Definition and Determination of the Correct Tibial Entry Portal With Accuracy in Intramedullary Nailing of Tibial Fractures
Rishabh Saxena, Ashwani Mathur, Nakul Fauzdar, Neel Agarwal, Shataayu Gugale, Shreyansh Gupta, Manasvi Bagree

TL;DR
This study identifies the correct tibial entry portal for intramedullary nailing to improve alignment and outcomes in tibial fracture surgery.
Contribution
The study prospectively evaluates the optimal tibial entry portal for intramedullary nailing in tibial shaft fractures.
Findings
Coronal and sagittal malalignments were linked to entry portal positioning.
Low complication rates were observed, with delayed union and infection each occurring in 3.1% of cases.
Abstract
Background Tibial shaft fractures, frequently caused by high-energy trauma, significantly challenge orthopedic trauma management. Intramedullary interlocking nailing, favored for its biomechanical advantages and reduced complications, critically depends on accurately identifying the tibial entry portal to ensure optimal alignment and functional outcomes. Methodology A prospective observational study was designed to evaluate the optimal tibial entry portal for improving alignment outcomes in patients undergoing intramedullary nailing (IMN) for tibial shaft fractures. Conducted at Mahatma Gandhi Medical College and Hospital, Jaipur, the study included 32 adult patients with tibial fractures suitable for IMN. Radiological outcomes and alignment accuracy were assessed at nine-month follow-ups. Results Participants had a mean age of 44.63±18.17 years; men predominated (18, 56.3%). The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
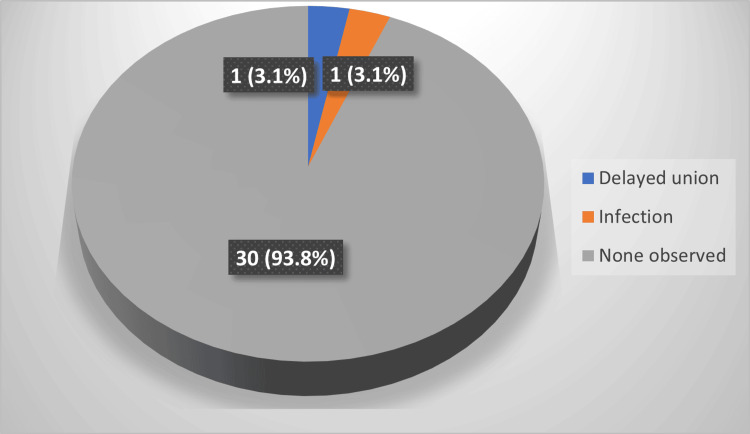 Figure 1
Figure 1| Variables | Frequency (n=32) | Percentage (%) |
| Age Group | ||
| <30 years | 10 | 31.2% |
| 30-45 years | 6 | 18.8% |
| 46-60 years | 7 | 21.9% |
| >60 years | 9 | 28.1% |
| Gender | ||
| Male | 18 | 56.3% |
| Female | 14 | 43.8% |
| Mode of Injury | ||
| Road traffic accident | 18 | 56.3% |
| Fall from height | 14 | 43.8% |
| Fracture Type | ||
| Closed | 20 | 62.5% |
| Open Type I | 1 | 3.1% |
| Open Type II | 6 | 18.8% |
| Open Type III-A | 4 | 12.5% |
| Open Type III-B | 1 | 3.1% |
| AO Classification | ||
| 42 A | 11 | 34.4% |
| 42 B | 9 | 28.1% |
| 42 C | 10 | 31.3% |
| Others | 2 | 6.2% |
| Grade | Coronal Plane | Sagittal Plane |
| 0 | 6 (18.8%) | 5 (15.6%) |
| 1 | 7 (21.9%) | 7 (21.9%) |
| 2 | 8 (25.0%) | 6 (18.8%) |
| 3 | 5 (15.6%) | 8 (25.0%) |
| 4 | 6 (18.8%) | 6 (18.8%) |
| Total | 32 (100.0%) | 32 (100.0%) |
| Variable | N | Minimum | Maximum | Mean ± SD |
| Knee range of motion (ROM) | 32 | 110 | 145 | 127.03±8.786 |
| Lysholm Knee Scoring Scale | 32 | 63 | 100 | 90.41±7.754 |
| Lower Extremity Functional Scale (LEFS) | 32 | 36 | 80 | 69.63±9.486 |
| Time of union | 32 | 4 | 9 | 4.84±1.221 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone fractures and treatments · Total Knee Arthroplasty Outcomes · Reconstructive Surgery and Microvascular Techniques
Introduction
Tibial shaft fractures are prevalent orthopedic injuries, particularly due to high-energy trauma such as road traffic accidents [1]. The standard treatment is reamed intramedullary interlocking nailing, which allows for biological fixation and early mobilization. However, the success of this procedure heavily depends on accurate placement of the tibial entry point, which influences post-operative alignment and functional outcomes [2,3]. Malalignment can result from improper entry point placement, particularly due to the tibia’s unique anatomy and muscle forces acting on fractured segments. Despite technological advancements, reliance on anatomical landmarks and fluoroscopy for entry point determination introduces variability, leading to angular deformities and inconsistent outcomes [4]. Studies show that misalignment of more than five degrees adversely affects function and increases joint degeneration risk. Yet, literature remains inconsistent regarding the ideal entry point, and most studies are retrospective or based on cadaver models. This study aims to prospectively investigate the correlation between tibial entry point and post-operative alignment in cases managed with reamed intramedullary nailing.
Materials and methods
A prospective observational clinical study was conducted in the Department of Orthopaedics, Mahatma Gandhi Medical College and Hospital, Jaipur, over a period of 18 months. Ethical approval was obtained from the Institutional Ethics Committee of the institution (approval number: IEC/1475). The study adhered to the principles of the Indian Council of Medical Research (ICMR) Guidelines (2017) and the Declaration of Helsinki (2004). Written informed consent was taken from all participants.
Study population
All patients admitted with tibial shaft fractures during the study period were screened. Eligible participants were recruited using systematic random sampling.
Inclusion Criteria
The study included adult patients aged 18 years and above presenting with tibial shaft fractures deemed appropriate for intramedullary nailing. Both closed fractures and open fractures classified as Gustilo-Anderson Type I and Type II were eligible for participation.
Exclusion Criteria
Patients were excluded if they had any previous history of tibial shaft fracture or presented with open fractures of Gustilo-Anderson Type III or higher grades. Individuals with a narrow medullary canal, significant tibial deformity, or any radiological or clinical evidence of active joint sepsis were also excluded due to the potential of compromising surgical access, fixation accuracy, or postoperative outcomes.
Data collection
Data were recorded on a semi-structured proforma. Demographic and clinical details included age, sex, occupation, mode of injury, fracture type, associated injuries, and time to intervention. Socioeconomic status was assessed using the modified BG Prasad classification (2022) [5].
Clinical evaluation involved detailed history, examination, and fracture classification (Arbeitsgemeinschaft für Osteosynthesefragen (AO) and Gustilo-Anderson). Radiological assessment comprised anteroposterior and lateral radiographs for pre- and post-operative alignment [6,7].
The Lower Extremity Functional Scale (LEFS) evaluates the functional limitations in lower extremity conditions [8]. The Lysholm Knee Scoring Scale, originally developed by Lysholm and Gillquist and later refined by Tegner and Lysholm [9], was used.
Data management and confidentiality
Data were entered into Microsoft Excel (Microsoft, Redmond, WA) and analyzed using SPSS version 21.0 (IBM Corp, Armonk, NY). Confidentiality was maintained through anonymization and password-protected data storage.
Statistical analysis
Continuous variables were expressed as mean±standard deviation (SD). Categorical variables as frequency and percentage. Chi-square test (χ²) applied for categorical normal distributed data. Student’s t-test used for continuous variable and p<0.05 was considered statistically significant.
Results
This study analyzed 32 patients with tibial shaft fractures, focusing on demographic variables, mechanism of injury, fracture types, classifications, malalignment patterns, surgical approaches, postoperative complications, and functional outcomes.
The age of the patients ranged from 20 to 76 years, with a mean age of 44.63 years. The most common age group was those younger than 30 years (31.2%), followed by those older than 60 years (28.1%). Gender distribution showed a male predominance with 18 patients (56.3%) compared to 14 women (43.8%). The most frequent cause of injury was road traffic accidents (56.3%), while falls from height accounted for 43.8% of cases. Closed fractures were the majority (62.5%). Among open fractures, type II was most common (18.8%), followed by type III-A (12.5%). According to the Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association (AO/OTA) classification system, type 42 A fractures were the most frequent (34.4%), followed by 42 C (31.3%) and 42 B (28.1%) (Table 1).
Malalignment distribution
Postoperative radiographs demonstrated coronal plane malalignment most frequently at grade 2 (8, 25.0%), while sagittal plane malalignment was most commonly grade 3 (8, 25.0%). Overall, 11 (34.4%) of patients showed grade ≥3 malalignment in coronal plane and 14 (43.8%) in sagittal plane, indicating clinically significant deformity (Table 2).
Figure 1 shows that postoperative complications were minimal: 30 (93.8%) patients had uneventful recovery, while one case each of delayed union and infection was reported (1, 3.1% each). Surgical approaches were equally distributed, with 16 (50%) patients undergoing the suprapatellar approach and 16 (50%) patients treated with the infrapatellar approach.
Post-operative Complications
Functional outcomes and union
Table 3 shows functional outcomes were favourable when the mean postoperative knee range of motion was 127.03°±8.79. The Lysholm Knee Scoring Scale yielded a mean of 90.41±7.75, indicating good knee function, while the LEFS averaged 69.63±9.49, reflecting satisfactory lower limb function. The mean time to radiological union was 4.84±1.22 months.
Discussion
Our findings align with existing literature indicating higher male predominance and a bimodal age distribution in tibial fractures managed via intramedullary nailing (IMN). The substantial incidence of malalignment emphasizes the critical role of entry portal selection [10]. Comparative analysis revealed the merits of both approaches, highlighting that precision in entry-point localization significantly impacts final alignment outcomes [11,12]. Also, previous cadaveric and clinical studies support thorough preoperative and intraoperative planning [13,14].
A series of studies has highlighted the clinical utility and outcomes of intramedullary interlocking nailing in tibial fractures. Favorable functional recovery has been documented in extra-articular distal tibia fractures treated with tibial interlocking nails [15], and good results have also been reported with dynamic interlock nailing in distal fractures [16]. Reamed interlocking nails have proven effective in managing diaphyseal fractures and aseptic nonunions.
The study comprised 32 patients, with a male predominance (56.3%) similar to findings by Liu et al. (2020) [17]. The mean age was 44.63 years, reflecting a bimodal distribution, suggesting the procedure’s applicability across a wide age spectrum. Similar age-related trends were observed in study by Yadav et al. (2025) [18], though others like Khalil et al. (2020) [19] reported younger cohorts.
Road-traffic accidents (56.3%) were the most common mechanism of injury, followed closely by falls from height (43.8%). The side of the fracture was nearly equally distributed, with a slight right-sided dominance. Most fractures were closed (62.5%), in alignment with findings by Liu et al. (2020) [17]. AO classification showed a balanced distribution among simple, wedge, and complex fractures, with a slight predominance of Type 42A.
Both suprapatellar and infrapatellar approaches were equally employed. While traditional studies favored infrapatellar access, recent evidence, including that from Yadav et al. (2025) [18], supports the rising preference for suprapatellar techniques due to improved alignment outcomes.
The correct tibial entry point continues to be debated, with anatomical localization emphasized in earlier literature [18] and safe surgical techniques elaborated upon in subsequent reports [19]. Technique-related refinements, such as suprapatellar and proximal tibia entry methods, have been further explored, underscoring the importance of fracture level and technical variation [20,21]. Complications remain relevant, with tibial malrotation [22] and anterior knee pain associated with radiological factors [22] being significant concerns. Additionally, the role of fibular integrity in facilitating fracture healing has been established [23], while the efficacy of intramedullary nails as primary fixation in compound tibial fractures has also been demonstrated [24,25].
Radiological alignment outcomes were excellent, with 100% achieving acceptable coronal alignment and no sagittal malalignment >5°. The complication rate was low (6.2%), with only isolated cases of delayed union and infection. Functional outcomes, as assessed by Lysholm and LEFS scores, indicated favorable recovery, corroborated by comparable studies. The average time to union was approximately 4.84 months, aligning with existing literature reported by Gadegone et al. (2015) [25] and Patel et al. (2024) [21].
Limitations
The small sample size (n=32) limit the generalizability of findings. Radiographic alignment was measured using plain radiographs; more advanced imaging techniques like CT scans could have provided greater precision in detecting malrotation. This being a single-centric study in a tertiary-care center limits the generalizability of the findings to a broader population.
Conclusions
Accurate selection and localization of the tibial entry portal play a decisive role in achieving optimal alignment during intramedullary nailing of tibial fractures. Intramedullary nailing remains a reliable and effective method for managing tibial shaft fractures, yielding good radiological and functional outcomes with low complication rates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology of adult fractures: a review Injury Court-Brown CM Caesar B 6916973720061681478710.1016/j.injury.2006.04.130 · doi ↗ · pubmed ↗
- 2Semiextended position of intramedullary nailing of the proximal tibia Clin Orthop Relat Res Tornetta P 3rd Collins E 185189199610.1097/00003086-199607000-000298653954 · doi ↗ · pubmed ↗
- 3Radiographic and clinical comparisons of distal tibia shaft fractures (4 to 11 cm proximal to the plafond): plating versus intramedullary nailing J Orthop Trauma Vallier HA Le TT Bedi A 3073112220081844898310.1097/BOT.0b 013e 31816 ed 974 · doi ↗ · pubmed ↗
- 4Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures J Bone Joint Surg Am Bhandari M Guyatt G Tornetta P 3rd Schemitsch EH Swiontkowski M Sanders D Walter SD 256725789020081904770110.2106/JBJS.G.01694 PMC 2663330 · doi ↗ · pubmed ↗
- 5Socioeconomic status scales: Revised Kuppuswamy, BG Prasad, and Udai Pareekh's scale updated for 2021 J Family Med Prim Care Majumder S 396439671020213513675310.4103/jfmpc.jfmpc_600_21PMC 8797108 · doi ↗ · pubmed ↗
- 6Fracture and dislocation classification compendium - 2018 J Orthop Trauma Meinberg EG Agel J Roberts CS Karam MD Kellam JF 032201810.1097/BOT.000000000000106329256945 · doi ↗ · pubmed ↗
- 7Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses J Bone Joint Surg Am Gustilo RB Anderson JT 453458581976 https://pubmed.ncbi.nlm.nih.gov/773941/773941 · pubmed ↗
- 8North American Orthopaedic Rehabilitation Research Network. The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application Phys Ther Binkley JM Stratford PW Lott SA Riddle DL 371383791999 https://pubmed.ncbi.nlm.nih.gov/10201543/10201543 · pubmed ↗