Table 1. Almost half (n = 122, 48%) of participants had acute depressive symptoms as identified through the CES-D 10 scale. Of those with depressive symptoms, only 44% had ever been diagnosed with depressive disorder. Of the 256 participants included in the study, four were excluded from the logistic regression analyses (n = 252) due to missing values for one or more of the included variables. Participants with depressive symptoms were significantly more likely to report recent unregulated substance use (AOR: 3.51; 95% CI: 1.36, 9.11), intimate relationship dissatisfaction (AOR: 3.43; 95% CI: 1.62, 7.24), unstable housing (AOR: 2.48; 95% CI: 1.37, 4.5), and healthcare barriers (AOR: 2.27; 95% CI: 1.02, 5.03) (Table 2). After conducting model selection, gender and age were not selected for the final multivariable model.
Table 1: Factors associated with depressive symptoms and psychiatric diagnosis (chi-square test).
Table 2: Factors associated with depressive symptoms (logistic regression analysis).
Psychiatric diagnosis was reported by 55% (n = 142) of study participants, the most frequent being depressive disorder (34%), anxiety disorder (19%), and trauma- and stressor-related disorder (17%) (Table 3). Psychiatric disorders listed are not mutually exclusive. Participants with a psychiatric diagnosis were significantly less likely to report a high quality of life (AOR: 0.19 [per unit increase]; 95% CI: 0.05, 0.76) and were significantly more likely to be diagnosed with at least one chronic health condition (AOR: 2.03; 95% CI: 1.17, 3.51) (Table 4). After conducting model selection, gender, history of homelessness, history of incarceration, and unregulated substance use were not selected for the final multivariable model.
Table 3: Prevalence of lifetime self-reported psychiatric diagnoses (n = 256).
Table 4: Factors associated with psychiatric disorders (logistic regression analysis).
Discussion
This study describes and assesses depressive symptoms and psychiatric disorders among a cohort of patients recently treated for HCV. We found a high burden of psychiatric conditions among our cohort, which is supported by previous literature [14–18]. However, our study is among few to evaluate depressive symptomatology among HCV-affected populations. We observed depressive symptoms among almost half of our cohort, and those with depressive symptoms were almost three times as likely to report having recently faced healthcare barriers. Less than half of those with depressive symptoms reported ever being diagnosed with depression. These results showcase that there is room to address an underlying need for mental health support among HCV-affected populations.
Consistent with other Canadian literature, we observed a high proportion of PWID, people with a history of IDU, previously incarcerated individuals, and Indigenous Peoples in our HCV-affected cohort [4, 27]. These priority populations face stigma and other barriers to HCV treatment [10]. In addition, untreated psychiatric comorbidities have been associated with loss to follow up during the HCV care cascade, thus inhibiting treatment completion [28]. Almost half our participants were experiencing depressive symptoms at baseline and over half had been previously diagnosed with a psychiatric disorder, yet they were able to successfully complete HCV treatment and achieve SVR. This is an important consideration that supports evidence of increased DAA treatment uptake among priority populations in BC [12]. While the successful completion of HCV treatment among our cohort despite high levels of psychiatric comorbidity is encouraging, it may also highlight an underlying gap in mental health care. Addressing this unmet need is vital for recently treated individuals who are vulnerable to reinfection, as there is evidence to support that receiving mental health care reduces the risk of HCV reinfection [19, 20]. The time when an individual is accessing HCV care could serve as a unique window of opportunity to engage priority populations in the screening and assessment of psychiatric conditions.
Among our cohort, 17% of participants reported recently experiencing barriers to healthcare, including discrimination and poor treatment by healthcare professionals. Although we found no significant association between psychiatric disorders and healthcare barriers, those with depressive symptoms were more than twice as likely to report having recently faced healthcare barriers. This may be because accessing healthcare services can be particularly challenging for individuals with depressive symptoms. Those with depressive symptoms in our cohort were also more than three times as likely to report recent unregulated substance use. This is important, as depression can further impede access to healthcare among stigmatized populations such as people who use unregulated substances [29]. We observed that 48% of our cohort had depressive symptoms, similar to an Australian cohort of HCV patients with a history of IDU, where 47% had moderate to severe depressive symptoms [17]. Such similar findings despite different settings suggests that disproportionately high rates of depressive symptoms among HCV-affected populations may be widespread.
In addition to the high prevalence of depressive symptoms and psychiatric disorders, 57% of participants reported having been previously diagnosed with at least one chronic health condition, and nearly a third experienced multimorbidity. These findings support existing evidence of elevated medical comorbidity and multimorbidity among HCV-affected populations [7–9]. Importantly, individuals in our cohort with a psychiatric diagnosis were more than twice as likely to have been diagnosed with at least one chronic health condition. This could be because those with chronic health conditions must access care more frequently, and thus were able to access screening for psychiatric conditions through their established connection to the health care system. In a population with high comorbidity and multimorbidity, taking a person-centered approach to HCV care is warranted.
Less than half (44%) of those with depressive symptoms reported ever being diagnosed with depression, suggesting a significant gap in access to screening for psychiatric illness. Targeted interventions to improve screening and care for specific health conditions have been successful for populations with comparable attributes [30, 31]. Psychosocial interventions targeting depression, anxiety, and quality of life have successfully improved mental health outcomes among people living with HIV, especially among those with depressive symptoms [30]. There is evidence demonstrating that integrating psychiatric care with HIV care reduces stigma, increases engagement in care, and improves the diagnosis and treatment of psychiatric conditions, including depression [31]. Taking a similar person-centered approach throughout the HCV care cascade could improve health outcomes for HCV-affected populations. Moreover, integrating HCV care into community mental health settings has been shown to increase access to HCV screening, as well as access and adherence to HCV care among people with severe mental illness [32, 33]. This underscores the opportunity to implement a syndemic approach, integrating routine mental health screening and treatment alongside HCV care. This strategy could streamline the diagnosis and management of depression and other psychiatric conditions among HCV-affected populations.
Our study had several limitations. First, we relied on self-reported data for our outcome measures of interest and the majority of our covariates. Self-reported data may have been affected by recall bias and/or social desirability bias, as well as the individual’s interpretation of survey questions. Stigma may also have impacted participants’ willingness to disclose psychiatric diagnoses. Moreover, it is possible that the reported psychiatric diagnoses occurred long before participants’ engagement in the survey, as we were not able to identify the current status of these diagnoses. Due to the cross-sectional nature of this analysis, we cannot establish causation. Additionally, despite recruiting participants from a variety of locations, many recruitment sites primarily served populations with a high incidence of substance use disorders, housing insecurity, and social inequity. Thus, it is possible that marginalized groups are overrepresented in our cohort, however, HCV has been found to be more prevalent among these priority populations in Canada [4, 27]. Finally, the nature of the study requires participants to be able to actively engage in answering survey questions, so we may not be capturing people with more severe mental illness.
Conclusion
We observed a high burden of depressive symptomatology and self-reported psychiatric conditions in a cohort of people recently treated for HCV, which may highlight an underlying gap in mental health care. Those with depressive symptoms were significantly more likely to experience healthcare barriers and the majority had never been diagnosed with depression, underscoring the urgent need for mental health support. Integrating routine mental health screening and treatment with HCV care could streamline the diagnosis and management of depression and other psychiatric conditions. Standardized provision of psychiatric care alongside HCV treatment may improve access to care, reduce HCV reinfection risk, and improve overall health outcomes among HCV-affected populations. Further research should explore the implementation of widely accessible, culturally safe, low barrier mental health care that can feasibly be administered alongside HCV treatment.
Supporting information
S1 TableBaseline profile of the cohort (n = 256).(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization [Internet]. Hepatitis C; [updated 2025 Jul 25; cited 2023 Aug 18]. Available from: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c
- 2Lourenço L, Kelly M, Tarasuk J, Stairs K, Bryson M, Popovic N. The hepatitis C epidemic in Canada: an overview of recent trends in surveillance, injection drug use, harm reduction and treatment. Can Commun Dis Rep. 2021;47(12):561–70.35692566 10.14745/ccdr.v 47i 12a 01PMC 9126177 · doi ↗ · pubmed ↗
- 3Mandel E, Underwood K, Masterman C, Kozak RA, Dale CH, Hassall M, et al. Province-to-province variability in hepatitis C testing, care, and treatment across Canada. Can Liver J. 2023;6(2):234–48. doi: 10.3138/canlivj-2022-0029 37503520 PMC 10370727 · doi ↗ · pubmed ↗
- 4Krajden M, Cook D, Janjua NZ. Contextualizing Canada’s hepatitis C virus epidemic. Can Liver J. 2018;1(4):218–30.35992621 10.3138/canlivj.2018-0011 PMC 9202764 · doi ↗ · pubmed ↗
- 5The Canadian Network on Hepatitis C [Internet]. Blueprint to inform hepatitis C elimination efforts in Canada; 2019 May [cited 2023 Nov 21]. Available from: https://cdn.ca.yapla.com/company/CP Yfg PV 3Cn IU Jxh G Ew Bsuytv M/asset/files/blueprint/blueprint_hcv_2019_05.pdf. 2019. 2023 November 21.
- 6Pan-Canadian Health Inequalities Reporting Initiative [Internet]. Key Health Inequalities in Canada: A National Portrait; 2018 May 28 [cited 2023 Nov 21]. Available from: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/science-research/key-health-inequalities-canada-national-portrait-executive-summary/key_health_inequalities_full_report-eng.pdf
- 7Louie KS, St Laurent S, Forssen UM, Mundy LM, Pimenta JM. The high comorbidity burden of the hepatitis C virus infected population in the United States. BMC Infect Dis. 2012;12:86. doi: 10.1186/1471-2334-12-86 22494445 PMC 3342214 · doi ↗ · pubmed ↗
- 8Cooper CL, Galanakis C, Donelle J, Kwong J, Boyd R, Boucher L, et al. HCV-infected individuals have higher prevalence of comorbidity and multimorbidity: a retrospective cohort study. BMC Infect Dis. 2019;19(1):712. doi: 10.1186/s 12879-019-4315-6 31438873 PMC 6706878 · doi ↗ · pubmed ↗