Angiotensin-Converting Enzyme (ACE) Inhibitor-Associated Hypersensitivity Vasculitis With Small Bowel Edema: A Case Report
Lamyae Debbagh, Marc Zalcman

TL;DR
An 84-year-old man developed abdominal pain and skin symptoms from an ACE inhibitor, which improved after stopping the drug.
Contribution
This case report highlights a rare ACE inhibitor side effect involving the small bowel and skin vasculitis.
Findings
ACE inhibitor use was linked to small bowel edema and cutaneous purpura.
Discontinuation of lisinopril led to rapid symptom resolution.
CT imaging showed bowel wall thickening without mesenteric ischemia.
Abstract
Angiotensin-converting enzyme (ACE) inhibitor-associated hypersensitivity vasculitis with gastrointestinal involvement is an uncommon but important drug-related cause of acute abdominal pain and may mimic an acute surgical abdomen. We report the case of an 84-year-old man admitted for redo aortic valve replacement following infective endocarditis, who developed acute abdominal pain on postoperative day 14. Physical examination revealed diffuse abdominal tenderness and cutaneous purpura. Laboratory testing showed elevated inflammatory markers with peripheral eosinophilia. Contrast-enhanced abdominal CT demonstrated concentric small bowel wall thickening with submucosal edema and ascites, without evidence of mesenteric ischemia. Skin biopsy confirmed leukocytoclastic vasculitis. Lisinopril was initiated at the time of admission and continued throughout the perioperative period; symptoms…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
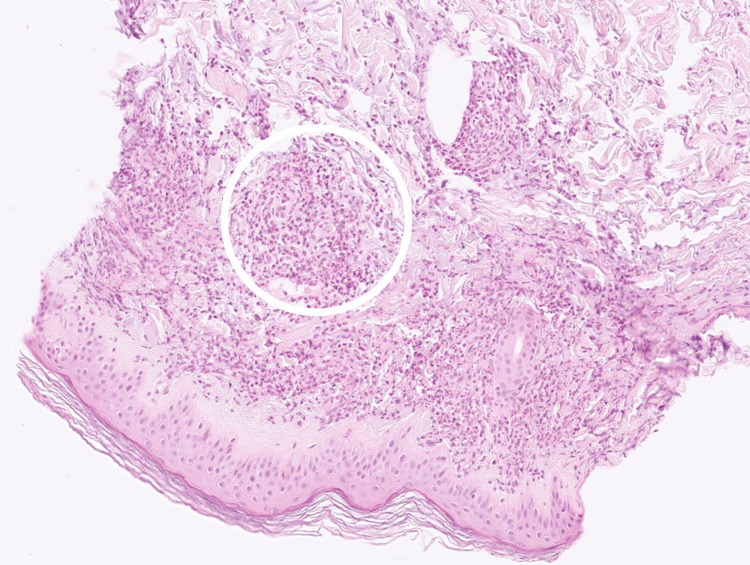 Figure 1
Figure 1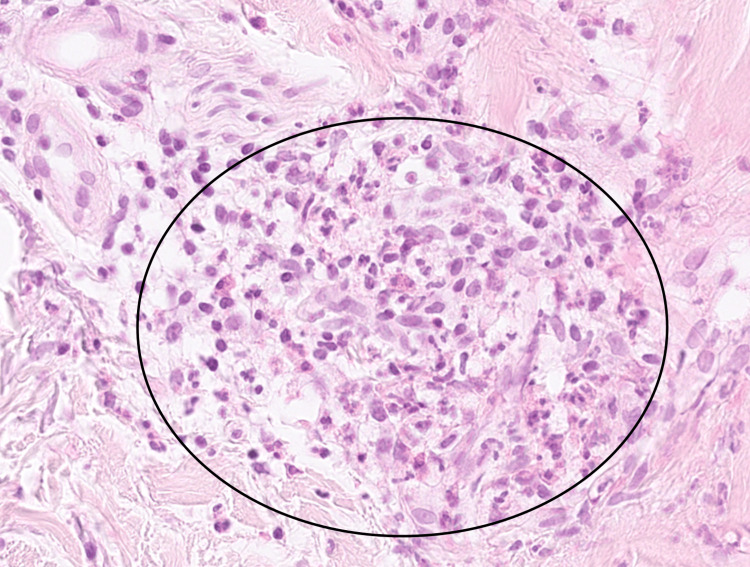 Figure 2
Figure 2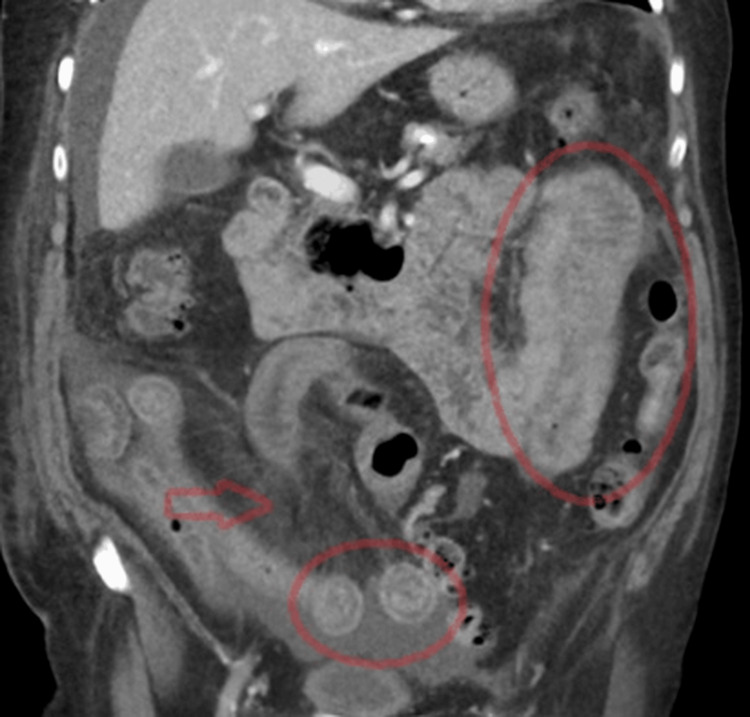 Figure 3
Figure 3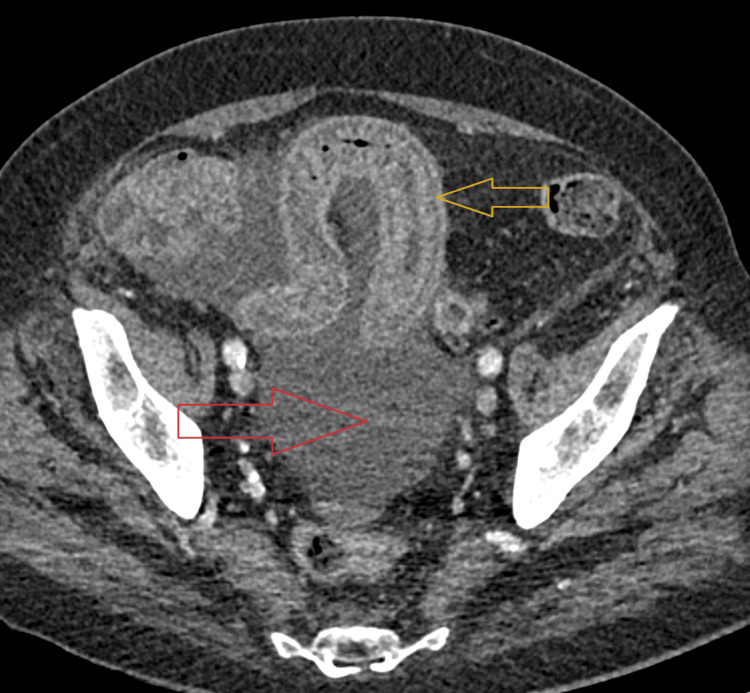 Figure 4
Figure 4| Parameter | Result | Reference range |
| C-reactive protein (CRP) | 88 mg/L | <5 mg/L |
| White blood cells | 12,000 /µL | 4,000-10,000 /µL |
| LDH (current) | 389 U/L | 135-225 U/L |
| LDH (previous) | 447 U/L | 135-225 U/L |
| Eosinophils | Elevated | <0.5 × 10⁹/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDrug-Induced Adverse Reactions · Vasculitis and related conditions · Eosinophilic Disorders and Syndromes
Introduction
Angiotensin-converting enzyme inhibitors (ACEIs) are widely prescribed for the treatment of hypertension, heart failure, and cardiovascular protection. Angioedema is a well-recognized adverse effect, usually involving the lips, tongue, or airway, and occurs in approximately 0.1-0.7% of patients receiving ACEIs [1,2]. Visceral involvement is a much rarer manifestation, first described in the 1980s, and remains underdiagnosed due to its nonspecific symptoms and delayed onset after drug initiation [3,4]. Patients typically present with acute abdominal pain, nausea, vomiting, or diarrhea, often mimicking mesenteric ischemia, inflammatory bowel disease, or intestinal obstruction [5-7]. Imaging, particularly contrast-enhanced CT, plays a crucial role in diagnosis, showing segmental bowel wall thickening, submucosal edema, and ascites [8,9]. Although ACEI-related bowel edema is classically attributed to bradykinin-mediated mechanisms, ACEIs may also rarely be associated with immune-mediated hypersensitivity reactions, including leukocytoclastic vasculitis, which may involve the gastrointestinal tract and produce overlapping imaging findings. Rapid resolution of symptoms following discontinuation of the ACEI strongly supports the diagnosis [6,10]. Awareness of this entity is essential, as misdiagnosis may lead to unnecessary surgical interventions. We report a case of lisinopril-associated leukocytoclastic vasculitis with gastrointestinal involvement presenting with small bowel edema, highlighting diagnostic challenges and the importance of careful medication review in elderly postoperative patients with acute abdominal pain.
Case presentation
An 84-year-old man with a history of aortic valve replacement in 2011 and a permanent pacemaker was admitted for redo aortic valve surgery following infective endocarditis. His immediate postoperative course was uneventful until day 14, when he developed severe intermittent abdominal pain rated 7/10 on the visual analogue scale. The pain was associated with nausea and vomiting but occurred in the absence of fever, diarrhea, or constipation. On clinical examination, the patient presented with diffuse abdominal tenderness and guarding. In addition, a progressive purpuric rash appeared on the wrists and arms and extended to the upper trunk during hospitalization. Vital signs remained stable throughout the episode. Laboratory investigations demonstrated elevated inflammatory and hematological parameters, as summarized in Table 1.
Histopathological analysis of the skin biopsy confirmed the presence of neutrophilic leukocytoclastic vasculitis involving dermal vessels (Figures 1-2).
Histopathology of skin biopsy.Hematoxylin and eosin stain, skin biopsy, ×10 magnification. The specimen shows features of leukocytoclastic vasculitis characterized by dense neutrophilic infiltration of dermal vessels with perivascular inflammation; one representative affected area is highlighted by a white circle.
Histopathology of skin biopsy at high magnification.Hematoxylin and eosin stain, skin biopsy, ×40 magnification. The image demonstrates leukocytoclastic vasculitis with prominent neutrophilic infiltration and perivascular inflammatory changes (black circle).
Urgent contrast-enhanced abdominal CT demonstrated a long segment of concentric small bowel wall thickening associated with submucosal edema, stratified mural enhancement, and the mesenteric comb sign. While the mesenteric comb sign and stratified mural enhancement are not specific and can be observed in inflammatory bowel disease or enteritis, the concurrent systemic findings in our patient (purpura, eosinophilia, and skin biopsy-confirmed leukocytoclastic vasculitis) supported the diagnosis of an immune-mediated hypersensitivity vasculitis with gastrointestinal involvement, which may produce CT findings similar to intestinal angioedema. Moderate ascites was also present, while no signs of mesenteric ischemia or mechanical obstruction were identified (Figures 3-4).
Coronal contrast-enhanced CT images showing concentric small bowel wall thickening with submucosal edema and stratified enhancement of the small bowel loops (red ellipses) with mesenteric comb sign (red arrow).
Axial contrast-enhanced CT image of the pelvis showing marked bowel wall edema (yellow arrow) with ascites (red arrow).
Based on the clinical and radiological findings, the internal medicine team suspected lisinopril-induced hypersensitivity vasculitis with intestinal involvement. Discontinuation of lisinopril resulted in the rapid resolution of abdominal symptoms and complete clinical recovery.
Discussion
ACE inhibitor-related gastrointestinal involvement is uncommon but clinically important, as it may present with acute abdominal pain and imaging findings suggestive of an acute surgical abdomen. Visceral edema associated with ACE inhibitors is classically attributed to bradykinin accumulation, resulting in increased vascular permeability and submucosal bowel edema [1,2]. Clinically, patients typically present with nonspecific symptoms such as abdominal pain, nausea, vomiting, and, in some cases, diarrhea. Because of this nonspecific presentation, the condition is frequently misdiagnosed as mesenteric ischemia, inflammatory bowel disease, or intestinal lymphoma [3-6].
However, ACE inhibitors may also rarely trigger immune-mediated hypersensitivity reactions, including leukocytoclastic vasculitis, which can involve the gastrointestinal tract and lead to similar clinical and radiological presentations. In our patient, the presence of purpura, peripheral eosinophilia, and biopsy-proven leukocytoclastic vasculitis strongly supported an immune-complex hypersensitivity vasculitis with gastrointestinal involvement rather than isolated bradykinin-mediated intestinal angioedema.
Radiological imaging, particularly contrast-enhanced abdominal CT, plays a key role in the diagnostic workup. Typical findings include segmental concentric bowel wall thickening, prominent submucosal edema with stratified mural enhancement, and variable amounts of ascites, usually without evidence of vascular occlusion or bowel ischemia [7,8]. Nevertheless, these CT features are not specific and may also be observed in inflammatory enteritis or vasculitis, making correlation with clinical and laboratory findings essential [3-6]. Recognition of this entity remains important to avoid unnecessary exploratory surgery, and rapid clinical improvement following ACEI discontinuation strongly supports a drug-related mechanism [4,6,9].
Although a drug rechallenge was not performed for safety reasons, the temporal relationship with lisinopril initiation and the rapid resolution after treatment discontinuation further supported the suspected diagnosis. This case highlights the value of careful medication review and recognition of associated systemic features in elderly postoperative patients presenting with acute abdominal pain, in order to prevent unnecessary invasive investigations and surgical exploration.
Conclusions
For this patient, although a rechallenge was not performed for safety reasons, the suspected diagnosis of lisinopril-associated hypersensitivity vasculitis with gastrointestinal involvement was supported by the temporal relationship with treatment initiation, purpura with biopsy-proven leukocytoclastic vasculitis, compatible CT findings of small bowel edema, and rapid improvement after drug discontinuation. This case illustrates that in elderly postoperative patients presenting with acute abdominal pain, drug-induced hypersensitivity reactions should be considered before pursuing invasive procedures. It also highlights the value of careful medication review and radiological assessment in preventing unnecessary interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1ACE inhibitor-induced angioedema of the intestine: case report, incidence, pathophysiology, diagnosis and management Can J Gastroenterol Oudit G Girgrah N Allard J 8278321520011177394910.1155/2001/247816 · doi ↗ · pubmed ↗
- 2ACE inhibitor-induced angioedema J Allergy Clin Immunol Pract Baram M Kommuri A Sellers SA Cohn JR 442445120132456561410.1016/j.jaip.2013.07.005 · doi ↗ · pubmed ↗
- 3Patients' perspective on full disclosure and informed consent regarding postoperative visual loss associated with spinal surgery in the prone position Mayo Clin Proc Corda DM Dexter F Pasternak JJ Trentman TL Nottmeier EW Brull SJ 8658688620112187859810.4065/mcp.2011.0279 PMC 3258003 · doi ↗ · pubmed ↗
- 4Angioedema of the bowel with ACE inhibitors: case report and systematic review Am J Gastroenterol Kotlyar D Hirten R Pasamba M 071052010 https://journals.lww.com/ajg/fulltext/2010/10001/angioedema_of_the_bowel_with_ace_inhibitors__a.985.aspx
- 5ACE inhibitor induced visceral angioedema: an elusive diagnosis BMJ Case Rep Sravanthi MV Suma Kumaran S Sharma N Milekic B 913202010.1136/bcr-2020-236391 PMC 768465033229477 · doi ↗ · pubmed ↗
- 6ACE inhibitor-induced angioedema of the small bowel: a case report and review of the literature J Pharm Pract Wilin KL Czupryn MJ Mui R Renno A Murphy JA 991033120182812592210.1177/0897190017690641 · doi ↗ · pubmed ↗
- 7ACE inhibitor-induced angioedema of the bowel Case Rep Med Campbell T Peckler B Hackstadt RD Payor A 510201010.1155/2010/690695 PMC 301483221209819 · doi ↗ · pubmed ↗
- 8Small bowel angioedema secondary to ACE inhibitor Am J Gastroenterol Barnett J Yu KK Mayilvaganan B 01192024