Effects of Earthquake Fear and Post-Traumatic Stress Disorder on Patients with Irritable Bowel Syndrome after a Major Earthquake in Türkiye: A Multicenter Study
Rasim Eren Cankurtaran, Hulusi Can Karpuzcu, Engin Ataman, Gokhan Aydin, Kenan Kosar, Sedat Cicek, Fatih Kivrakoglu, Batuhan Baspinar, Emre Dirican

TL;DR
This study shows that PTSD and earthquake fear worsen symptoms and quality of life in IBS patients after a major earthquake in Türkiye.
Contribution
The study identifies PTSD and earthquake fear as key predictors of IBS severity and quality of life in post-earthquake settings.
Findings
IBS patients in earthquake zones had significantly higher symptom severity and lower quality of life than those in non-earthquake zones.
PTSD (PCL-5) was the strongest predictor of IBS symptom severity and quality of life.
Fear of earthquakes (FES) also significantly predicted IBS outcomes.
Abstract
: On February 6, 2023, 2 devastating earthquakes struck south-eastern Türkiye, causing over 100 000 injuries and more than 50 000 deaths. This study aimed to investigate the impact of post-traumatic stress disorder (PTSD) and fear of earthquake on the severity of irritable bowel syndrome (IBS) symptoms and IBS-related quality of life (IBS-QoL). : Participants diagnosed with IBS were categorized into 2 groups: those residing in earthquake zones and those in non-earthquake zones. Data regarding demographic characteristics, IBS Symptom Severity Scale (IBS-SSS), IBS-QoL, Post-traumatic Stress Disorder Checklist for Diagnostic and Statistical Manual of Mental Disorders-5th edition (PCL-5), and Fear of Earthquake Scale (FES) were collected through validated questionnaires. Multivariate analyses, multiple linear regression, and elastic net (EL) models were performed to identify predictors of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1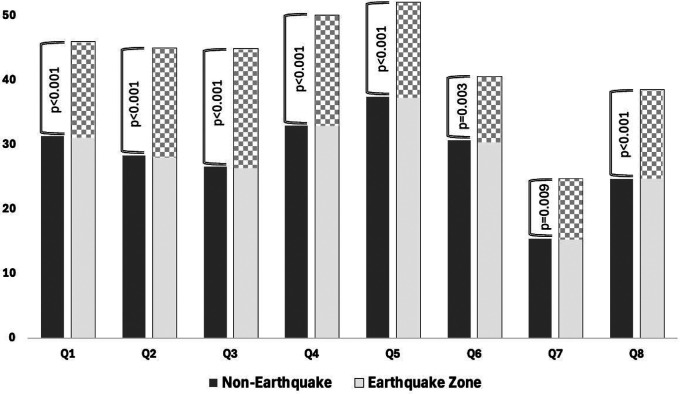 Figure 2
Figure 2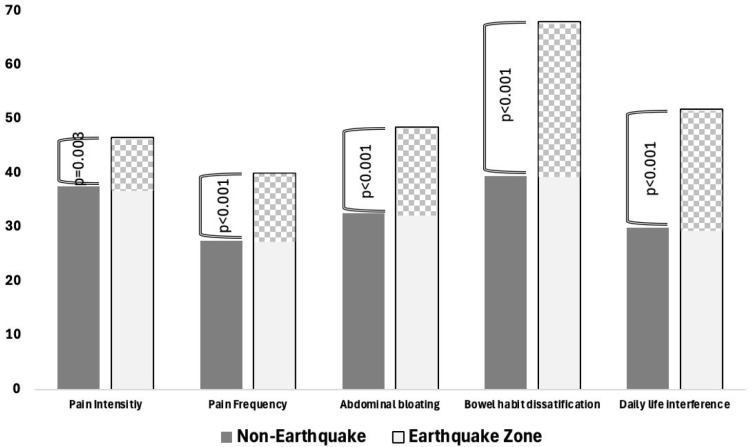 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPosttraumatic Stress Disorder Research · Psychosomatic Disorders and Their Treatments · COVID-19 and Mental Health
Introduction
Irritable bowel syndrome (IBS) is a common functional gastrointestinal disorder characterized by chronic abdominal pain and changes in stool frequency or consistency.1 It is the most commonly diagnosed functional gastrointestinal disorder, accounting for approximately one-third of all gastroenterology admissions.2 Although there are regional variations, the prevalence of IBS is generally estimated to be between 10% and 15%.3^,^4 The direct or indirect cost of IBS has been reported to be between 7700 per patient per year.5 It is also known that IBS is a disease that is not limited to treatment costs, but also negatively affects the quality of life (QoL) of patients, causes fatigue, restricts physical activities, and keeps their general health perception lower than the general population.6
Although IBS is a common disorder, its pathophysiology has not been clearly elucidated. With ongoing research and the updating of the Rome criteria, the mechanism of brain-bowel interaction has come to the fore in recent years.7^,^8 Psychosocial factors are one of the important factors in the etiology of IBS.9 It has been reported that abuse and trauma in early life are associated with the development of IBS in adulthood.10 Post-traumatic stress disorder (PTSD) is an important clinical condition associated with IBS.^11^ The PTSD is characterized by symptoms following exposure to a physical or emotional traumatic event, such as re-experiencing the event, avoidance of triggers, development of negative thoughts and moods, and symptoms of chronic hyperarousal.12 Many recent studies have found PTSD to be an independent risk factor for IBS.13^,^14 In these studies, it was observed that IBS symptoms were common in soldiers returning after war.
On February 6, 2023, 2 major earthquakes measuring 7.7 and 7.8 on the Richter scale struck south-eastern Türkiye, causing over 100 000 injuries and more than 50 000 deaths. In addition, many problems such as shelter, nutrition, and access to health services emerged after the earthquake, and many people had to migrate to other cities.15 The earthquake not only caused financial loss and physical damage but also had a significant negative impact on people’s mental health.16 A recent study reported that nearly one-fifth of individuals affected by the February 6 earthquake continued to meet the diagnostic criteria for PTSD even at the end of the first year.^17^ Although numerous publications in the literature have investigated various bodily systems in individuals affected by this earthquake, no articles were identified that examined its effects on the gastrointestinal system.18^,^19 Focusing specifically on IBS among gastrointestinal disorders, it was observed that previous studies investigating the effects of earthquakes on this condition were also highly limited.20
This study aimed to evaluate the impact of PTSD and earthquake-related fear on symptom severity and QoL in patients with IBS. An additional aim was to shed light on the effect of the earthquake on patients with IBS by comparing patients with IBS in the earthquake zone with patients in the non-earthquake zone. Furthermore, the study sought to contribute to the limited existing literature on how earthquakes may affect IBS.
Materials and Methods
Study Design and Participants
This was a cross-sectional study conducted in 6 centers in Turkiye between February 3, 2024, and March 3, 2024. All participants with IBS were divided into 2 groups: the earthquake zone group and the control group. Five centers from the earthquake-affected region (Hatay, Adıyaman, Kahramanmaraş, Osmaniye, and Kilis) and 1 center from Ankara (as the control site) participated in the study. The study included consecutive adult outpatients diagnosed with IBS according to Rome IV criteria at gastroenterology clinics, regardless of subtype, who gave informed consent. Patients with severe mood disorders, impaired mental function, organ failure, or organic gastrointestinal diseases (e.g., IBD, pancreatitis, or malignancy) were excluded. Individuals who were unable to complete the questionnaire in Turkish and those who refused to participate in the study were also excluded. In addition, patients who had migrated to the control center after experiencing the earthquake were excluded from the control group to avoid misclassification. Ethical approval was obtained from the Ankara Etlik City Hospital ethics committee, and the study was conducted in accordance with the tenets of the Declaration of Helsinki (Date: January 31, 2024, approval number: AEŞH-BADEK-2024-094). Written informed consent was obtained from all participants prior to enrollment in the study
Data Collection
Data related to demographic characteristics such as age, gender, comorbidities, educational, and marital status were obtained by questionnaires from the participants. Information such as injuries in the earthquake, death of relatives, damage to the house, and economic losses were also obtained from the patients in the earthquake zone group. The IBS Symptom Severity Scale (IBS-SSS) was used for the IBS severity score and the IBS-QOL scale for IBS-related QoL. The PTSD Checklist-5 (PCL-5) scale, developed by summarizing the Diagnostic and Statistical Manual of Mental Disorders-5th edition (DSM-5), was used to measure PTSD symptoms. In order to evaluate the level of earthquake fear, the Fear of Earthquake Scale (FES) was used.
Irritable Bowel Syndrome Symptom Severity Scale
The IBS-SSS is a summary score that includes several IBS-related measures, such as intensity of abdominal pain, frequency of pain episodes, bloating, satisfaction with bowel habits, and QoL, each scored from 0 to 100. The total score ranges from 0 to 500, providing an overall assessment of IBS severity. Severity classification includes mild (75-175), moderate (175-300), and severe (>300) categories.21
Irritable Bowel Syndrome Quality of Life
According to Patrick et al22 and Drossman et al,23 a questionnaire consisting of 34 items was administered, each rated on a 5-point Likert scale. The questionnaire covers 8 subscales: dysphoria, interference with activity, body image, health worry, food avoidance, social reactions, sexual issues, and relationships. Scores for each subscale range from 0 to 100. Higher scores on this instrument are indicative of lower QoL. The validated Turkish version of the IBS-QoL questionnaire validated by Uran et al24 was used in this study.
Post-traumatic Stress Disorder Checklist for Diagnostic and Statistical Manual of Mental Disorders—Fifth Edition
The PCL-5, as described by Weathers et al25 and revised by Blevins et al,26 is a 20-item self-report questionnaire designed to assess PTSD symptoms according to DSM-5 criteria. Each symptom is rated on a 5-point Likert scale ranging from 0 (not at all) to 4 (extremely). The cumulative scores of all items give a total symptom severity score ranging from 0 to 80. The Turkish version of the PCL-5 was validated by Boysan et al,^27^ who found a validated cut-off score of 47 for the purposes of this study.
Fear of Earthquake Scale
The FES was developed to measure the level of fear associated with earthquakes.28 It consists of 7 items and uses a 5-point Likert scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). The total score on this scale ranges from 7 to 35 points. The Turkish adaptation of the questionnaire was developed by Sarı et al.29
Statistical Analysis and Simple Size
In this study, the data were analyzed using SPSS 25 (IBM SPSS Corp.; Armonk, NY, USA) and R Studio Team (2020). (RStudio; Boston, MA, USA) http://www.rstudio.com/ 2023.06.1+524 version, “caret v6.0-94,” “dplyr v1.1.4,” and “elastic net v1.3” packages. Mean, standard deviation, median (Q1-Q3), frequency, and percentage values were used for descriptive statistics. Normality assessment was made with Shapiro–Wilk and Kolmogorov–Smirnov tests. Student’s t-test, Mann–Whitney U, and chi-square tests were used in univariate analyses. Univariate and multivariate logistic regression (with enter method) analyses were performed for the case where IBS-SSS categories (moderate-severe) were the dependent variable. Odds ratio (OR) and 95% CI are given for this analysis. For the case where IBS-QOL scores were the dependent variable, univariate analyses, correlation analysis, and the routine comparison tests mentioned above were used. For the dependent variable in question, linear regression analysis was performed by ensuring model qualifications (linearity, independence, homoscedasticity, normality, and multicollinearity) with the backward elimination method. In addition, an elastic net (EL) model was constructed with the same independent variables for both deviations from simplistic qualifications and variable importance for the dependent variable in question. The EL procedure is a form of regularized optimization for linear regression that provides a bridge between ridge regression and the lasso.30 In addition, this method simultaneously does automatic variable selection and continuous shrinkage, and it can select groups of correlated variables.31 After the parameters were determined α = 0.3, λ = 2.36 for final EL model) with 10-fold cross validation (all data were accepted as both training and test sets), the order of importance of the variables contributing to the prediction was determined.
In the general score types (FES, PCL-5, IBS-SSS, IBS-QOL), a pilot study conducted with those from the earthquake zone (n = 20) and those from the non-earthquake zone (n = 20) found high effect sizes and the required sample sizes for each score type (1.72 (n = 14), 0.71 (n = 68), 0.95 (n = 38), 0.65 (n = 176), respectively). Sample sizes were calculated by taking the 2-sided hypothesis into account, assuming the type I error was 0.05 for 80% statistical power. However, due to higher power (99%) and possible data loss, it was decided to conduct the study with a total of 225 individuals. G*Power 3.1.9.4 program was used in statistical power calculations.
Results
Out of 241 IBS patients, 225 were included in the study, 117 (52%) from earthquake centers and 108 (48%) from non-earthquake centers. Due to incomplete questionnaire responses or refusal to participate, a total of 16 IBS patients were excluded from the study. Age (P = .137), sex (P = .763), marital status (P = .513), educational status (P = .289), place of residence (P = .137), and other variables showed similar differences between the 2 groups. Significant differences were likely to be found for some of the earthquake-specific questions. The detailed results of the variables are shown in Table 1.
When the scale scores were evaluated according to earthquake experience (Table 2), it was observed that all of the total scale scores were higher in patients in the earthquake zone. Scores for IBS-SSS, IBS-QOL, FES, and PCF-5 were significantly higher in the earthquake region (249, 44.1, 20, and 47, respectively) compared to the non-earthquake region (141, 22.8, 9, and 28, respectively) (P < .001 for all).
When IBS-QOL subscores in the Q1-Q8 range were evaluated according to both groups, statistically significant elevation of all subscores in patients in the earthquake zone group was noted (Figure 1). In addition, IBS-SSS subscores such as pain intensity (P = .003), pain frequency (P < .001), abdominal bloating (P < .001), bowel habit dissatisfaction (P < .001), and daily life interference (P < .001) were also significantly higher in the earthquake zone group (Figure 2).
Independent risk factors affecting the severity of IBS-SSS were evaluated separately according to the presence of moderate-to-severe IBS by univariate and multiple regression analysis (Table 3). A 10-point increase in FES score was associated with approximately a 2.36-fold higher likelihood of moderate-to-severe IBS-SSS (95% CI: 1.37-4.09), whereas a 10-point increase in PCL-5 score corresponded to a nearly 1.70-fold increase in risk (95% CI: 1.37-2.11). When the effect of living in an earthquake zone as the primary variable on the severity of IBS-SSS was analyzed according to univariate and multivariate approaches when the effect of other variables was controlled, living in an earthquake zone was found to be significant in univariate analysis (OR = 4.882, CI: 2.775-8.591, P < .001), but not in multivariate analysis (P = .316). However, PCL-5 and FES scores were significant in both univariate analysis (OR = 1.076, CI: 1.055-1.097, P < .001 and OR = 1.185, CI: 1.130-1.243, P < .001) and multivariate analysis (OR = 1.057, CI: 1.034-1.080, P < .001 and OR = 1.082, CI: 1.013-1.156, P = .019).
Multiple linear and EL models were created by comparing IBS-QOL scores for possible risk factors and then defining them as dependent variables (Table 4). While gender (P < .001), marital status (P < .042), educational status (P = .03), living in the earthquake zone (P < .001), history of psychiatric follow-up (P = .015), and some other earthquake-related variables were significant in the baseline comparison, only PCL-5 (P < .001) and FES (P = .006) were significant in the multiple model. In addition, according to the EL model, PCL-5 was the most important variable (100%) and FES was the second most important variable (38%) in predicting IBS-QOL scores.
Discussion
This study found that IBS patients in the earthquake zone had higher IBS severity and QoL scores than IBS patients in the non-earthquake zone. In addition, the PTSD and FES scores of the patients in the earthquake zone were significantly higher than those in the control group. However, the main important findings of the study were that living in the earthquake zone was not found to be an independent risk factor in terms of IBS-SSS and IBS-QOL, while PCL-5, which is an indicator of PTSD, and FES scores, which are indicators of fear of earthquakes, were found to be independent risk factors for both scores.
Although the pathophysiology of IBS is still not clearly elucidated today, there are increasing views on the mechanism of the brain-gut axis.32 Many studies have put forward various hypotheses in this direction.33^,^34 In a recent review, it was emphasized that the gut microbiota is effective in the gut-brain axis interaction, and for this reason, IBS is associated with many neuropsychiatric disorders.34
Post-traumatic stress disorder is one of the important clinical conditions whose relationship with IBS has been investigated in recent years. Irritable bowel syndrome is highly associated with other neuropsychiatric disorders and PTSD. In a study investigating the association of neuropsychiatric disorders with IBS, it was reported that 54% of IBS patients had a history of psychiatric illness, 44% had a history of trauma, and 36% had current PTSD.35 Recent studies have suggested that there are both molecular and genetic factors that may explain the association between IBS and PTSD.36^,^37 In particular, neuropeptide Y levels and activity have been reported to play a key role in the association between PTSD and IBS.^37^ Additionally, several hypotheses have proposed that this relationship may be mediated through dysregulation of the hypothalamic–pituitary–adrenal axis, alterations in gut–brain axis signaling, and stress-related changes in the intestinal microbiota.38 Although the underlying mechanism is still unclear, the close relationship and association between PTSD and IBS has been the subject of research in many studies. In a meta-analysis of 8 studies, the presence of PTSD was associated with an increased likelihood of IBS.9 Another study reported that PTSD in veterans was a significant risk factor for IBS in a condition called Gulf War illness, which is characterized by some gastrointestinal symptoms.39 In another study including veterans with symptomatic PTSD, IBS was found to be more common than in the general population, and severe PTSD was found to be a risk factor for the severity of gastrointestinal symptoms such as diarrhea, constipation, and bloating.40 In the study, PTSD severity was a significant risk factor for IBS-SSS, which is similar to this study. In a recent population-based study involving 1617 civilians exposed to war, it was found that some war-related events were significantly associated with IBS. Another important result of this study was that a significant association was found between PTSD and IBS.41 The study was related to earthquake and IBS, and the population without earthquake exposure was also included in the study. No association was identified between earthquake-related factors such as death of a family member, financial problems, trauma, and IBS severity in the study. However, although these data related to earthquake exposure were included in the study, making a comparison with this study may not be appropriate due to the lack of a standardized trauma exposure scale, the inclusion of the population without exposure, and the lower number of participants in the study compared to population studies.
Until this part of the article, all the studies examining the relationship between PTSD and IBS in the literature consisted of veterans and civilians exposed to war.14^,^39^-^41 Another important objective of the study was to evaluate the effect of earthquake fear on IBS severity and QoL. However, only a limited number of studies investigating the relationship between earthquake and IBS were identified in the literature.20 In that study, it was reported that the implementation of a health education program for students diagnosed with IBS after the earthquake significantly decreased IBS-QOL scores and had a positive effect on the participants. Although that was an interventional study and therefore not directly comparable with the cross-sectional design, it further reinforces the notion that earthquake-related psychosocial distress can meaningfully influence IBS outcomes. In line with those findings, the results similarly indicate that post-traumatic psychological factors such as PTSD and earthquake-related fear may play a critical role in symptom burden and QoL among IBS patients. In the study, the FES score, which is an earthquake fear scale, was an independent risk factor for IBS-SSS and IBS-QOL, just like PTSD. The fact that FES also significantly increased the severity of IBS shows us that psychosocial factors should be evaluated as a triggering factor. Although the IBS-SSS and IBS-QOL scores of IBS patients in the earthquake zone were higher than those in the non-earthquake zone, living in the earthquake zone was not an independent risk factor affecting these scores. In this case, the presence of patients with severe IBS in the non-earthquake region and the presence of patients with high PTSD scores due to other causes, such as abuse and trauma, may be effective.
The study had several limitations. The first was that the study started 1 year after the earthquake. This may have influenced and weakened the association between IBS and the earthquake. Another limitation was that the study was not a population-based field survey, but a cross-sectional study of patients who presented to the participating health centers, without longitudinal follow-up. Finally, although the prevalence of psychiatric history or current psychiatric follow-up was included in the study, detailed information on the use of psychotropic medications was not available. This may be considered a limitation, as such medications could potentially influence IBS symptoms.
In conclusion, this study found that PTSD and FES scores were independent risk factors affecting IBS severity and IBS-related QoL. While evaluating these patients, it should be kept in mind that underlying psychosocial factors may also be effective in the disease. Patients with IBS may benefit from a holistic approach to treatment, including mental health and psychosomatic conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Drossman DA. Functional gastrointestinal disorders: history, pathophysiology, clinical features and Rome IV. Gastroenterology. 2016;150:S 0016-5085(16)00223-7. (doi: 10.1053/j.gastro.2016.02.032) 27144617 · doi ↗ · pubmed ↗
- 2Ikechi R Fischer BD De Sipio J Phadtare S. Irritable bowel syndrome: clinical manifestations, dietary influences, and management. Healthcare (Basel). 2017;5(2):21. (doi: 10.3390/healthcare 5020021) PMC 549202428445436 · doi ↗ · pubmed ↗
- 3Hungin APS Chang L Locke GR Dennis EH Barghout V. Irritable bowel syndrome in the United States: prevalence, symptom patterns and impact. Aliment Pharmacol Ther. 2005;21(11):1365 1375. (doi: 10.1111/j.1365-2036.2005.02463.x) 15932367 · doi ↗ · pubmed ↗
- 4Grover M Drossman DA. Centrally acting therapies for irritable bowel syndrome. Gastroenterol Clin North Am. 2011;40(1):183 206. (doi: 10.1016/j.gtc.2010.12.003) 21333907 · doi ↗ · pubmed ↗
- 5Nellesen D Yee K Chawla A Lewis BE Carson RT. A systematic review of the economic and humanistic burden of illness in irritable bowel syndrome and chronic constipation. J Manag Care Pharm. 2013;19(9):755 764. (doi: 10.18553/jmcp.2013.19.9.755) 24156644 PMC 10437427 · doi ↗ · pubmed ↗
- 6Gralnek IM Hays RD Kilbourne A Naliboff B Mayer EA. The impact of irritable bowel syndrome on health-related quality of life. Gastroenterology. 2000;119(3):654 660. (doi: 10.1053/gast.2000.16484) 10982758 · doi ↗ · pubmed ↗
- 7Huang KY Wang FY Lv M Ma XX Tang XD Lv L. Irritable bowel syndrome: epidemiology, overlap disorders, pathophysiology and treatment. World J Gastroenterol. 2023;29(26):4120-4135. (doi: 10.3748/wjg.v 29.i 26.4120) PMC 1035457137475846 · doi ↗ · pubmed ↗
- 8Li Y Wang Z Zhang S Hua Y Fan X Li L. mi R-539-5p regulates irritable bowel syndrome pathological processes by targeting KDM 6A. Turk J Gastroenterol. 2025 [Epub ahead of print]. (doi: 10.5152/tjg.2025.24684) PMC 1282489040955148 · doi ↗ · pubmed ↗