Rescue Therapy for Impacted Large Chicken Bone in the Esophagus: Argon Plasma Coagulation–Assisted Endoscopic Removal – A Case Report
Muhammet Yener Akpinar, Hasan Sahin, Tolga Bakir, Mustafa Gulsen

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1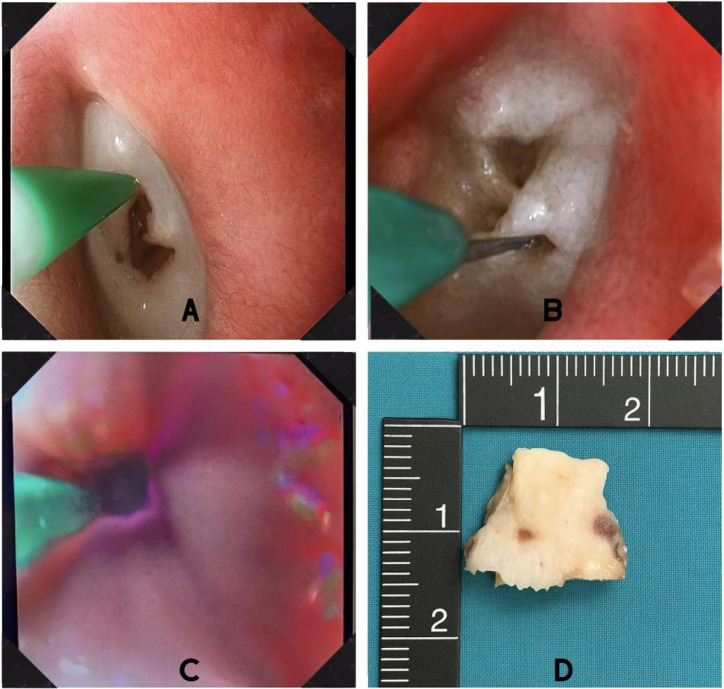 Figure 2
Figure 2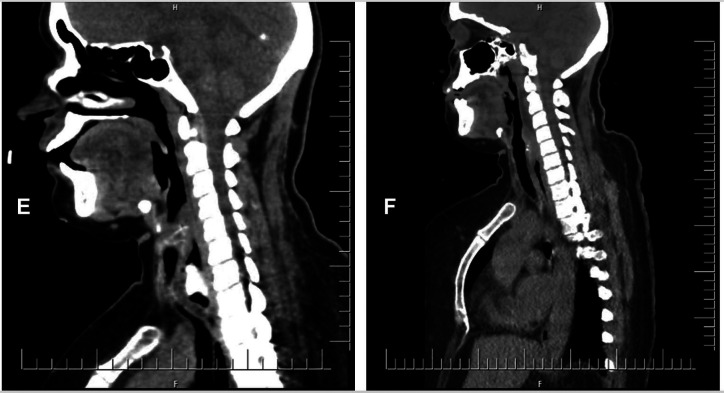 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Foreign Body Medical Cases · Hemostasis and retained surgical items
Dear Editor,
A 46-year-old female with no history of systemic or psychosocial issues presented with a complaint of foreign body sensation in her throat after drinking chicken soup. The informed consent was obtained. She denied prior episodes of foreign body ingestion or any relevant family history. She reported pain and a feeling of obstruction while swallowing. Physical examination and laboratory tests were unremarkable except for leukocytosis (14.7 × 10^9^/L) and an elevated C-reactive protein (CRP) level (19 mg/L).
Neck computed tomography (CT) revealed a dense foreign body measuring 21 × 11 mm within the upper esophageal lumen, causing near-complete luminal obstruction. Due to the detection of complete blockage and suspicion of mediastinitis, initial evaluation included consultations with infectious disease, general surgery, and thoracic surgery departments. Empiric antibiotherapy was initiated, and an endoscopic approach was preferred. During the initial endoscopic evaluation, a chicken bone approximately 2 cm in diameter was identified in the proximal esophagus. Following the complete obstruction and the rigid, potentially lacerating nature of the foreign body, attempts at removal using a snare, balloon, and standard forceps were unsuccessful. The patient was closely monitored in the intensive care unit and underwent a second endoscopic procedure under general anesthesia. As part of the rescue therapy, an initial attempt was made to create access using a needle-knife sphincterotome, but this was unsuccessful because of the hardness and position of the foreign body. Subsequently, a second rescue technique was employed using an argon plasma coagulation (APC) probe (KLS MARTIN ME 411) set to 60 watts. Two linear tunnels were created on the surface of the bone, facilitating better instrument engagement. These grooves enabled secure grasping with alligator-jaw forceps, and the foreign body was successfully extracted without complication, as shown in Figure 1.
Follow-up CT revealed no signs of complications other than a localized collection thought to be secondary to trauma, as seen in Figure 2. The case was clinically stable, and she was discharged. At the one-month follow-up endoscopy, no significant pathology was observed, the patient recovered fully, and no long-term complications were expected.
In line with the European Society of Gastrointestinal Endoscopy guidelines,1 computed tomography was utilized to assess potential complications, surgical consultation was obtained prior to the innovative endoscopic approach, and urgent endoscopic intervention was preferred as a result of complete obstruction by a sharp foreign body.
Argon plasma coagulation is used in various procedures such as the removal of embedded stents, ablation of granulation tissue around metal stents, control of bleeding after sphincterotomy, debulking of periampullary tumors, coagulation of superficial mucosal lesions, and endoscopic hemostasis.2 Similar to previously reported cases involving difficult foreign body extraction, such as the entangled plastic wires described by Park et al,3 our case also required the use of multiple endoscopic tools in a non-standard fashion. In Park’s case, APC was used to damage the food material surrounding plastic wires, indirectly weakening the structure. Benatta et al^4^ described the use of APC and polypectomy snare to fragment and remove a gastric trichobezoar in a pediatric patient, avoiding surgery. A recent case by Abadia et al5 demonstrated successful removal of an impacted garlic clove in the esophagus using a similar APC-based tunneling technique, followed by Fogarty balloon extraction. Our approach parallels this strategy but differs in target material (bone vs. vegetable) and retrieval method (forceps vs. balloon), underscoring the adaptability of APC-assisted tunneling in managing complete esophageal obstructions. All aforementioned cases highlight the potential of adapting endoscopic techniques beyond their conventional use, especially in complex scenarios where traditional methods fail. To the best of our knowledge, this is the first case describing APC-assisted tunneling for complete esophageal obstruction by a chicken bone. This report is limited by being a single case with a relatively short follow-up period. Also, the delayed intervention may have influenced the outcome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Birk M Bauerfeind P Deprez PH Removal of foreign bodies in the upper gastrointestinal tract in adults: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2016;48(5):489 496. (doi: 10.1055/s-0042-100456) 26862844 · doi ↗ · pubmed ↗
- 2Sumiyama K Kaise M Kato M New generation argon plasma coagulation in flexible endoscopy: ex vivo study and clinical experience. J Gastroenterol Hepatol. 2006;21(7):1122 1128. (doi: 10.1111/j.1440-1746.2005.04133.x) 16824063 · doi ↗ · pubmed ↗
- 3Park CK Kim HD Kim JY Endoscopic removal of tangled plastic wires in the stomach using an argon plasma coagulation and endoscopic scissors. Korean J Helicobacter Up Gastrointest Res. 2015;15(2):124 126. (doi: 10.7704/kjhugr.2015.15.2.124) · doi ↗
- 4Benatta MA. Endoscopic retrieval of gastric trichobezoar after fragmentation with electrocautery using polypectomy snare and argon plasma coagulation in a pediatric patient. Gastroenterol Rep (Oxf). 2016;4(3):251 253. (doi: 10.1093/gastro/gov 013) 25877378 PMC 4976679 · doi ↗ · pubmed ↗
- 5Abu-Suboh Abadia M Dot Bach J Masachs Peracaula M Armengol MiróJ Armengol MiróJR. Extraction of esophageal foreign body with burrowing technique. Gastrointest Endosc. 2016;84(1):174. (doi: 10.1016/j.gie.2016.02.037) 26965741 · doi ↗ · pubmed ↗