Intravenous Immunoglobulin Treatment in Patients With Streptococcal Toxic Shock Syndrome in Southern Sweden: A Retrospective Population-Based Study
Olof Wullt, Charlotta Utbult, Erik Carlson, Oskar Ljungquist, Torgny Sunnerhagen, Anna Bläckberg, Gustav Torisson

TL;DR
A study in southern Sweden found no clear evidence that IVIG treatment improves survival in patients with streptococcal toxic shock syndrome.
Contribution
This is the first population-based study evaluating IVIG's effect on STSS mortality in a real-world setting.
Findings
IVIG-treated patients were younger and had fewer comorbidities but higher disease severity.
Crude analysis suggested lower mortality in IVIG-treated patients, but adjusted analysis showed no significant benefit.
The study highlights risks of bias in observational research for rare diseases.
Abstract
Intravenous immunoglobulins (IVIGs) have been suggested as an adjunctive treatment in streptococcal toxic shock syndrome (STSS), but there are no conclusive trials. In southern Sweden, IVIG is routinely used in certain hospitals but not others. We hypothesized that this would resemble a natural experiment, and we aimed to evaluate the effect of IVIG in patients with STSS. We conducted a population-based retrospective cohort study on STSS cases in southern Sweden from 2017 to 2024. The main exposure was any IVIG treatment, and the primary outcome was 30-day mortality. Cox regression was used, adjusted for lactate, Sequential Organ Failure Assessment score, Charlson Comorbidity Index, and concurrent clindamycin treatment. We modeled IVIG as a time-dependent variable to address immortal time bias. In total, 106 patients fulfilled STSS criteria, of which 56 (53%) were treated with IVIG.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
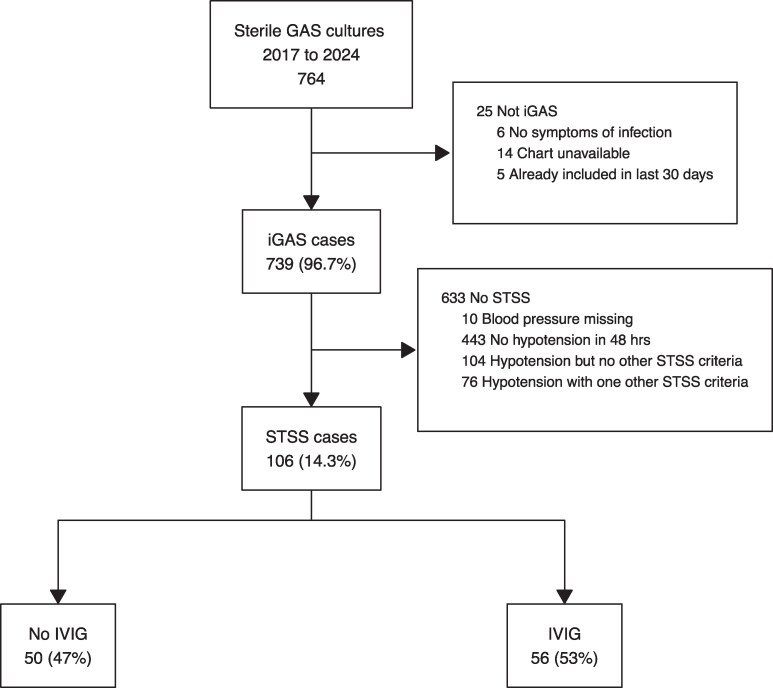 Figure 1
Figure 1| No IVIG (n = 50) | IVIG (n = 56) |
| |
|---|---|---|---|
| Age, y | 65 (52–79) | 60 (49–72) | .17 |
| Male sex | 30 (60) | 40 (71) | .21 |
| Hospital city | <.001 | ||
| Malmö | 24 (48) | 3 (5.4) | |
| Lund | 8 (16) | 23 (41) | |
| Helsingborg | 8 (16) | 21 (38) | |
| Kristianstad | 5 (10) | 9 (16) | |
| Other | 5 (10) | 0 (0) | |
| Comorbidities | |||
| Ischemic heart disease | 9 (18) | 4 (7.1) | .089 |
| Heart failure | 9 (18) | 0 (0) | <.001 |
| Cerebrovascular disease | 3 (6.0) | 3 (5.4) | >.99 |
| Chronic pulmonary disease | 4 (8.0) | 4 (7.1) | >.99 |
| Connective tissue disease | 5 (10) | 6 (11) | .90 |
| Chronic hepatic disease | 2 (4.0) | 3 (5.4) | >.99 |
| Diabetes mellitus | 15 (30) | 4 (7.1) | .002 |
| Active malignancy | 6 (12) | 3 (5.4) | .30 |
| Chronic skin disorder | 11 (22) | 5 (8.9) | .061 |
| Immunosuppression | 8 (16) | 6 (11) | .42 |
| Any chronic comorbidity | 31 (62) | 19 (34) | .004 |
| Home care or nursing home | 8 (16) | 2 (3.6) | .04 |
| Ceiling of care | 6 (12) | 2 (3.6) | .14 |
| Charlson Comorbidity Index | 3 (1–5) | 2 (0–3) | .022 |
| Clinical Presentation | No IVIG (n = 50) | IVIG (n = 56) |
|
|---|---|---|---|
| Symptoms | |||
| Fever | 36 (72) | 40 (71) | .95 |
| Gastrointestinal | 24 (48) | 28 (50) | .84 |
| Localized pain | 14 (28) | 23 (41) | .16 |
| Dyspnea | 12 (24) | 20 (36) | .19 |
| ENT symptoms | 5 (10) | 5 (8.9) | >.99 |
| Erythema | 12 (24) | 7 (13) | .12 |
| Other symptom | 7 (14) | 6 (11) | .61 |
| Disease severity | |||
| Systolic blood pressure, mm Hg | 100 (85–120) | 90 (80–120) | .38 |
| Heart rate per minute | 110 (100–124) | 112 (100–134) | .34 |
| Respiratory rate per minute | 30 (20–36) | 32 (28–40) | .024 |
| Mental alteration | 8 (16) | 14 (25) | .23 |
| NEWS2 score | 8 (6–11) | 10 (8–12) | .005 |
| SOFA score | 7.5 (5–10) | 10 (8–11) | <.001 |
| Lactate, mmol/L | 4.3 (3.2–7.2) | 6.8 (4.9–9.4) | <.001 |
| Septic shock | 42 (84) | 53 (95) | .073 |
| STSS criteria | |||
| Necrosis | 15 (30) | 25 (45) | .12 |
| ARDS | 14 (28) | 20 (36) | .40 |
| Rash | 5 (10) | 19 (34) | .003 |
| Acute renal failure | 37 (74) | 44 (79) | .58 |
| Coagulopathy | 26 (52) | 37 (66) | .14 |
| Liver involvement | 24 (48) | 36 (64) | .091 |
| No IVIG (n = 50) | IVIG (n = 56) | |
|---|---|---|
|
| ||
| 1 | 22 (47) | 35 (65) |
| 89 | 8 (17) | 4 (7.4) |
| 4 | 2 (4.3) | 6 (11) |
| 12 | 5 (11) | 1 (1.9) |
| 28 | 3 (6.4) | 1 (1.9) |
| 22 | 0 (0) | 3 (5.6) |
| 3 | 2 (4.3) | 0 (0) |
| 77 | 1 (2.1) | 1 (1.9) |
| 6 | 1 (2.1) | 0 (0) |
| 81 | 1 (2.1) | 0 (0) |
| 119 | 1 (2.1) | 0 (0) |
| 9 | 0 (0) | 1 (1.9) |
| 44 | 0 (0) | 1 (1.9) |
| 118 | 1 (2.1) | 0 (0) |
| 87 | 0 (0) | 1 (1.9) |
| Infection focus | ||
| Soft tissue | 25 (50) | 30 (54) |
| Pulmonary | 11 (22) | 8 (14) |
| Bacteremia with unknown focus | 7 (14) | 11 (20) |
| Other | 6 (12) | 2 (3.6) |
| ENT focus | 1 (2.0) | 5 (8.9) |
| Positive blood culture | 48 (96) | 51 (91) |
| GAS in another sterile site | 12 (24) | 25 (45) |
| GAS in nonsterile site | 31 (62) | 31 (55) |
| Interventions and Outcomes | No IVIG (n = 50) | IVIG (n = 56) |
|
|---|---|---|---|
| Antibiotics | |||
| Empiric β-lactam | .089 | ||
| Benzylpenicillin | 2 (4.0) | 1 (1.8) | |
| Cloxacillin | 1 (2.0) | 0 (0) | |
| Cefotaxime | 29 (58) | 22 (39) | |
| Piperacillin/tazobactam | 7 (14) | 9 (16) | |
| Carbapenem | 11 (22) | 24 (43) | |
| Adjunctive clindamycin | 36 (72) | 56 (100) | <.001 |
| Other interventions | |||
| Intensive or intermediate care unit | 43 (86) | 56 (100) | .004 |
| Surgical intervention | 21 (42) | 39 (70) | .004 |
| Mechanical ventilation or CPAP | 27 (54) | 45 (80) | .004 |
| Renal replacement therapy | 8 (16) | 27 (48) | <.001 |
| Vasopressor therapy | 42 (84) | 55 (98) | .012 |
| IVIG | |||
| Time to IVIG, h | … | 10 (4–25) | … |
| No. of IVIG doses | … | ||
| 1 | … | 30 (55) | |
| 2 | … | 10 (18) | |
| 3 | … | 15 (27) | |
| Total IVIG dose, g/kg | … | 0.80 (0.57–1.08) | … |
| Outcomes | |||
| Length of stay, d | 16 (12–24) | 32 (14–45) | .010 |
| In-hospital mortality | 17 (34) | 15 (27) | .42 |
| 7-d mortality | 17 (34) | 11 (20) | .094 |
| 30-d mortality | 17 (34) | 14 (25) | .28 |
| 90-d mortality | 17 (34) | 15 (27) | .38 |
| Model | HR | 95% CI |
|
|---|---|---|---|
| Crude | 0.69 | .34–1.41 | .31 |
| Adjusted for SOFA and lactate | 0.50 | .23–1.08 | .08 |
| Adjusted for CCI and clindamycin | 1.01 | .44–2.30 | .98 |
| Time dependent: crude model | 1.18 | .57–2.44 | .66 |
| Final model: adjusted for all | 1.69 | .66–4.30 | .27 |
- —Clinical Health Sciences
- —Maggie Stephens Foundation (to G. T
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Antimicrobial Resistance in Staphylococcus · Neonatal and Maternal Infections
The incidence of invasive group A streptococcus (iGAS) infections has increased in several locations after the COVID-19 pandemic [1]. One of the most severe forms of iGAS is streptococcal toxic shock syndrome (STSS), occurring in 10% to 15% of iGAS cases, with short-term mortality ranging from 23% to 44% [2, 3]. Treatment of STSS includes β-lactam antibiotics as well as adjunctive clindamycin, which has been shown to inhibit bacterial toxin production and improve outcomes [2, 4, 5]. In addition, surgery is often necessary for source control and supportive care, predominantly in the intensive care setting [3, 6].
The survival benefit of adjunctive intravenous immunoglobulin (IVIG) treatment in STSS is debated. Several mechanistic studies have provided biological plausibility for a positive effect [7, 8]. However, clinical studies are limited to 1 prematurely stopped randomized controlled trial and observational studies, with somewhat divergent results [4, 9–17]. A meta-analysis of the crude effect in clindamycin-treated cases from 5 studies, with a population of 165 patients, described a pooled mortality of 16% in the IVIG group, as compared with 34% in the non-IVIG group, suggesting a beneficial effect of IVIG in clindamycin-treated STSS, although the authors acknowledge the risk of confounding and bias [15].
In southern Sweden, the shortage of conclusive clinical studies has led to different interpretations of the current evidence. Consequently, treatment traditions differ among hospitals in the region. In the 2 major university hospitals in Lund and Malmö, adjunctive IVIG is administered routinely in one but not the other. We hypothesized that this would represent a natural experiment, in which the treatment would depend primarily on the site of residence, thus reducing selection bias.
Therefore, we aimed to carry out a population-based study in this region to determine the effect of adjunctive IVIG treatment on 30-day mortality in patients with STSS.
METHODS AND MATERIALS
This retrospective population-based cohort study was conducted in the Skåne region in southern Sweden, with 1.4 million inhabitants. The region is served by 10 hospitals: the 2 university hospitals in Malmö and Lund, 3 midsize hospitals with intensive care units (ICUs; Helsingborg, Kristianstad, and Ystad), and 5 community hospitals without intensive care capacities. Any patient requiring intensive care presenting to a community hospital will be transferred to a hospital with ICU capacity. In the region, all aspects of modern health care are provided except liver transplantation and intensive care for patients with burns. All hospitals in the region are served by the Department of Clinical Microbiology in Lund, with a comprehensive microbiological database. Data were collected through manual review of electronic medical records, as performed by resident physicians (C. U., O. W., E. C.) according to a prespecified protocol and supervised by an infectious disease consultant (G. T.). The primary outcome was 30-day mortality. The study was approved by the Swedish Ethical Review Authority.
Case Finding of iGAS in the Microbiology Database
For case finding, data were retrieved from the Department of Clinical Microbiology in Lund, including cultures with group A streptococcus (GAS) obtained from blood or another normally sterile site (deep tissue biopsy, synovial fluid, cerebrospinal fluid, pericardial fluid, pleural fluid, or another sterile site) between 1 January 2017 and 31 December 2024 in a resident of Skåne region. An episode was excluded if the patient had no symptom of infection at the time of culture or if symptoms could not be determined due to the medical record being unavailable. Patients with GAS in a sterile site and symptoms were considered to have iGAS infection. An individual could be included multiple times in the study if that patient had 2 separate iGAS episodes. To separate iGAS episodes, we required that ≥30 days had elapsed since the previous episode and the patient had been discharged from the hospital in the interim. Baseline was defined as the time point when the iGAS-defining culture had been obtained. Microbiological data included emm types when available.
Definition of STSS Cases
The final study population consisted of patients with STSS, defined in accordance with the definition used by the Working Group on Severe Streptococcal Infections [18]. To fulfill STSS criteria, verified iGAS and hypotension (≤90 mm Hg, systolic blood pressure) were required, with at least 2 of the following: acute respiratory distress syndrome, liver involvement, generalized erythematous rash, coagulopathy, soft tissue necrosis, or renal impairment. Any missing values in STSS criteria (eg, rash was not mentioned in medical record) were considered normal or absent.
Baseline Characteristics
Demographic data were collected, including age, sex, and functional status (if patients were receiving municipal home care or lived in a nursing home). Patients’ preexisting disease burden was evaluated by the Charlson Comorbidity Index (CCI), including age [19]. Other comorbidity data included skin disease predisposing for infection and current immunosuppressive treatment. Ceiling of care status was collected, defined as a doctor's documented recommendation not to escalate to ICU.
Clinical Presentation
We recorded the following symptoms: fever, pulmonary symptoms, gastrointestinal symptoms, localized pain, erythema, symptoms from ear/pharynx, or other (eg, headache). Laboratory values and vital signs at baseline included plasma lactate, platelet count, bilirubin, and creatinine. Vital signs were collected according to the National Early Warning Score 2 (NEWS2), per local routine [20]. We also estimated the Sequential Organ Failure Assessment (SOFA) score at baseline [21]. Occurrence of septic shock was assessed per the Sepsis-3 definition [22].
Interventions
IVIG exposure was defined as having received at least 1 dose of IVIG with the purpose of treating STSS. The number of doses, total accumulated IVIG dose, and time from baseline to first IVIG administration were collected. Normally, IVIG would be administrated in a dose of 1 g/kg (maximum, 50 g) on day 1, with subsequent doses day 2 and 3 if the patient is still in shock. Other in-hospital interventions and treatments included choice of β-lactam antibiotic and whether adjunctive clindamycin was given. In addition, surgery, ICU care, ventilator treatment, renal replacement therapy, and vasopressor treatment were recorded. Infection focus was determined subjectively by the reviewer at the end of each chart review, incorporating symptoms, culture findings from sterile and nonsterile sites, radiologic findings, ICD codes from surgery notes, and discharge. Outcomes included 30-day mortality (primary outcome) as well as 7-day mortality, in-hospital mortality, 90-day mortality, and length of stay for those surviving to discharge.
Statistical Analysis
All variables in the IVIG and non-IVIG groups were presented as median (IQR) or count with percentage. Groups were compared with Fisher exact tests, χ^2^ tests, and Mann-Whitney tests, as appropriate. In case of missing values, we used complete case analysis for the specific variables. In the estimation of composite scores such as CCI, SOFA, or NEWS2, missing values in the different subitems were assumed to be normal; for example, if bilirubin had not been obtained, we considered this to be normal, resulting in 0 points for this subitem when calculating the SOFA score.
The crude effect on the risk for 30-day mortality was estimated by a Cox proportional hazards model and presented as a hazard ratio (HR) with 95% CIs. The exposure was coded as 0 = no IVIG and 1 = IVIG and the outcome as 0 = alive and 1 = deceased. Thus, an HR <1 would be in favor of IVIG. To address imbalances between the IVIG and non-IVIG groups, adjustments were made for disease severity (plasma lactate, SOFA score), comorbidities (CCI with age), and adjunctive clindamycin treatment. A priori selection of these variables was based on previous research and their clinical relevance. A time-to-event model was chosen to address immortal time bias, with IVIG as a time-dependent variable. In this analysis, patients who received IVIG belonged to the non-IVIG group until the first dose of IVIG was given, after which they were allocated to the IVIG group. To visualize the effect and direction of selection bias, these adjustments were performed stepwise in the Cox proportional hazards model, with each variable added individually and plotted in a forest plot. To determine which other factors were associated with mortality, we performed an exploratory analysis with univariate Cox regression models for each variable vs the primary outcome. All analyses were performed in R, and the code is found at www.github.com/gtorisson/iGAS.
RESULTS
In total, 764 episodes with GAS obtained from a sterile site were identified. Of these episodes, 25 (3.3%) were excluded for a lack of symptoms (n = 6), unavailable charts (n = 14), and previous inclusion in the preceding 30 days (n = 5). The remaining 739 episodes were considered iGAS episodes, occurring in 734 individuals, with 5 persons having 2 iGAS episodes during the 8-year follow-up. In total, 106 episodes (14.3%) in 106 unique patients fulfilled STSS criteria upon review, with 56 subsequently receiving IVIG and 50 not (Figure 1). As hypothesized, the proportion of patients with STSS receiving IVIG differed among hospitals in the region: in Malmö, 3 of 27 (11%) received IVIG; in Lund, 23 of 31 (74%); and in Helsingborg, 21 of 31 (68%).
Flowchart describing the identification of patients with STSS. GAS, group A streptococcus; iGAS, invasive group A streptococcus; IVIG, intravenous immunoglobulin; STSS, streptococcal toxic shock syndrome.
The median age was 62 years, with IVIG recipients being younger than those who did not receive IVIG. Most comorbidities were less frequent in the IVIG group, including heart disease, diabetes, and malignancies. The group receiving IVIG also had a lower Charlson comorbidity score and were less likely to have home care or a ceiling of care decision (Table 1).
Symptoms were similar across groups, with fever and gastrointestinal symptoms being the most common, occurring in approximately 70% and 50%, respectively. Disease severity was higher in the IVIG group, as reflected by lower blood pressure, higher NEWS2 and SOFA scores, and higher plasma lactate. All STSS criteria were more common in the IVIG group (Table 2).
The most frequent emm type was emm 1 in both groups, occurring in 57 of 106 (54%), slightly more common in the IVIG group. The most common source of infection was soft tissue infections, in 55 of 106 (52%) patients. Infection foci were quite similarly distributed between the groups. A positive blood culture was obtained in 99 (93%) episodes. In patients receiving IVIG, a larger proportion had GAS in other sterile sites as well (Table 3).
In IVIG recipients, the median time from baseline to the first IVIG dose was 10 hours. Of 56 patients, 30 received a single IVIG dose, 10 two doses, and 15 three doses (in 1 case, the number of doses could not be determined). The median accumulated dose equaled 0.8 g/kg. Patients in the IVIG group received empiric carbapenems to a greater extent as well as adjunctive clindamycin treatment. All other interventions, including surgery, were also more common in the IVIG group (Table 4).
The primary outcome (30-day mortality) occurred in 31 of 106 (29%) patients. The median time to death was 27 hours (IQR, 18–73) from baseline. In the non-IVIG group, all patients died within the first 7 days. The 30-day mortality rate was 14 of 56 (25%) in the IVIG group and 17 of 50 (34%) in the non-IVIG group, resulting in a crude HR of 0.69 (95% CI, .34–1.41). When adjustments were made for CCI and clindamycin treatment, the HR increased. When adjustments for lactate and SOFA were included, the HR decreased. Finally, when the model was adjusted for immortal time bias and all covariates, the HR for IVIG was 1.69 (.66–4.30; Table 5, Supplementary Figure 1).
In the exploratory univariate analysis of other factors associated with outcome, age, comorbidities, and functional dependency were more strongly associated with mortality than markers of acute disease severity (Supplementary Tables 1–3).
DISCUSSION
In this population-based observational study, we found no clear evidence of an effect of IVIG treatment on 30-day mortality in patients with STSS. Our hypothesis of a natural experiment was disproved, as there were substantial differences between the groups, which complicated the interpretation of our results.
As hypothesized, a greater proportion of patients with STSS in Lund and Helsingborg received IVIG as compared with Malmö. Despite this, we observed considerable between-group differences: patients who received IVIG were younger and less frail, with fewer chronic diseases and less functional impairment. There were also clear indications of higher acute disease severity in the IVIG group, with greater NEWS2 and SOFA scores, as well as increased plasma lactate. Patients receiving IVIG were more likely to receive other interventions, including surgery and adjunctive clindamycin treatment. These group differences resemble those found in previous observational studies, where patients receiving IVIG were younger, had fewer comorbidities, and were treated with adjunctive clindamycin to a larger extent [4, 9, 10].
The crude HR estimate of 0.69 for IVIG vs 30-day mortality signaled that receiving IVIG was associated with a 31% decrease in crude mortality. However, the aforementioned group differences suggest selection bias. The higher disease severity in patients receiving IVIG is likely to have increased the apparent mortality in this group. Consequentially, adjusting for lactate levels and SOFA score, the HR decreased from 0.69 to 0.50. Correspondingly, the younger age, lower degree of comorbidity, and higher frequency of adjunctive clindamycin treatment may have decreased the apparent mortality in the IVIG group. Subsequently, upon adjusting for CCI and clindamycin treatment, the HR increased from 0.69 to 1.01. Table 5 and Supplementary Figure 1 illustrate how different adjustments with regard to selection bias may lead to different results. With small sample sizes, composite clinical scores reduce the number of adjustment variables, mitigating the risk of overfitting. We used CCI and SOFA scores to enable separation of chronic comorbidity and acute disease severity. Previous studies have used scoring based on APACHE II (Acute Physiology and Chronic Health Evaluation II) [9, 23] or SAPS II (Simplified Acute Physiology Score) [10, 16, 24]. These scores combine markers for disease severity and comorbidities but are tilted toward measuring current disease severity. Therefore, adjusting for these would only to a lesser degree adjust for differences in comorbidities, which could retain bias. This was supported by our exploratory analysis, in which chronic conditions appeared more strongly associated with mortality than acute disease severity.
Observational studies evaluating an intervention occurring after baseline also risk being subjected to immortal time bias [25, 26]. This risk becomes pronounced when the outcome occurs soon after baseline and the intervention is delayed. This might be the case if the administration of IVIG is withheld until a definitive microbiological diagnosis is made. In our patients, mortality occurred early, at a median 27 hours after baseline. Immortal time bias may have favored IVIG treatment in the crude analysis, as these patients would by definition have survived the initial critical period before receiving IVIG. However, treatment was not extensively delayed, with a median time to IVIG of 10 hours, indicating that many patients received IVIG before a definitive microbiological diagnosis. When IVIG was modeled as a time-dependent covariate, the HR increased from 0.69 to 1.18, suggesting that immortal time bias may have influenced crude results. Yet, the exact reason for initiating IVIG treatment at that time point was not known. If IVIG was used as a “last resort” due to further clinical deterioration from baseline, time-dependent modeling may also introduce bias, disfavoring IVIG if given too late [27].
Strengths of this study include a population-based cohort that is characterized in large detail, including exact times for IVIG distribution and outcome. This is the first observational study on adjunctive IVIG in STSS attempting to address immortal time bias, with a larger study population than most studies on this subject [4, 9–12, 14, 17]. However, despite covering >10 million person-years of follow-up, only 106 STSS cases were included. Although certain aspects of the hypothesis of a natural experiment were correct, it failed in creating a balance in covariates between the treatment groups, which is a major limitation. In our most comprehensive model, we included 5 covariates despite having only 31 events, suggesting overfitting; this precluded further adjustments, such as choice of β-lactam, which may have influenced results. The accumulated dose of IVIG was lower than in many recommendations, which may have affected the results. Data on the reason to choose a specific dosage regime were not available, but the presence of acute respiratory distress syndrome or acute kidney failure could have led to lowered doses. Furthermore, although the medical records were generally well documented, some records were incomplete. The representativity of our study population could be questioned: applying STSS criteria retrospectively will most likely identify a population slightly different from that in a prospective setting. Nevertheless, 90% of cases fulfilled septic shock criteria, and the proportion of iGAS cases fulfilling STSS criteria and mortality rates were similar to previous studies [3].
This study highlights the challenges with observational studies involving rare conditions. Small sample sizes and unbalanced groups limit the possibilities to adjust for confounders, reducing the ability to draw conclusions. A lack of power is also an issue, with clinically relevant differences being statistically insignificant. Our result regarding immortal time bias further signals that the interpretation of observational studies is intricate. We conclude that a randomized controlled trial is required to determine if adjunctive IVIG is beneficial or not in STSS. Such a study would preferably randomize patients early, before a definitive microbiological diagnosis, accepting the risk of administering IVIG to patients not having STSS. Owing to the rarity of STSS, such an randomized controlled trial must be an international collaboration to reach statistical power.
CONCLUSION
Although our study included a large population of patients with STSS, our results were inconclusive regarding the effect of IVIG on 30-day mortality. This study highlights the risk of bias in observational studies in rare conditions. Prospective interventional studies are needed to determine the efficacy of IVIG in patients with STSS.
Supplementary Material
ofag092_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wrenn K, Blomquist PB, Inzoungou-Massanga C, et al Surge of lower respiratory tract group A streptococcal infections in England in winter 2022: epidemiology and clinical profile. Lancet 2023; 402:S 93.37997140 10.1016/S 0140-6736(23)02095-0 · doi ↗ · pubmed ↗
- 2Brouwer S, Rivera-Hernandez T, Curren BF, et al Pathogenesis, epidemiology and control of group A Streptococcus infection. Nat Rev Microbiol 2023; 21:431–47.36894668 10.1038/s 41579-023-00865-7PMC 9998027 · doi ↗ · pubmed ↗
- 3Schmitz M, Roux X, Huttner B, Pugin J. Streptococcal toxic shock syndrome in the intensive care unit. Ann Intensive Care 2018; 8:88.30225523 10.1186/s 13613-018-0438-y PMC 6141408 · doi ↗ · pubmed ↗
- 4Carapetis JR, Jacoby P, Carville K, Ang SJ, Curtis N, Andrews R. Effectiveness of clindamycin and intravenous immunoglobulin, and risk of disease in contacts, in invasive group A streptococcal infections. Clin Infect Dis 2014; 59:358–65.24785239 10.1093/cid/ciu 304 · doi ↗ · pubmed ↗
- 5Andreoni F, Zürcher C, Tarnutzer A, et al Clindamycin affects group A Streptococcus virulence factors and improves clinical outcome. J Infect Dis 2017; 215:269–77.27247345 10.1093/infdis/jiw 229 · doi ↗ · pubmed ↗
- 6Björck V, Påhlman LI, Bodelsson M, Petersson A-C, Kander T. Morbidity and mortality in critically ill patients with invasive group A Streptococcus infection: an observational study. Crit Care 2020; 24:302.32505194 10.1186/s 13054-020-03008-z PMC 7275847 · doi ↗ · pubmed ↗
- 7Norrby-Teglund A, Stevens DL. Novel therapies in streptococcal toxic shock syndrome: attenuation of virulence factor expression and modulation of the host response. Curr Opin Infect Dis 1998; 11:285–91.17033393 10.1097/00001432-199806000-00004 · doi ↗ · pubmed ↗
- 8Basma H, Norrby-Teglund A, Mc Geer A, et al Opsonic antibodies to the surface M protein of group A streptococci in pooled normal immunoglobulins (IVIG): potential impact on the clinical efficacy of IVIG therapy for severe invasive group A streptococcal infections. Infect Immun 1998; 66:2279–83.9573118 10.1128/iai.66.5.2279-2283.1998 PMC 108192 · doi ↗ · pubmed ↗