Implementing Transitional Care Interventions for Surgical Patients: A Scoping Review
G. Tobiano, B. M. Gillespie, K. Turner, A. M. Eskes, B. Patel, J. Colquhoun, L. Ferronato, W. Chaboyer

TL;DR
This scoping review summarizes strategies used to implement transitional care for adult surgical patients, highlighting common and underused methods.
Contribution
The study identifies frequently used and underutilized implementation strategies for surgical transitional care interventions.
Findings
Staff education, staffing changes, and electronic system updates were commonly used strategies.
Colorectal and cardiac surgery patients in Asia and the U.S. were most frequently studied.
Capacity-building and scale-up strategies were less commonly implemented.
Abstract
To synthesise the evidence on implementation strategies used to implement transitional care interventions for adult surgical patients. Scoping review. Medline, CINAHL and EMBASE were searched in August 2023 and updated June 2025, followed by citation searches. Studies were screened independently by two researchers, and one extracted data, another verified its accuracy. Studies about transitional care interventions for adult surgical patients were coded according to the ‘Five classes of implementation strategies’ and the ‘Patterns, Advances, Gaps, Evidence for practice and Research recommendations’ framework, to illuminate the review findings. Based on 27 studies included in the scoping review, staff education, changes to staffing and electronic systems, and change management techniques were frequently used implementation strategies. Implementation strategies were mostly used with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
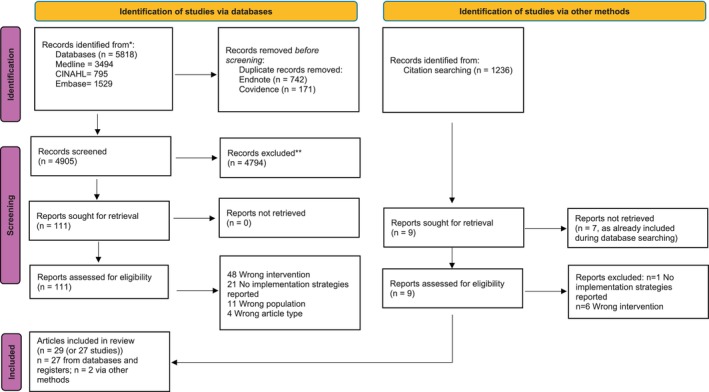 FIGURE 1
FIGURE 1| Target audience | Person responsible (who enacted the strategy) | Strategy | # studies that used the strategy (# studies that mentioned person responsible) | References |
|---|---|---|---|---|
|
| ||||
| Nurses, nurse managers, enterostomists, pharmacists, social workers, physicians, doctor kidney transplant surgeons, attending physicians, kidney transplant specialist nurses, transitional nursing staff | Not reported | Staff education and training to support the intervention delivery | 11 (0) | (Hu et al. |
| Nurse, orthopaedic case manager, person conducting follow‐up telephone calls, stakeholders, colorectal surgical department | Implementation team: Chief nurse, unit director, project leader, nurses, nursing manager, orthopaedic case manager | Staff education about the intervention | 5 (3) | (Hu et al. |
| Patient | Nurse | Patient education about the intervention (not as an intervention component) | 4 (1) | (Robertson et al. |
|
| ||||
| Frontline, supervisory, leadership staff | Nurses, pharmacists, social workers, physicians, research team, nurse health education team | Monitor process/outcomes | 9 (5) | (Hu et al. |
| Not reported | Cardiac service team, project administrator, patients, nurses, surgeons, interdisciplinary lung transplant team, surgical staff | Assess context | 6 (5) | (Du |
| Not reported | Intervention team | Select change management approach | 5 (1) | (Xu |
| Not reported | Physicians, inpatient and outpatient nursing staff, case managers, pharmacists, hospital administrators, clinical leaders, surgeons, frontline staff, supervisory staff, ‘providers’, patients, caregivers, nutritionists, psychological consultants, ostomy specialists, care administrators | Stakeholder engagement (in implementation process, not intervention development) | 5 (5) | (Li et al. |
| Not reported | Chief nurse | Determine project goals and measures of success | 2 (1) | (Fisher et al. |
|
| ||||
| Associate chief nurse, attending physician, charge nurse, nurses, lead nurses, transitional care nurses, pharmacists, outpatient nurses and clinical staff, case managers, multi‐disciplinary team, kidney transplant surgeons, kidney transplant specialist nurses, medical assistant, project administrator, care navigator, nonclinical professional | Chief nurse, unit director, hospital administrators | Staffing changes and role clarification | 11 (2) | (Li et al. |
| Follow‐up specialists, researcher | Not reported | Changes to electronic systems | 7 (2) | (Li et al. |
| Nurse, caregivers | Researcher | Prompting | 3 (1) | (Hu et al. |
| Not reported | Surgeon, nursing administrator, specific member of the surgery ward staff, e.g., dedicated wound/ostomy and surgical floor nurses | Champion | 2 (2) | (Du |
| Not reported | Hospital administrators | Financial resources | 3 (1) | (Fisher et al. |
| Catheterisation laboratory nursing and ancillary staff, Advanced practice provider | Not reported | Physical resources | 2 (0) | (Aicher et al. |
| Patients | Outpatient departments | Change routines and schedules | 1 (1) | (Grahn et al. |
| Not reported | Not reported | Guidelines and policies | 1 (0) | (Coskun and Duygulu |
|
| ||||
| Not reported | Project leader, project administrator, medical coordinated‐transitional care originator, coordinated‐transitional care clinical leaders, champion | Project leader to direct implementation process | 3 (3) | (Fisher et al. |
| Not reported | Program managers, chief physician, ostomy therapist/specialists, nurses, physician, care administrator | Ensure implementation staff adequately trained or possess the necessary expertise | 3 (3) | (Zhang et al. |
|
| ||||
| Patients | Not reported | State‐wide or nation‐wide program | 2 (0) | (Zhou et al. |
| Other institutions | Not reported | Prepare for dissemination to other institutions | 1 (0) | (Fisher et al. |
| Patterns | Advances | Gaps | Evidence for practice | Research recommendations |
|---|---|---|---|---|
| Implementation strategies for surgical TCIs are targeted at the delivery system (i.e., those individuals, teams and systems that must adopt the intervention into practice). | There is growing evidence that implementation strategies needed to support surgical TCI implementation include:
Providing adequate staffing. Developing or changing electronic systems. Educating multi‐disciplinary clinicians to deliver the intervention. Using change management processes. | Few implementation strategies were targeted at the support system (i.e., those individuals, teams and systems that build capacity to adopt the intervention):
In a few instances a project leader was hired to manage the change process; their skills/training was rarely reported. Few interventions were scaled up; often surgical TCIs are context specific, approaches to transferring TCIs to other settings was unclear in this review. Although two studies reported increased financial resources provided for surgical TCIs, the financial viability of strategies such as staffing and electronic system changes is unclear. Implementation fidelity and intervention fidelity were underreported. |
Hospital leader support is critical to implementing surgical TCIs; they must provide resources such as staffing, including up‐skilled staff to manage the change management process and have adequate IT departments to make changes to electronic systems. Staff member/s responsible for implementing the surgical TCI could use strategies outlined in this review. For example, they could provide specific education to multi‐disciplinary teams and use change management processes. |
Consider using strategies outlined in this review when implementing and evaluating surgical TCIs. Report intervention fidelity as well as implementation fidelity for all implementation strategies used. Develop and test scale‐up strategies in the context of implementation trials, to demonstrate how to best adapt surgical TCIs across settings. Some implementation strategies appear costly; economic analyses to demonstrate the benefits of increased costs on outcomes like hospital readmission could be beneficial. Consider reporting the qualifications/training of the person responsible for implementing the surgical TCI to make reporting transparent and replication easier. |
- —National Health and Medical Research Council10.13039/501100000925
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPrimary Care and Health Outcomes · Interprofessional Education and Collaboration · Health Policy Implementation Science
Summary
- Provides key tactics for hospital staff when implementing surgical transitional care interventions, and clear gaps for future researchers such as testing scale‐up strategies.
Introduction
1
Almost 30% of patients who have undergone major surgery have postoperative complications after hospital discharge (Morris et al. 2014). Of these complications, 59% are associated with hospital readmission (Morris et al. 2014) and cost the US healthcare systems $269 million (Brown et al. 2021). There has been growing economic pressure on hospitals to contain costs, with fast‐track protocols being implemented to reduce patient length of stay (Fiona 2014). However, transitioning home quicker may increase patient and caregiver burden if they are not adequately supported to manage the postoperative recovery (Eskes et al. 2023). Common challenges patients and caregivers face include difficulty recognising complications and uncertainty about when and where to seek help, often leading to unnecessary emergency department visits (Kang et al. 2020). Patient education and follow‐up in the community have been suggested to support better postoperative complication management and, in turn, reduce hospital readmissions (Jones et al. 2016). Ultimately, targeted strategies are needed to enhance postoperative care to reduce readmissions for surgical patients.
Background
2
Transitional care interventions (TCIs) are interventions utilised to ensure continuity of care as patients move across healthcare settings (Naylor et al. 2011). They do not have a specific event that denotes their start and end point; they start in hospital and continue after discharge, to support patients and their caregivers to manage recovery (Holland and Harris 2007). TCIs are multi‐component, which is defined as an approach incorporating many strategies to tackle a specific issue, such as behavioural, educational and organisational techniques (Craig et al. 2008). Common components of TCIs include engaging patients and caregivers in care plan development, education and self‐management, and ensuring seamless contact between patients/caregivers and healthcare professionals in the community (Hirschman et al. 2015). One of the most studied and effective TCI models is the Naylor model, which incorporates these components but is primarily applied to older medical patients with multiple chronic conditions (Hirschman et al. 2015). Surgical patients face unique risks, particularly postoperative complications associated with the anaesthetic, surgical procedure and subsequent incision or wound, highlighting the need for TCIs specifically tailored to their needs.
TCIs are proposed to promote surgical patient recovery by enhancing activities of daily living and quality of life, and reducing emergency department visits and hospital readmission rates (Mao et al. 2022). For example, a review found that surgical patients who receive TCIs were 40% less likely to be readmitted to hospital (Mao et al. 2022). TCIs may also positively influence surgical patient perceptions of their transition experience and satisfaction with care received (Tobiano et al. 2025). Evidence suggests that TCIs with more intervention components tend to show more positive outcomes (Tobiano et al. 2025). Despite their potential, TCIs for surgical patients remain an underutilised strategy, presenting a solution waiting to be realised.
However, TCIs are complex interventions, and those implementing TCIs must navigate the inherent tensions of using them in the real world (Fakha et al. 2021). Implementation research focuses on identifying barriers and facilitators to intervention uptake, and identifying implementation strategies to address these barriers and promote the facilitators to ultimately increase intervention adoption (Bauer and Kirchner 2020). The complexity of implementation strategies lies in their need to address multiple factors concurrently, such as providing education, engaging stakeholders, securing resources and ensuring sustainability at the same time (Proctor et al. 2013). Previous reviews tend to overlook the importance of implementation for maximising impact. For example, in a review of TCIs across a range of settings, most researchers failed to report implementation strategies (Rennke et al. 2013). For reviews that are specific to surgical TCIs, most aim to determine intervention effectiveness rather than implementation effectiveness or implementation fidelity (Jones et al. 2016; Mao et al. 2022). Yet, a review on TCIs for older people showed that implementation strategies are critical at both the individual and organisational level to address common barriers such as lack of resources and higher priority for implementation of other initiatives (Fakha et al. 2021, 2023). Before implementing interventions into practice, a clear implementation plan for surgical TCIs is required to ensure intervention outcomes are achieved. Thus, this scoping review aimed to synthesise the evidence on implementation strategies used to implement TCIs for adult surgical patients. This scoping review is complementary to a published review of TCI components and outcomes (Tobiano et al. 2025).
Methods
3
Design
3.1
A scoping review was undertaken, and reported as per the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses extension for Scoping Reviews (PRISMA‐ScR) Checklist (Tricco et al. 2018). The protocol was registered a priori (https://osf.io/kf2v7/). The stages for a scoping review were followed which include: (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, (5) collating, summarising and reporting the results and (6) consultation (Arksey and O'Malley 2005).
Identifying the Research Question
3.1.1
The mnemonic ‘population, concept and context (PCC)’ was used to frame the review question (Peters 2015). The population was adult, hospital surgical patients. The concept was multi‐component TCIs, that occur across the intra‐ and post‐ hospital setting, such as patient education and follow‐up in the community (Holland and Harris 2007). The context was in hospital and post‐hospital, where post‐hospital care was being managed by the patient/caregiver. Thus, the review questions was: ‘What strategies are used to implement TCIs for adult surgical patients?’.
Identifying Relevant Studies
3.1.2
Searches occurred in August 2023, and were updated in June 2025, in the computerised databases Medline, CINAHL and EMBASE. The search strategy used subject headings and search terms, informed by crucial articles in the field and health librarian input (See File S1). Examples of subject headings and search terms were ‘perioperative’, ‘surgical procedures, operative+’, ‘transition’ and ‘transitional care’. Additionally, studies that were included had their reference lists searched for past studies that met eligibility criteria. Finally, Scopus was used to find newer articles that had cited the included articles.
Study Selection
3.1.3
Duplicates were removed in EndNote 20 and then again in Covidence systematic review software (www.covidence.org). Studies were screened independently by two researchers in the Covidence systematic review software package based on eligibility criteria.
Inclusion criteria were:
- TCIs with ≥ 2 components, aimed at adult surgical inpatients, because it aligns with our phenomenon of interest.
- ≥ 1 Intervention components delivered by a nurse, due to their pivotal role (Mao et al. 2022).
- Reports implementation strategies, as this addresses our research question.
- Original peer‐reviewed research and quality improvement projects, in English, published from 2016 to 2025. These criteria were selected to capture a wide range of TCIs, not just those evaluated by randomised controlled trials (Jones et al. 2016; Mao et al. 2022), in a language widely accessible and understood by the research team. Additionally, the date range reflects the release of the World Health Organisation's guidelines for enhancing care transitions (World Health Organization 2016).
Exclusion criteria included:
- Interventions that include post‐hospital components occurring in rehabilitation settings or care facilities, where patients receive 24/7 care from healthcare professionals, due to this being an alternative care pathway.
- Paediatrics, where data for adults cannot be disconnected, as paediatrics necessitate a different approach to TCIs.
- Letters, commentaries, editorials, conference abstracts/presentations, protocols, theses, reviews, grey literature, because of absence of peer review and paucity of detail about implementation strategies.
First, researchers screened titles and abstracts, and those studies labelled ‘include’ or ‘maybe’ had full‐texts retrieved and were screened again. Disagreements were resolved through discussion and unresolved disagreements were adjudicated by a third researcher. Study selection is presented narratively and as a flow diagram (Tricco et al. 2018).
Charting the Data
3.1.4
A data extraction form was designed by our team, which included author/year/country, setting, type of surgery, implementation fidelity (i.e., were implementation strategies used as intended) and intervention fidelity. We piloted the form with six studies and then one researcher extracted data, and a second confirmed its accuracy. A third researcher could arbitrate disagreements, but was not needed.
Collating, Summarising and Reporting the Results
3.1.5
Data extraction tables were summarised narratively.
The first step of data synthesis was to identify patters. Thus, we returned to the original articles, and mapped the strategies used to implement TCIs as per Leeman et al.'s (2017) ‘Five classes of implementation strategies'. These classes include: (1) dissemination strategies defined as activities aimed at raising the understanding, knowledge, attitudes and intentions of staff to adopt the intervention; (2) implementation process strategies which are processes or actions done by the implementation team to plan, choose and integrate the intervention into practice; (3) integration strategies are any actions that address elements supporting or obstructing best possible integration of the intervention; (4) capacity‐building strategies aim to increase people’s overall ability to execute implementation process strategies (described in bullet point 2) and (5) scale‐up strategies are used to implement the intervention in multiple settings. Additionally, we identified who the target audience was for the implementation strategy and the person responsible for enacting the implementation strategy. These data were presented as a table.
Second, the ‘Patterns, Advances, Gaps, Evidence for practice and Research recommendations (PAGER) framework’ was used to synthesise implementation strategy patterns found (Bradbury‐Jones et al. 2021). This was reported in a table starting with Pattern (P), to present the patterns identified when summarising the implementation strategies as per Leeman et al.'s (2017) ‘Five classes of implementation strategies'. Under Advances (A), what the patterns could add into the current body of literature was reported. Based on the review results, the research Gap (G) column was used to identify knowledge gaps whereas Evidence of practice (E) reported suggestions for clinical practice. Lastly, Research recommendations (R) was used to recommend future research based on the previous four domains of the PAGER framework.
Consultation
3.1.6
A health consumer who had experienced surgeries, a surgical ward nurse responsible for discharge planning, and a surgeon reviewed the patterns found and provided their interpretations, which shaped the PAGER findings, discussion and subsequent manuscript. Health consumer engagement is reported using the GRIPP2 reporting checklist (Staniszewska et al. 2017) (See File S2).
Results
4
In total 27 studies are included in our findings. The database search resulted in 5818 articles, and citation searching resulted in 1236 articles (See Figure 1). After removing duplicates and screening, 29 articles were included. The articles by Robertson et al. (2018) and Liu et al. (2019) and Zhang et al. (2020) and Zhang et al. (2021) reported on the same two studies and interventions, however, different outcomes were reported in each article, thus Robertson et al.'s (2018) and Liu et al.'s (2019) articles were counted as one ‘study’ and Zhang et al.'s (2020) and Zhang et al.'s (2021) articles were counted as one ‘study’ when reporting the findings.
PRISMA flowchart.
Study Characteristics
4.1
See File S3 for data extraction. Studies were conducted in Asia (13/27 (48%)) (Zhang et al. 2020, 2021; Hu et al. 2020; Li et al. 2020, 2024; Lin et al. 2025, 2024; Tian et al. 2023; Tseng et al. 2021; Tu et al. 2024; Wang and Gao 2025; Xu 2021; Yang et al. 2023; Zhou et al. 2023), USA (12/27 (44%)) (Robertson et al. 2018; Liu et al. 2019; Aicher et al. 2019; Du 2021; Fisher et al. 2018; Fitz et al. 2020; Grahn et al. 2019; Iseler et al. 2018; Koeckert et al. 2017; Mitchell 2022; Pelt et al. 2018; Weintraub et al. 2018; Zuckerman 2020), Turkey (1/27 (4%)) (Coskun and Duygulu 2022) and Canada (1/27 (4%)) (Ahmadi et al. 2021). The surgical populations in the studies were colorectal and complex abdominal surgery (8/27 (30%)) (Zhang et al. 2020, 2021; Li et al. 2024; Lin et al. 2025, 2024; Zhou et al. 2023; Du 2021; Fisher et al. 2018; Grahn et al. 2019), cardiac (6/27 (22%)) (Tu et al. 2024; Aicher et al. 2019; Iseler et al. 2018; Koeckert et al. 2017; Weintraub et al. 2018; Coskun and Duygulu 2022), orthopaedic (4/27 (15%)) (Tseng et al. 2021; Xu 2021; Mitchell 2022; Pelt et al. 2018), neurological (3/27 (11%)) (Robertson et al. 2018; Liu et al. 2019; Yang et al. 2023; Zuckerman 2020), kidney (2/27 (7%)) (Hu et al. 2020; Li et al. 2020), lung (2/27 (7%)) (Fitz et al. 2020; Ahmadi et al. 2021), urology (1/27 (4%)) (Wang and Gao 2025), and gynaecological (1/27 (4%)) (Tian et al. 2023).
Implementation fidelity was most evident for Leeman et al.'s (2017) ‘implementation process’ strategies. ‘Selecting a change management process’ and ‘assessing the context’ were enacted by explicitly detailing the change management process selected (Xu 2021; Du 2021; Fitz et al. 2020; Mitchell 2022; Zuckerman 2020) and providing data of assessments conducted (Fisher et al. 2018; Fitz et al. 2020; Koeckert et al. 2017; Pelt et al. 2018; Zuckerman 2020). How well or not well ‘staffing changes and role clarification’ went was also frequently reported (5/27 (18.5%)) (Du 2021; Fisher et al. 2018; Iseler et al. 2018; Mitchell 2022; Zuckerman 2020). Additionally, evidence that staff had received training to support intervention delivery was reported in almost one in five studies (5/27 (18.5%)) (Li et al. 2020, 2024; Lin et al. 2025, 2024; Zhou et al. 2023).
Intervention fidelity was not reported in 16/27 (59%) studies. In the remaining 11/27 studies, intervention fidelity ranged from 20 to 100% for intervention components in 8/27 (30%) studies (Tseng et al. 2021; Yang et al. 2023; Du 2021; Fitz et al. 2020; Grahn et al. 2019; Iseler et al. 2018; Mitchell 2022; Zuckerman 2020), and 3/27 (11%) mentioned intervention fidelity but did not report specific results (Hu et al. 2020; Tu et al. 2024; Fisher et al. 2018).
Results of Data Mapping
4.2
The implementation strategies are in Table 1. They were most frequently categorised as ‘dissemination’, ‘integration’ or ‘implementation process’ strategies. The most frequent dissemination strategy was staff education and training to support intervention delivery. This differed from simply making staff aware of the intervention, but instead involved detailed training in areas like vascular medicines and surgery (Aicher et al. 2019), dehydration and acute kidney injury (Grahn et al. 2019), enterostomy skills (Zhang et al. 2020, 2021), education about clinical issues and community resources (Weintraub et al. 2018) and transitional care training inclusive of an exam (Li et al. 2020). The people responsible were not reported.
For integration strategies, the most frequently used strategies were changes to staffing such as hiring staff, role clarification (Du 2021; Fisher et al. 2018; Ahmadi et al. 2021), re‐allocating staff or some of their time (Iseler et al. 2018; Coskun and Duygulu 2022), and integrating new and existing roles (Fisher et al. 2018). Only two studies reported people responsible, which included senior staff such as chief nurses, unit directors and hospital administrations. The second most common integration strategy was changes to electronic systems, including implementing electronic tools for quality monitoring (Zuckerman 2020), adding workflows (Fisher et al. 2018), platforms (Yang et al. 2023; Weintraub et al. 2018) and databases (Li et al. 2020; Tian et al. 2023), and integrating forms into the electronic medical record (Fitz et al. 2020); people responsible were not reported.
Monitoring processes and outcomes, assessing the context, and selecting change management approaches were common implementation process strategies. Examples of monitoring processes and outcomes included readmission data being regularly reviewed for lessons learnt (Weintraub et al. 2018), metrics reported to frontline staff (Du 2021), and in one study intervention fidelity was checked weekly with a WeChat group created to share issues with the implementation process and ensure these were promptly addressed (Hu et al. 2020). Assessing the context tended to focus on examining existing processes and issues in the hospitals (Du 2021; Fisher et al. 2018; Fitz et al. 2020; Koeckert et al. 2017; Pelt et al. 2018; Zuckerman 2020), while stakeholder engagement incorporated a range of hospital staff, as well as patients and caregivers to support the implementatin process (Lin et al. 2024; Zhou et al. 2023; Du 2021; Fisher et al. 2018; Pelt et al. 2018). Finally, change management approaches such as ‘Plan, Do, Study, Act’ (Fitz et al. 2020; Mitchell 2022; Zuckerman 2020), and ‘Promoting Action on Research Implementation in Health Services’ (PARIHS) framework (Xu 2021) were used. People responsible for implementation process strategies were both frontline clinicians, as well as project administrators and research teams members. Table 2 details the synthesis of findings using the PAGER Framework.
Discussion
5
In this scoping review, the most common implementation strategies for surgical TCIs were dissemination strategies (i.e., staff education and training), integration strategies (i.e., staff changes and changes to electronic systems), and implementation process strategies (i.e., change management approaches including assessing the context and monitoring). As per Leeman et al. (2017), all of these implementation strategies are targeted at individuals, teams and systems that must use the intervention in practice (i.e., the delivery system). Less common strategies were capacity‐building strategies for those responsible for leading the change initiative and scale‐up strategies. These strategies help individuals, teams and systems build capacity to adopt the intervention (i.e., the support system) (Leeman et al. 2017). The implementation strategies we found were largely used in the US and Asian countries with patients undergoing colorectal and complex abdominal surgery or cardiac surgery; these contextual factors must be considered by those intending to use the strategies in their setting.
Building staff capacity was brought to the fore in this scoping review. Staff education was a common implementation strategy, which contrasts with previous TCI research that showed detailed training is often lacking, creating a barrier to successful implementation (Fakha et al. 2021; Sadler et al. 2019). As found in our scoping review, the target audience requiring education can be extensive depending on whether a monocentric (i.e., one professional coordinates the whole TCI process) or polycentric (i.e., responsibility for the TCI process is shared amongst a multi‐disciplinary team) approach to surgical TCIs is undertaken (Landi et al. 2024). Yet, capacity‐building for the person responsible for driving the change management process was infrequent in our scoping review. Previous research has shown that those responsible for managing change processes in hospitals often have no formal training in change management, they learn through mentors who may promote misinformation, and they misapply change management approaches like PDSA cycles (Wright et al. 2022). Given that implementation process strategies, such as using change management approaches, were frequent in our scoping review, it underlines the importance of providing training for those leading the change management process, in addition to those delivering the intervention (Lewis and Kulhanek 2022).
Our scoping review highlights the importance of harmonising the resources needed to implement surgical TCIs with desired outcomes like cost‐savings. It was evident in our scoping review that financial support from hospital leaders was required for high‐cost integration strategies like staffing and changes to electronic systems; strategies found to facilitate TCI implementation in other reviews (Fakha et al. 2021; Sadler et al. 2019). Lack of staffing is a common reason TCI implementation fails (Fakha et al. 2021; Sadler et al. 2019), especially if staff in existing roles are expected to take on additional tasks to facilitate the TCI (Fakha et al. 2023). Creating a new role for a designated person to coordinate the whole TCI, often a master's prepared nurse, is a common approach that provides continuity of care for patients and their caregivers, but adds to hospital budgets (Fakha et al. 2021, 2023; Sadler et al. 2019). Overall, further research is needed to demonstrate the cost benefits of surgical TCIs, as previous research has only provided partial economic evaluations, that were descriptive in manner or had issues with quality (Landi et al. 2024; Kast et al. 2021). In the current climate where hospitals are financially constrained and workload and staffing issues are rife (Fakha et al. 2021, 2023); there is a real need to show that implementation strategies result in outcomes, to convince hospital leaders of the need for continuous funding for this approach to care.
Scale‐up strategies were rarely trialled for the surgical TCIs included in this scoping review. TCIs are complex interventions (Gesell et al. 2021) that must be adapted to the population and environment, and coupled with context‐specific implementation strategies, to reduce implementation failure when scaled up (Fakha et al. 2023). Considering that studies included in our scoping review were largely conducted with patients undergoing colorectal and cardiac surgery in Asian countries and the US, future adaptation of these interventions is likely needed to ensure a match between the intervention and the population/setting. A suggested approach is to preserve function (i.e., the core purpose of an intervention or intervention component), but change form (i.e., activities used to carry out functions of intervention, such as intended mode of delivery, materials, intervention dose or providers involved) when transferring surgical TCIs across settings; as form often requires adaptation to make interventions acceptable for the population and setting (Fann et al. 2021). Currently, many TCI researchers define intervention form and measure intervention fidelity, rather than function (Gesell et al. 2021). An increased focus on TCI function would facilitate standardisation of TCI interventions across settings and support maintenance of intervention effectiveness (Gesell et al. 2021; Hawe 2015). However, agreement on the function of surgical TCIs is needed, presenting a future research opportunity. Recently, researchers identified that ideal TCI components for achieving outcomes like reduced readmission included monitoring and managing symptoms after discharge and discharge planning, which must be combined with either staff coordination or patient education and social and community support (Landi et al. 2024). To further enhance the success of scale‐up, context‐specific and theory‐informed implementation strategies ought to be selected and implementation fidelity should be measured and reported (Proctor et al. 2013). Without this, it will be difficult to interpret why the intervention worked or not (Proctor et al. 2013). In summary, knowing the essential function of surgical TCIs would reduce the need for reinventing solutions and selecting overly intensive intervention components, while facilitating the comparison of data across settings for researchers; however, implementation considerations are just as important for assessing the true effectiveness of the intervention (Hawe 2015).
Recommendations for Clinical Practice and Further Research
5.1
We recommend high‐quality change management processes, led by qualified people, be used when implementing TCIs. This could include careful assessment of the context to determine implementation strategies required. Importantly, these strategies should be theory‐informed as this approach is more likely to ensure behaviour change and successful implementation. For future research, we suggest investigation of surgical TCI adaptation, in a way that maintains their function. This could be coupled with testing of the implementation strategies found in this scoping review and measurement of implementation fidelity. Finally, economic evaluations of surgical TCIs are necessary to provide compelling data to increase hospital leader buy‐in for surgical TCI implementation.
Strengths and Limitations
5.2
In terms of study strengths, first, we used a systematic approach when conducting the search and screening, however, there is always the chance that eligible studies were missed. Second, we included both research and quality improvement to provide a more holistic view of the surgical TCI landscape; QI can be viewed as lower quality than research but may provide practical implementation strategies that work in the real world. For limitations, first, we intended to use the Expert Recommendations for Implementing Change (ERIC) implementation strategies framework to identify patterns, as per our published protocol. However, there were 73 ERIC implementation strategies making coding challenging, and as Powell et al. (2015) concluded, ERIC implementation strategies require ongoing work to make them into conceptually distinct categories. We believe that using Leeman et al.'s (2017) classes instead provided a clear and organised framework that could be understood by both clinicians and researchers, aiding practical implementation efforts. Further, scoping review methodology is flexible, allowing adaptations such as this. Finally, the results are limited as there was homogeneity in context and surgical populations; thus, readers must consider the generalisability of the implementation strategies for their context.
Conclusions
6
Our scoping review provides a synthesis of previously used implementation strategies for surgical TCIs, which often include staff education, adequate staffing, changes to electronic systems, and change management processes. Many of these strategies will likely result in increased financial resources, highlighting the need for hospital leader support and evidence of the financial sustainability of surgical TCIs. Underexplored implementation strategies included evaluation of how to scale up TCIs considering their context‐specific nature and capacity‐building to ensure high‐quality change management processes. On the whole, reporting of implementation and intervention fidelity is lacking, and research has been largely confined to Asia and the US with patients who experience colorectal, complex abdominal and cardiac surgery. Overall, there is much work to be done to ensure surgical TCIs are implemented in the real world effectively, to achieve their intended benefits.
Author Contributions
G.T.: conceptualisation, data curation, formal analysis, investigation, methodology, project administration, validation, visualisation, writing – original draft, writing – review and editing. B.M.G.: conceptualisation, formal analysis, methodology, resources, validation, visualisation, supervision, writing – review and editing. K.T.: data curation, formal analysis, investigation, methodology, project administration, validation, visualisation, writing – review and editing. A.M.E.: formal analysis, investigation, validation, visualisation, writing – review and editing. B.P.: formal analysis, investigation, validation, visualisation, writing – review and editing. J.C.: formal analysis, validation, visualisation, writing – review and editing. L.F.: formal analysis, validation, visualisation, writing – original draft, writing – review and editing. W.C.: conceptualisation, formal analysis, investigation, methodology, resources, validation, visualisation, supervision, writing – review and editing.
Ethics Statement
The authors have nothing to report.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
File S1. Search strategy in Medline (EBSCOhost).
File S2. Patient partner engagement in scoping review, informed by GRIPP2‐SF reporting guidelines.
File S3. Study characteristics (N = 27 studies).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ahmadi, N. , L. Mbuagbaw , C. Finley , J. Agzarian , W. C. Hanna , and Y. Shargall . 2021. “Impact of the Integrated Comprehensive Care Program Post‐Thoracic Surgery: A Propensity Score–Matched Study.” Journal of Thoracic and Cardiovascular Surgery 162, no. 1: 321–330.32713635 10.1016/j.jtcvs.2020.05.095 · doi ↗ · pubmed ↗
- 2Aicher, B. O. , E. Hanlon , S. Rosenberger , S. Toursavadkohi , and R. S. Crawford . 2019. “Reduced Length of Stay and 30‐Day Readmission Rate on an Inpatient Vascular Surgery Service.” Journal of Vascular Nursing 37, no. 2: 78–85.31155166 10.1016/j.jvn.2018.11.004PMC 6548444 · doi ↗ · pubmed ↗
- 3Arksey, H. , and L. O'Malley . 2005. “Scoping Studies: Towards a Methodological Framework.” International Journal of Social Research Methodology 8, no. 1: 19–32.
- 4Bauer, M. S. , and J. Kirchner . 2020. “Implementation Science: What Is It and Why Should I Care?” Psychiatry Research 283: 112376.31036287 10.1016/j.psychres.2019.04.025 · doi ↗ · pubmed ↗
- 5Bradbury‐Jones, C. , H. Aveyard , O. R. Herber , L. Isham , J. Taylor , and L. O’Malley . 2021. “Scoping Reviews: The PAGER Framework for Improving the Quality of Reporting.” International Journal of Social Research Methodology 25, no. 4: 457–470. 10.1080/13645579.2021.1899596. · doi ↗
- 6Brown, C. S. , J. R. Montgomery , P. U. Neiman , et al. 2021. “Assessment of Potentially Preventable Hospital Readmissions After Major Surgery and Association With Public vs Private Health Insurance and Comorbidities.” JAMA Network Open 4, no. 4: e 215503.33847752 10.1001/jamanetworkopen.2021.5503 PMC 8044735 · doi ↗ · pubmed ↗
- 7Coskun, S. , and S. Duygulu . 2022. “The Effects of Nurse Led Transitional Care Model on Elderly Patients Undergoing Open Heart Surgery: A Randomized Controlled Trial.” European Journal of Cardiovascular Nursing 21, no. 1: 46–55.33821999 10.1093/eurjcn/zvab 005 · doi ↗ · pubmed ↗
- 8Craig, P. , P. Dieppe , S. Macintyre , S. Michie , I. Nazareth , and M. Petticrew . 2008. “Developing and Evaluating Complex Interventions: The New Medical Research Council Guidance.” BMJ 337: a 1655.18824488 10.1136/bmj.a 1655 PMC 2769032 · doi ↗ · pubmed ↗