Severe and profound hearing loss in patients with multiple sensory impairments: increased incidence of cognitive impairment
Jacob C. Lucas, Alexandra M. Arambula, Katherine Yu, Linda D’Silva, Jennifer A. Villwock, Hinrich Staecker

TL;DR
People with severe hearing loss and other sensory issues are more likely to have cognitive problems, suggesting the need for broader screening.
Contribution
This study shows that combined sensory dysfunction, especially severe hearing loss, significantly increases the risk of cognitive impairment.
Findings
Combined sensory dysfunction significantly increases the odds of cognitive impairment.
Severe and profound hearing loss is associated with higher odds of cognitive impairment compared to milder hearing loss.
Patients with dysfunction in all tested sensory domains had the highest risk of cognitive impairment.
Abstract
•Combined sensory dysfunction increased the odds of cognitive impairment.•More severe hearing loss increased the likelihood of cognitive impairment.•Patients with hearing loss should be screened for other sensory disorders. Combined sensory dysfunction increased the odds of cognitive impairment. More severe hearing loss increased the likelihood of cognitive impairment. Patients with hearing loss should be screened for other sensory disorders. Determine odds of incident cognitive impairment among patients with severe to profound hearing loss and co-existing multisensory impairment. 14 prospectively recruited aging (age 50+) patients with severe and profound hearing loss were pooled for analysis with 180 previously enrolled patients with demonstrated multisensory impairment. Patients were recruited as part of a cross-sectional case-control study at a tertiary care…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
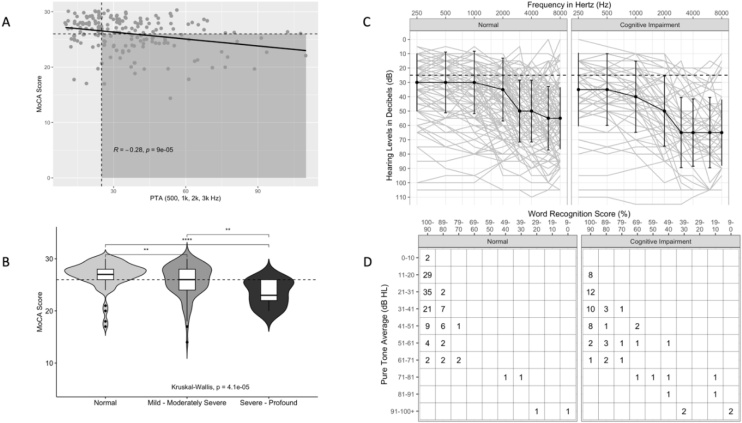 Figure 1
Figure 1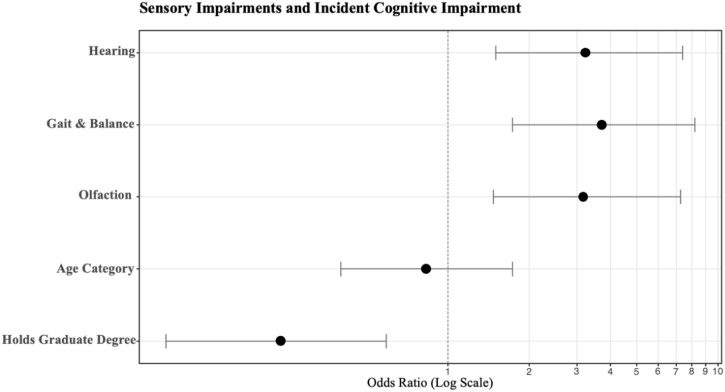 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOlfactory and Sensory Function Studies · Vestibular and auditory disorders · Hearing, Cochlea, Tinnitus, Genetics
Introduction
Cognitive Impairment (CoI) and dementia have been repeatedly linked to Sensorineural Hearing Loss (SNHL).1, 2, 3 Impairment of other sensory domains such as olfaction and vestibular function are also strongly linked to cognition deficits.4, 5, 6, 7, 8 A recent prospectively recruited case-control study examined the interplay between loss of hearing, balance, and olfaction; patients with deficits in these domains were more likely to present with a worse cognitive screening score on the Montreal Cognitive Assessment (MoCA).9 Additionally, deficits were additive: patients with impairment in more than one domain had an increased odds of having incident CoI. One weakness of that study was a lack of enrolled patients with severe and profound hearing loss. The resultant data was under-powered to stratify odds of CoI by hearing loss severity. Recent population studies have suggested that not only the severity of hearing loss but also the quality of rehabilitation affects dementia risk.10^,^11
Due to this, an additional cohort of patients was recruited from a population of patients undergoing evaluation for Cochlear Implantation (CI), to specifically target patients with severe and profound SNHL. 14 additional patients with severe or profound SNHL were recruited, consented, and pooled for analysis with the previously enrolled 180 patients. We determined the following research question: Among a prospectively recruited cohort of patients with variable deficits in hearing, balance, and olfaction, does worse hearing equate to an increased Odds Ratio (OR) of CoI on the MoCA screening instrument? The hypothesis was that patients with Multisensory Impairment (MSI) and severe or profound hearing loss would have a higher proportion of CoI compared to patients with either normal hearing or hearing in the mild-moderately severe range.
Methods
Patients
A previously described cohort of 180 patients was recruited from February 2021 through June 2021 and included “aging” above 50-years-old. Patients presenting with a chief complaint of “hearing loss” were eligible.9 Exclusion criteria were patients younger than 50, progressive Central Nervous System (CNS) disease, nonambulatory, unable to follow written or verbal instructions due to cognition or language barriers, conductive hearing loss, tympanic membrane perforation, hearing loss due to vestibular schwannoma, and recent COVID-19. An additional 14 patients meeting inclusion and exclusion criteria, and with documented severe or profound SNHL were recruiting during a period spanning from September 2021 through January 2021. A total of 194 patients were pooled for statistical analysis and stratified based on severity of SNHL.
Interventions
All study-related activities were conducted with local Institutional Review Board approval. The 14 patients with severe-profound hearing loss were recruited while undergoing evaluation for possible cochlear implantation. This population was targeted due to the high rate of severe and profound sensorineural hearing loss present.
Hearing
Hearing was evaluated based on the ANSI/AS S3.21-2004, and thresholds were recorded at 0.25, 0.5, 1, 2, 3, 4, 6, and 8 kilohertz (kHz).12^,^13 Pure-tone averages were calculated using 0.5, 1, 2, and 3 (or an average of 2 and 4 when unavailable) kHz as recommended by the AAO-HNS.14^,^15 Word recognition scores were recorded. Air conduction levels were used.
Balance
Point of care balance and gait testing was performed using the Timed ‘Up & Go’ (TUG) instrument,16^,^12 a timed measure of gait and coordinated standing which has been previously validated in elderly populations and patients with vestibular disorders, with up to an 80 percent sensitivity in determining fall risk in these populations.17^,^18 The test is easy for research personnel to administer and acts as a proxy for both peripheral and central vestibular function, as it requires visual, proprioceptive, and vestibular inputs to perform the coordinated task. Testing for specific vestibular end-organ disease processes was not a goal of the present study, so the TUG was an easy and proven instrument to bimodally stratify patients into “impaired” and “unimpaired” balance categories based on a cutoff score of 11 seconds for the task.
Olfaction
The Affordable, Rapid, Olfactory Measurement Array (AROMA) test is an essential oil-based instrument for characterizing degree of olfactory impairment, with validation among patients with cognitive impairment, dementia, and Alzheimer’s disease19^,^20 which has strong association with olfactory impairment.21 A full accounting of the olfactory testing methodology is available in previous works.9 AROMA was utilized to stratify patients into impaired and unimpaired olfaction categories based on patient responses to 14 scents at 4 consecutive increasing concentrations.
Main outcome measures
The Montreal Cognitive Assessment (MoCA) has been shown to detect mild cognitive impairment at a higher sensitivity than the Mini Mental Status Examination (MMSE) and tests multiple domains of cognition including working memory, visuospatial abstraction, and recall.22^,^23 A modification for the Hearing Impaired (HI), the HI-MoCA, provides written rather than spoken instructions to prevent the hearing impairment itself from contributing to the cognition score.24 HI-MoCA was used in the assessment of patients with severe and profound hearing loss. A score of 26 (out of 30) was used as the cutoff for CoI. A correction for education level of 1 point was added for patients who did not complete high school.
Statistical analysis
Data analysis was performed using the R statistical computing program in RStudio25; with the Tidyverse suite of packages used for data wrangling and transformation.26 The ggplot2.27 and audiometry28 packages were used to generate visualizations of the data. Univariate analysis was performed on demographic and predictor variables to evaluate their effect on the outcome variable – cognitive status. Wilcoxon Rank Sum, Pearson’s Chi-Squared, and Fisher’s exact test were used for univariate testing. Cognitive status was classified as a binary outcome; MoCA scores 26 or greater were considered normal and scores less than 26 were considered CoI. Due to this, binary logistic regression was used for multivariate analysis, using a stepwise selection procedure for variables. Odds Ratios (OR) with Confidence Intervals (CI) were calculated for predictor variables.
Results
A total of 194 patients were included; 180 were enrolled during the initial study period, with an additional 14 individuals with severe or profound hearing loss recruited for the present study and pooled for analysis. The recruitment and testing protocols were identical for both groups. Demographic and univariate analysis of predictor variables are reported in Table 1. Of the enrolled subjects, 66 screened positive for CoI as defined by MoCA score <26. All sensory domains were individually significant contributors toward an increased odds of incident CoI. Education was also a significant predictor toward higher scores on the screening instrument and was therefore included in multivariate analysis.Table 1. Univariate analysis for demographic and predictor variable inputs.Table 1. CharacteristicNormal (n = 128)^a^CI (n = 66)ap-valuebAge at Enrollment66 (59, 72)69 (63, 75)0.094Age Category0.5 50‒6553 (41%)24 (36%) 65+75 (59%)42 (64%)Sex0.3 Female69 (54%)30 (45%) Male59 (46%)36 (55%)Education Level<0.001 Completed College49 (38%)19 (29%) Completed High School37 (29%)38 (58%) Completed Graduate/ Professional Degree39 (30%)7 (11%) Did not complete High School3 (2.3%)2 (3.0%)Timed Up-and-Go9.1 (8.1, 10.5)10.4 (8.8, 13.9)0.001PTA (500, 1k, 2k, 3k Hz)29 (21, 40)39 (27, 52)<0.001AROMA Score75 (66, 84)66 (54, 73)<0.001Gait Status<0.001 Normal Gait107 (84%)36 (55%) Gait Impairment21 (16%)30 (45%)Hearing Status<0.001 Normal Hearing58 (45%)12 (18%) SNHL70 (55%)54 (82%)Hearing Severity<0.001 Normal58 (45%)12 (18%) Mild ‒ Moderately Severe66 (52%)45 (68%) Severe ‒ Profound4 (3.1%)9 (14%)Olfactory Status<0.001 Normal Olfaction60 (47%)11 (17%) Hyposmia68 (53%)55 (83%)Number of Sensory Losses<0.001 0 or 177 (60%)13 (20%) 241 (32%)31 (47%) 310 (7.8%)22 (33%)aMedian (IQR); n (%).bWilcoxon rank sum test; Pearson's Chi-Squared test; Fisher's exact test.
Hearing results are visualized in Fig. 1. Aggregation of the audiometric data (Fig. 1a) shows a negative correlation between MoCA score and PTA (R = -0.28, p < 0.001). Fig. 1b shows a clear difference between “Normal”, “Mild-Moderately Severe”, and “Severe-Profound” hearing groups; as hearing worsens, the average MoCA score within groups trends downward. Composite audiograms are shown in Fig. 1c for the Normal and CoI comparison groups. The AAO-HNS recommended reporting of hearing outcomes with PTA/WRS scattergram is shown in Fig. 1d.Fig. 1. An aggregation of audiometry and hearing data for normal and CoI subjects. (A) PTA is presented on the x-axis with response variable MoCA score on the y-axis. Shaded area bounded by cutoff scores for normal MoCA (26) and normal PTA (<25 dB HL). Solid line represents best fit for Pearson Correlation; R and p-values are listed. (B) Violin boxplots are presented for 3 hearing categories: “Normal”, “Mild-Moderately Severe”, and “Severe-Profound. Dashed line is MoCA cutoff for normal. * p < 0.05; ** p < 0.01; *** p < 0.001; **** p < 0.0001. (C) Composite audiograms for Normal and CoI data, solid dark line is the median for each threshold, error bars correspond to 1 standard deviation. (D) AAO-HNS minimum reporting standards for raw data of PTA plotted against Word Recognition Scores (WRS).10Fig. 1
Multivariate analysis is summarized in Table 2 and visualized in Fig. 2 as a plot of the Odds Ratios with Confidence Intervals. Each individual sensory deficit was found in the model to contribute to an increased odds of incident CoI (ORs = 3.17, 3.71, and 3.23 for olfactory, gait, and SNHL respectively). Sensory deficits were additive; impairment in all 3 domains was most likely to have CoI (OR = 15.2, 95% CI [5.66, 44.2], p < 0.001) compared to 2 domains (OR = 5.09, 95% CI [2.36, 11.6], p < 0.001).Table 2. Binary Logistic Regression performed and listed by sensory impairment. Hearing is represented with 3 stratified groups based on severity of hearing. Worse hearing equates to a higher odds of incident CoI. Education had a protective effect on classification as CoI.Table 2. CharacteristicOR95% CIp-valueHearing Severity Normal‒‒ Mild ‒ Moderately Severe2.811.28, 6.530.012 Severe ‒ Profound8.322.11, 38.20.004Gait & Balance Normal Gait‒‒ Gait Impairment3.571.65, 7.930.001Olfaction Normal Olfaction‒‒ Hyposmia3.311.51, 7.720.004Age Category 50 ‒ 65‒‒ 65+0.900.43, 1.910.8Holds Graduate Degree No Graduate Degree‒‒ Graduate Degree0.250.09, 0.620.005OR, Odds Ratio; CI, Confidence Interval.Fig. 2. Odds Ratios for each sensory domain visualized. When hearing is represented as a binary outcome (Normal or SNHL), the odds of an incident CoI is 3.23.Fig. 2
When stratifying hearing status within cognitive outcomes, severe and profound SNHL were most likely to occur alongside CoI (OR = 8.32, 95% CI [2.11, 38.2], p < 0.001) compared to mild – moderately severe HL (OR = 2.81, 95% CI [1.28, 6.53], p < 0.001).
Discussion
Impairment of multiple sensory domains seems to increase the likelihood of a co-existing cognitive deficit, at least when screening with the MoCA instrument. More interesting, in the present study, poorer hearing seems to correlate with a worse MoCA score. A worsening risk of cognitive impairment was also demonstrated in a large cohort of insurance data.10 Combination of balance dysfunction with visual loss has also been demonstrated to increase the risk of cognitive impairment.29 A number of hypotheses have been proposed to explain the link between sensory system disturbance and cognitive impairment including depletion of cognitive reserve, direct effects and loss of social interaction.30 Having multiple impairments could affect any of these potential mechanisms making comprehensive evaluation of our patients of paramount importance. The findings here underscore the groundwork laid in our previous work and address the under-powering of our previous study to demonstrate a relationship between worsening hearing and cognitive status. The findings here also add to the growing body of research linking hearing loss in the elderly with increased lifetime risk of dementia. The Lancet Commission has identified hearing loss as the most important modifiable risk factor for dementia.31 Since recent studies demonstrate cochlear implantation gives a greater improvement in dementia risk compared to amplification,11^,^32 rigorous assessment of the severity of hearing loss is an important component of patient care.
Despite these findings, the study is not without limitation. There is likely a component of selection bias; only a small percentage of recruited individuals consented to participate, and those could possibly have skewed towards having a pre-existing cognitive deficit. Our MoCA score cutoff likely over-estimates true cognitive impairment and is not sufficient alone for the diagnosis of dementia. Similarly, dedicated vestibular testing might have yielded more specific insights into the contribution of the peripheral vestibular system compared to the TUG instrument. However, the testing in this study was chosen for convenience and in the hopes of yielding some insight into cognition and its complex relationship with peripheral multi-sensory inputs. These sensory losses, especially hearing, are ripe targets for rehabilitative efforts. Future studies will attempt to alter the disease course of dementia by addressing these sensory deficits early on. The patients in this study were recruited based on complaints of hearing loss. With sensorineural hearing loss being the most common neurodegenerative disorder in man, the current study suggests that we should also screen patients who present for isolated sensory complaints for other areas of dysfunction since there is increasing evidence that rehabilitation of sensory deficits can mitigate the risk of cognitive decline.
Conclusion
Impairment of multiple senses increases the risk of having an abnormal MoCA score. The risk of an abnormal MoCA score, and thereby higher risk of dementia is increased with worsening hearing loss.
ORCID ID
Jacob C. Lucas: 0000-0002-5441-6576
Alexandra M. Arambula: 0000-0002-5624-3613
Katherine Yu: 0000-0002-2867-5291
Jennifer A. Villwock: 0000-0001-5645-4210
Disclosures
JAV discloses intellectual property and a filed patent (17/281121 – “Olfactory Diagnostic and Training Kits and Methods”) related to the objective olfactory testing methods used in this research.
Data availability statement
The authors declare that all data are available in repository.
Declaration of competing interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lin F.R.Thorpe R.Gordon-Salant S.Ferrucci L.Hearing loss prevalence and risk factors among older adults in the United States J Gerontol A Biol Sci Med Sci.66A 201158259010.1093/gerona/glr 002PMC 307495821357188 · doi ↗ · pubmed ↗
- 2Lin F.R.Metter E.J.O’Brien R.J.Resnick S.M.Zonderman A.B.Ferrucci L.Hearing loss and incident dementia Arch Neurol.6820112142202132098810.1001/archneurol.2010.362PMC 3277836 · doi ↗ · pubmed ↗
- 3Lin F.R.Yaffe K.Xia J.Hearing loss and cognitive decline in older adults JAMA Intern Med.17320132932333797810.1001/jamainternmed.2013.1868 PMC 3869227 · doi ↗ · pubmed ↗
- 4Fischer M.E.Cruickshanks K.J.Schubert C.R.Age‐related sensory impairments and risk of cognitive impairment J Am Geriatr Soc.642016198119872761184510.1111/jgs.14308 PMC 5073029 · doi ↗ · pubmed ↗
- 5Schubert C.R.Cruickshanks K.J.Fischer M.E.Sensorineural impairments, cardiovascular risk factors, and 10-year incidence of cognitive impairment and decline in midlife: the Beaver dam offspring study J Gerontol A Biol Sci Med Sci.742019178617923062913210.1093/gerona/glz 011PMC 6777086 · doi ↗ · pubmed ↗
- 6Agrawal Y.Smith P.F.Rosenberg P.B.Vestibular impairment, cognitive decline and Alzheimer’s disease: balancing the evidence Aging Ment Health.2420207057083069129510.1080/13607863.2019.1566813 PMC 6663651 · doi ↗ · pubmed ↗
- 7Kim H.J.Jeong S.Oh Y.H.Suh M.J.Suh J.Y.Association of balance impairment with risk of incident dementia among older adults J Prev Alzheimers Dis.1120241301373823072510.14283/jpad.2023.79 · doi ↗ · pubmed ↗
- 8Shrestha S.Zhu X.Kucharska‐Newton A.M.Characterizing the olfaction and dementia association in the community‐based ARIC study Alzheimers Dement.212025 e 1461310.1002/alz.14613 PMC 1184798239988999 · doi ↗ · pubmed ↗