Exploring the core symptoms and influencing factors of fatigue-related symptom clusters in patients with HIV/AIDS
Dan Xu, Jianghui Zhang, Lan Shen, Haowen Chen, Jia Li

TL;DR
This study identifies key fatigue-related symptoms and factors in HIV/AIDS patients, highlighting sleep issues as central for targeted management.
Contribution
The study identifies gender-specific core symptoms and influencing factors in fatigue-related symptom clusters among HIV/AIDS patients.
Findings
Sleep disturbances and fatigue are prevalent in both male and female HIV/AIDS patients.
Partner’s HIV status and ART duration significantly influence fatigue-related symptoms.
Sexual dysfunction and daytime functioning are central in female symptom networks.
Abstract
To explore the core symptoms and associated factors of fatigue-related symptom clusters in people living with HIV/AIDS during follow-up, with the aim of informing precision-based symptom management strategies. Fatigue-related symptom clusters in patients with HIV/AIDS were assessed using the Fatigue Self-Assessment Scale, the Pittsburgh Sleep Quality Index, the Sexual Dysfunction Scale, and the Groningen Frailty Indicator. Symptom networks were constructed using R software to identify central symptoms based on network metrics. Univariate analysis and multivariate linear regression were then performed to explore potential factors associated with these core symptoms. Among male patients living with HIV/AIDS, the three most prevalent symptoms within the fatigue-related symptom cluster were fatigue (86.32%), sleep disturbances (44.63%), and weakness (43.32%). In female patients, the top…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
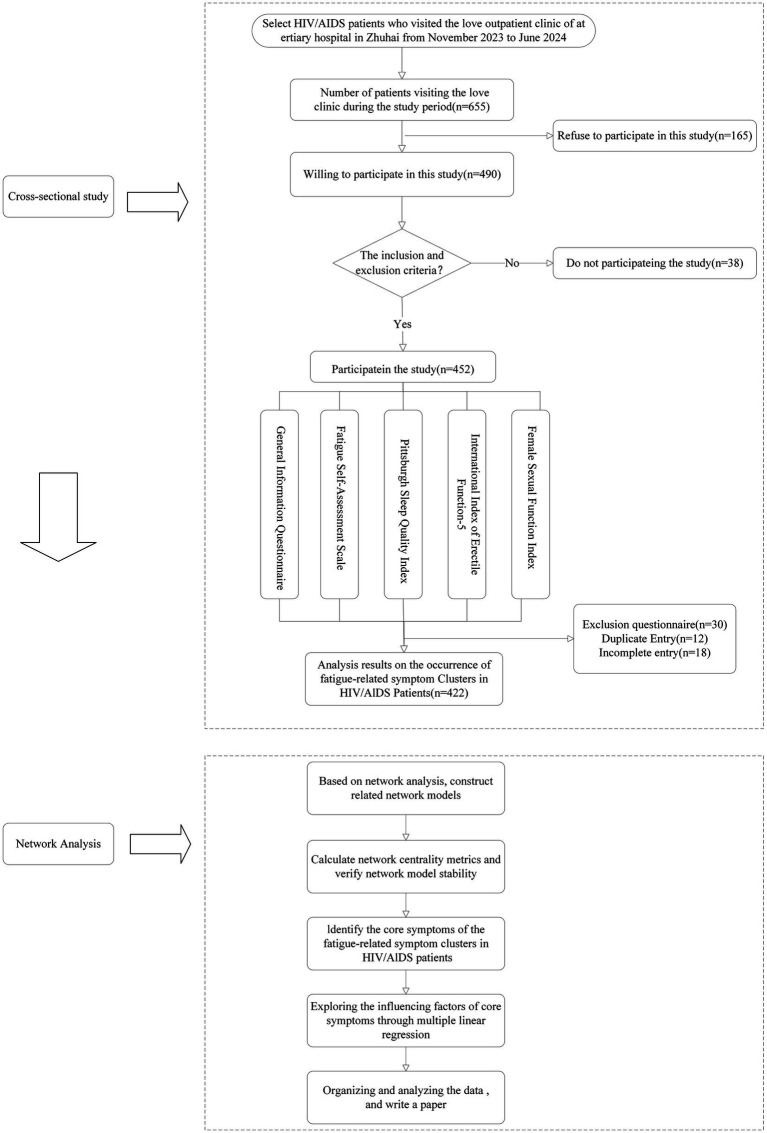 Figure 1
Figure 1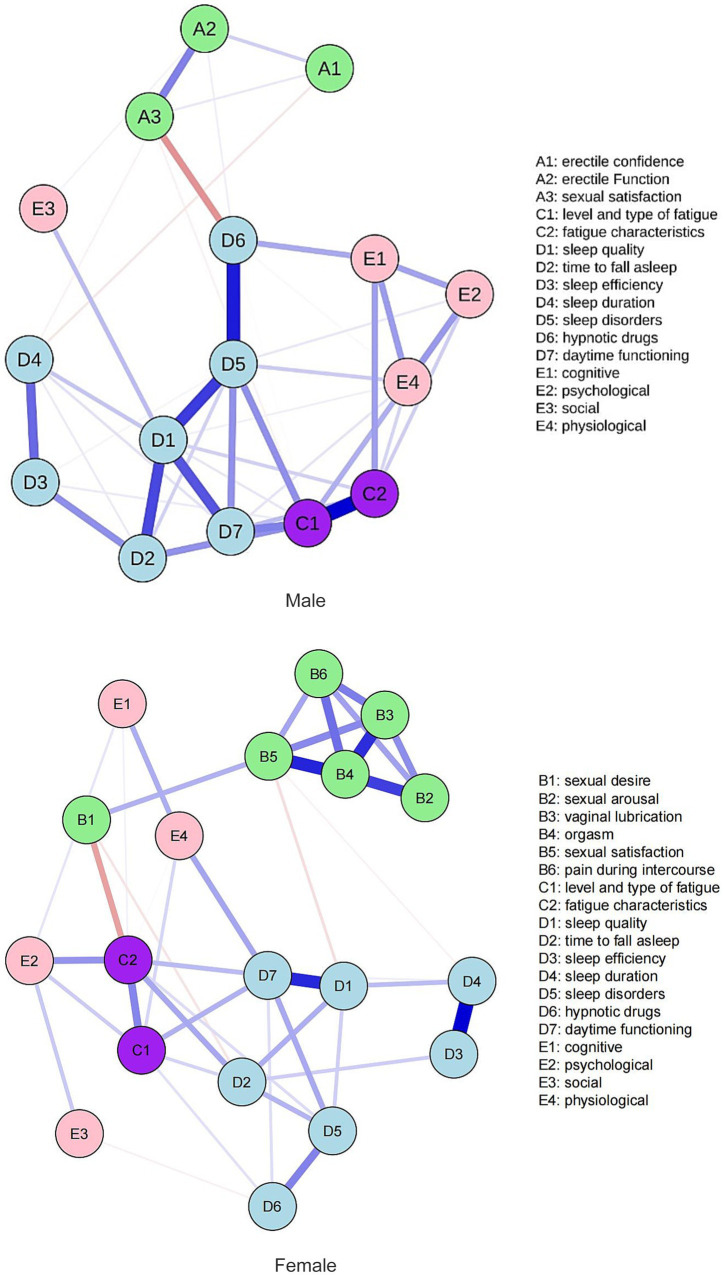 Figure 2
Figure 2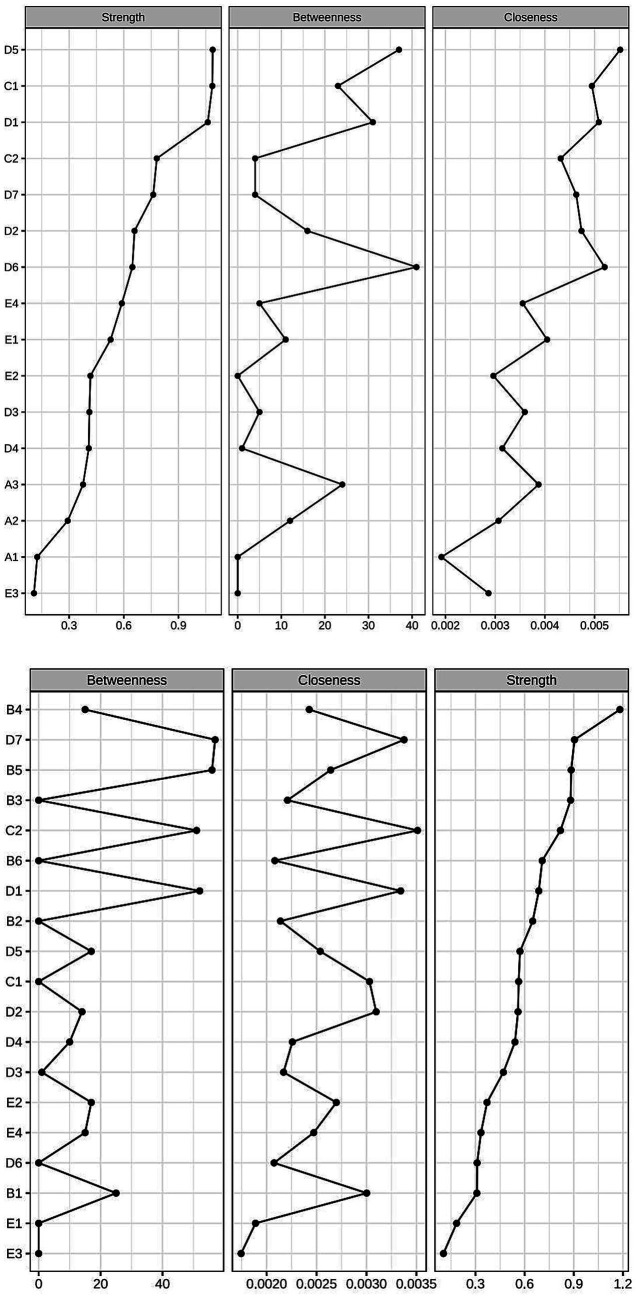 Figure 3
Figure 3| Item | Category | Frequency | Percentage (%) |
|---|---|---|---|
| Gender | Male | 307 | 72.75 |
| Female | 115 | 27.25 | |
| Ethnicity | Han | 383 | 90.76 |
| Minorities | 39 | 9.24 | |
| Marital status | Single | 209 | 49.53 |
| Married | 164 | 38.86 | |
| Otherwise | 49 | 11.61 | |
| Partner’s HIV status | Yes | 97 | 22.99 |
| No | 325 | 77.01 | |
| Sexual orientation | Heterosexual | 271 | 64.22 |
| Homosexual | 117 | 27.72 | |
| Bisexual | 34 | 8.06 | |
| Number of sexual partners | 0 | 33 | 7.82 |
| 1 | 309 | 73.22 | |
| ≥2 | 80 | 18.96 | |
| Number of children | 0 | 172 | 40.76 |
| 1 | 107 | 25.35 | |
| ≥2 | 143 | 33.89 | |
| Living arrangement | Living alone | 193 | 39.96 |
| Spouse | 126 | 26.09 | |
| Children | 86 | 17.81 | |
| Parents | 43 | 8.91 | |
| Otherwise | 35 | 7.25 | |
| BMI | Underweight | 46 | 10.90 |
| Normal weight | 265 | 62.80 | |
| Overweight | 94 | 22.27 | |
| Obesity | 17 | 4.03 |
| Item | Category | Frequency | Percentage (%) |
|---|---|---|---|
| Education level | No formal education | 9 | 2.13 |
| Lower secondary education or below | 240 | 56.87 | |
| Lower secondary education or above | 173 | 41.00 | |
| Place of residence | Owner-occupied housing | 176 | 41.71 |
| Rented housing | 202 | 47.87 | |
| Other | 44 | 10.42 | |
| Economic income | <1,000 RMB | 86 | 20.38 |
| 1,000–3,000 RMB | 70 | 16.59 | |
| 3,000–5,000 RMB | 144 | 34.12 | |
| ≥5,000 RMB | 122 | 28.91 | |
| Employment status | Unemployed | 81 | 19.19 |
| Temporary or short-term employment | 69 | 16.35 | |
| Permanent or long-term stable employment | 239 | 56.64 | |
| Agricultural employment | 14 | 3.32 | |
| Retired | 19 | 4.50 | |
| Health insurance coverage | Local health insurance | 281 | 66.59 |
| No-Local health insurance | 100 | 23.70 | |
| Other insurance | 9 | 2.13 | |
| Uninsured | 32 | 7.58 |
| Item | Category | Frequency | Percentage (%) |
|---|---|---|---|
| Comorbidities | Yes | 28 | 6.64 |
| No | 394 | 93.36 | |
| CD4 + T-cell count | <50 | 12 | 2.84 |
| 50–350 | 106 | 25.13 | |
| 350–500 | 117 | 27.72 | |
| ≥500 | 187 | 44.31 | |
| Years since HIV infection | <1 year | 47 | 11.14 |
| 1–5 years | 183 | 43.36 | |
| 5–10 years | 85 | 20.14 | |
| ≥10 years | 107 | 25.36 | |
| Duration of ART | <1 year | 47 | 11.14 |
| 1–3 years | 102 | 24.17 | |
| 3–5 years | 95 | 22.51 | |
| ≥5 years | 178 | 42.18 | |
| Route of transmission | Heterosexual intercourse | 234 | 55.45 |
| Homosexual intercourse | 143 | 33.89 | |
| Intravenous drug use | 25 | 5.92 | |
| Blood transfusion | 2 | 0.47 | |
| Unknown | 18 | 4.27 |
| Item | Prevalence [ | Score ( |
|---|---|---|
| Fatigue | 265m(86.32) | 20.20 ± 18.14 |
| 84w(73.04) | 19.39 ± 17.61 | |
| Sleep disturbances | 137m(44.63) | 5.65 ± 3.09 |
| 52w(45.22) | 5.65 ± 3.27 | |
| Frailty | 133m(43.32) | 3.25 ± 2.11 |
| 51w(44.35) | 3.36 ± 2.19 | |
| Sexual dysfunction | 110m(35.83) | 21.40 ± 2.30 |
| 83w(72.17) | 17.02 ± 8.54 |
| Variable | Frequency | PSQI |
| |
|---|---|---|---|---|
| Age | 1.73F | 0.18 | ||
| 18–29 | 65 | 5.01 ± 3.27 | ||
| 30–49 | 229 | 5.71 ± 3.11 | ||
| ≥50 | 128 | 5.88 ± 3.08 | ||
| Gender | 0.01t | 0.99 | ||
| Male | 307 | 5.66 ± 3.09 | ||
| Female | 115 | 5.65 ± 3.28 | ||
| Ethnicity | −0.30t | |||
| Han | 383 | 5.67 ± 3.20 | ||
| Minorities | 39 | 5.54 ± 2.44 | ||
| Comorbidities | 1.54t | 0.12 | ||
| Yes | 28 | 6.54 ± 3.90 | ||
| No | 394 | 5.59 ± 3.07 | ||
| Partner’s HIV status | −2.20t | 0.03 | ||
| Yes | 97 | 5.04 ± 2.82 | ||
| No | 325 | 5.83 ± 3.20 | ||
| Education level | 1.63F | 0.20 | ||
| No formal education | 9 | 5.56 ± 2.60 | ||
| Lower secondary education or below | 240 | 5.89 ± 3.24 | ||
| Lower secondary education or above | 173 | 5.33 ± 3.00 | ||
| Marital status | 0.53F | 0.59 | ||
| Single | 209 | 5.57 ± 3.08 | ||
| Married | 164 | 5.63 ± 3.20 | ||
| Other | 49 | 6.08 ± 3.16 | ||
| BMI | 0.51F | 0.67 | ||
| Underweight | 46 | 6.09 ± 3.38 | ||
| Normal weight | 265 | 5.66 ± 3.11 | ||
| Overweight | 94 | 5.39 ± 3.03 | ||
| Obesity | 17 | 5.76 ± 3.51 | ||
| CD4 + T-cell count | 1.61F | 0.19 | ||
| <50 | 12 | 7.00 ± 4.29 | ||
| 50–350 | 106 | 5.88 ± 3.30 | ||
| 350–500 | 117 | 5.80 ± 2.99 | ||
| ≥500 | 187 | 5.35 ± 3.04 | ||
| Living arrangement | 0.96F | 0.38 | ||
| Owner-occupied housing | 176 | 5.77 ± 3.07 | ||
| Rented housing | 202 | 5.68 ± 3.27 | ||
| Other | 44 | 5.05 ± 2.68 | ||
| Years since HIV Infection | 1.97F | 0.12 | ||
| <1 year | 47 | 5.12 ± 2.53 | ||
| 1–5 years | 183 | 5.61 ± 3.22 | ||
| 5–10 years | 85 | 5.34 ± 2.90 | ||
| ≥10 years | 107 | 6.22 ± 3.35 | ||
| Route of transmission | 1.47F | 0.21 | ||
| Heterosexual intercourse | 234 | 5.71 ± 3.08 | ||
| Homosexual intercourse | 143 | 5.43 ± 3.10 | ||
| Intravenous drug use | 25 | 6.00 ± 3.24 | ||
| Blood transfusion | 2 | 10.50 ± 6.36 | ||
| Unknown | 18 | 5.72 ± 3.49 | ||
| Employment Status | 7.74F | |||
| Unemployed | 81 | |||
| Temporary or short-term employment | 69 | 6.53 ± 3.50 | ||
| Permanent or long-term stable employment | 239 | 6.14 ± 3.08 | ||
| Agricultural employment | 14 | 4.99 ± 2.78 | ||
| Retired | 19 | 7.57 ± 3.46 | ||
| Duration of ART | 2.86F | 0.04 | ||
| <1 year | 47 | 4.49 ± 2.23 | ||
| 1–3 years | 102 | 5.57 ± 2.94 | ||
| 3–5 years | 95 | 6.05 ± 3.51 | ||
| ≥5 years | 178 | 5.80 ± 3.18 | ||
| Monthly income (RMB) | 5.11F | 0.002 | ||
| <1,000 | 86 | 6.51 ± 3.63 | ||
| 1,000–3,000 | 70 | 6.17 ± 3.30 | ||
| 3,000–5,000 | 144 | 5.49 ± 3.04 | ||
| ≥5,000 | 122 | 4.95 ± 2.56 | ||
| Number of sexual partners | ||||
| 0 | 33 | 5.61 ± 3.11 | ||
| 1 | 309 | 6.26 ± 3.23 | ||
| ≥2 | 80 | 4.61 ± 2.90 | ||
| Health insurance coverage | 0.89F | 0.45 | ||
| Local health insurance | 281 | 5.60 ± 3.14 | ||
| No-local health insurance | 100 | 5.66 ± 3.24 | ||
| Otherwise | 9 | 4.67 ± 1.58 | ||
| Sexual orientation | 0.28F | 0.76 | ||
| Heterosexual | 271 | 5.70 ± 3.09 | ||
| Homosexual | 117 | 5.49 ± 3.31 | ||
| Bisexual | 34 | 5.88 ± 2.97 | ||
| Variable |
| Beta |
|
|
|---|---|---|---|---|
| (Constant) | 4.49 | 6.26 | ||
| Partner’s HIV status1 | ||||
| Yes | −0.93 | −0.13 | −2.66 | 0.008 |
| Duration of ART2 | ||||
| 1–3 | 1.09 | 0.15 | 2.05 | 0.04 |
| 3–5 | 1.77 | 0.24 | 3.29 | 0.001 |
| ≥5 | 1.27 | 0.50 | 2.55 | 0.01 |
| Number of sexual partners3 | ||||
| 1 | 1.25 | 0.18 | 2.24 | 0.02 |
| ≥2 | 1.92 | 0.24 | 3.04 | 0.003 |
| Monthly income (RMB)4 | ||||
| 1,000–3,000 | −0.10 | −0.01 | −0.18 | 0.85 |
| 3,000–5,000 | −0.03 | −0.01 | −0.09 | 0.93 |
| ≥5,000 | −0.32 | −0.05 | −0.52 | 0.60 |
| Employment status5 | ||||
| Temporary or short-term employment | −0.72 | −0.09 | −1.17 | 0.24 |
| Permanent or long-term stable employment | −1.61 | 0.26 | −2.86 | 0.004 |
| Agricultural employment | 0.98 | 0.89 | 1.11 | 0.27 |
| Retired | 0.46 | 0.03 | 0.59 | 0.55 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · Sleep and related disorders · Bipolar Disorder and Treatment
Introduction
With the widespread implementation and promotion of antiretroviral therapy (ART), HIV infection has shifted from a fatal disease to a manageable chronic condition. The life expectancy of people living with HIV/AIDS is now approaching that of the general, uninfected population. As a result, efforts in HIV/AIDS prevention and control have increasingly focused on reducing the number of new infections and improving the quality of life for those living with the disease (1). In response, the Joint United Nations Programme on HIV/AIDS (UNAIDS) proposed a “fourth 90” target in 2019, building on the original “90–90–90” goals. This additional target aims to ensure that 90% of individuals with viral suppression also achieve a good quality of life (2). However, due to the combined effects of the disease itself, antiretroviral medications, and psychosocial factors, The people living with HIV/AIDS (PLWHA) often experience multiple concurrent symptoms during treatment. These symptoms interact with and influence one another, forming symptom clusters. Compared to isolated symptoms, the synergistic effects within symptom clusters can significantly increase symptom burden. If left unmanaged, they may accelerate the decline in patients’ functional status and quality of life (3).
Studies have identified fatigue, sleep disturbances, weakness, and sexual dysfunction as some of the most distressing and severe symptoms experienced by people living with HIV/AIDS (4, 5). These symptoms often co-occur and collectively form a fatigue-related symptom cluster (4, 6, 7). This cluster has been shown to negatively impact treatment adherence, therapeutic outcomes, and overall quality of life, ultimately contributing to increased mortality in this population (8–11). However, due to the large number of interrelated and interacting symptoms within the cluster, effective intervention remains challenging. The absence of clearly defined therapeutic targets has limited the precision and efficiency of symptom management strategies, thereby undermining the potential advantages of symptom cluster–based interventions.
Network analysis is an analytical approach that explores the complex interrelationships among symptoms by examining attributes such as centrality, accuracy, and stability within a network structure. It enables the identification of core symptoms, bridge symptoms, and other key features (12). By reflecting the interaction mechanisms of symptoms in real-world settings, network analysis provides precise intervention targets and optimizes symptom management strategies, thereby enhancing the efficiency and accuracy of clinical interventions (13). Accordingly, this study investigates the current status of fatigue-related symptom clusters among people living with HIV/AIDS and employs network analysis to identify core symptoms and their influencing factors. The ultimate goal is to provide a foundation for developing personalized and targeted symptom management strategies.
Materials and methods
Ethics approval
This study was approved (or granted exemption) by the ethics committee of The Fifth Affiliated Hospital of Zunyi Medical University (approval no. [2023]2023KY014). We certify that the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Source of study subjects and sampling methods
Using convenience sampling HIV/AlDS patients who visited the Love Clinic of a tertiary hospital in Zhuhai from November 2023 to June 2024were selected. The study design flow chart is provided in Figure 1.
Then study design flow chart.
Study participants
This study employed a convenience sampling method to conduct a cross-sectional survey of HIV/AIDS patients attending the Love Clinic at a tertiary general hospital in Zhuhai, China, between November 2023 and June 2024. Inclusion criteria: (1) Diagnosed as HIV-positive; (2) Aged ≥18 years; (3) Clear consciousness and the ability to communicate and read normally; (4) Signed informed consent and voluntarily participated in the study. Exclusion criteria: (1) Presence of severe HIV-related neurocognitive disorders or other major physical illnesses; (2) History of chronic conditions such as diabetes, hypertension, or coronary heart disease; (3) Participation in other HIV/AIDS-related research studies.
Sample size calculation
Currently, there is no consensus on the sample size calculation method for network analysis, and this remains an area for future research. The prevailing approach is to assess the reliability of network analysis results through post-hoc stability testing (14). Using the Kendall rough sampling principle (15) (which suggests that the sample size should be 5–10 times the number of predictor variables), we estimate the minimum sample size for this study, which involves 23 variables from the scales, to be between 115 and 230 participants. Considering a 20% attrition rate, the final sample size was determined to be 276 participants. Stability testing was then conducted to assess the reliability of the network analysis results. This study was approved by the Ethics Committee of the hospital where the research was conducted ([2023]2023KY014).
Survey instruments
General information questionnaire
A self-designed questionnaire was used to collect general demographic, socio-economic, and disease-related data from HIV/AIDS patients. Demographic data: Age, gender, number of children, household composition, marital status, height, weight, sexual orientation, ethnicity, and HIV status of sexual partners. Socio-economic data: Income level, education level, marital status, employment status, and residence. Disease-related data: ART status, duration of ART treatment, presence of comorbidities, CD4 + T lymphocyte count, duration of HIV infection, and mode of transmission. Disease-related data were extracted by the investigator from follow-up records.
Fatigue self-assessment scale
The Fatigue Self-Assessment Scale (FSAS) consists of two dimensions: fatigue type and severity, and fatigue characteristics, with a total of 23 items (16). Items 1–22 are rated on a 5-point scale, ranging from 0 to 4 points. The standard score for fatigue type and severity ranges from 0 to 100, with higher scores indicating more severe fatigue. The severity levels are categorized into four levels: negligible, mild, moderate, and severe. The fatigue characteristics score also ranges from 0 to 100, with higher scores indicating more prominent fatigue characteristics. The severity levels are categorized into five levels: negligible, slight, moderate, marked, and very marked. FSAS has been validated and shown to possess good reliability and validity (17), and it can be used to assess fatigue type, severity, and characteristics in individuals aged 18 years and older across various disease populations.
Pittsburgh sleep quality index
The Pittsburgh Sleep Quality Index (PSQI) is primarily used to assess the sleep quality of participants over the past month. It consists of seven dimensions: sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleep medications, and daytime dysfunction, with a total of 19 self-reported items and 5 items rated by others (18). The 19th self-reported item and the 5 items rated by others are not included in the scoring. The total score ranges from 0 to 21, with a score greater than 5 indicating poor sleep quality. PSQI has been validated and demonstrated to have good internal consistency and reliability (19).
International index of erectile Function-5
The International Index of Erectile Function-5 is a tool used to assess erectile function, consisting of three dimensions: erectile confidence, erectile function, and sexual satisfaction (20). The scale includes 5 items, each rated from 0 to 5 points. The total score ranges from 0 to 25, with scores less than 7 indicating severe erectile dysfunction, scores between 8 and 11 indicating moderate erectile dysfunction, scores between 12 and 21 indicating mild erectile dysfunction, and scores greater than 21 indicating normal erectile function (21).
Female sexual function index
The Female Sexual Function Index (FSFI) is a scale used to assess female sexual function, consisting of six dimensions: sexual desire, sexual arousal, vaginal lubrication, orgasm, sexual satisfaction, and pain during intercourse. It includes a total of 19 items, with scores ranging from 0 to 5 or 1 to 5 for each item. The total score can range up to 36 points, with a score below 23.45 indicating the presence of sexual dysfunction (22). Chinese scholar Sun Xiaoguang translated and validated the scale, confirming its good reliability and validity (23).
Groningen frailty Indicator
The Groningen Frailty Indicator (GFI) consists of four dimensions: physical, cognitive, social, and psychological, with a total of 15 items. Each item is scored on a 0–1 scale, and a score of ≥4 points indicates frailty (24). In 2022, Huang Yun zhi and colleagues translated and adapted the GFI into a Chinese version, which was validated to have good reliability and validity. This scale is suitable for use as a self-assessment tool in frailty evaluation studies within populations (25).
Data collection
Data were collected using paper-based questionnaires, administered by two trained nursing researchers. These researchers explained the purpose and significance of the study to the participants using standardized instructions. After obtaining informed consent, participants were asked to complete the questionnaire based on their personal circumstances. The questionnaires were to be filled out on-site. For illiterate participants, the investigators assisted by reading the questions and recording the answers through a question-and-answer format. Once completed, the questionnaires were immediately collected and checked. Any incomplete or unclear responses were addressed by communicating with the participants on-site.
Statistical methods
Descriptive analysis
Data were entered and analyzed using EpiData 3.1 software with double-entry by two researchers. The occurrence of symptoms and the associated influencing factors of core symptoms in the fatigue-related symptom cluster of HIV/AIDS patients were analyzed. Normally distributed continuous data are presented as mean ± standard deviation (X̅ ± S), with comparisons between two groups made using the t-test and comparisons among multiple groups made using analysis of variance (ANOVA). Non-normally distributed data are presented as median and interquartile range. Categorical data are presented as frequency and percentage. Demographic, socio-economic, and disease-related data were analyzed for their impact on core symptoms using chi-square tests and one-way ANOVA, with a p < 0.05 considered statistically significant. Multivariate linear regression analysis was used to examine the impact of demographic, socio-economic, and disease-related factors on core symptoms, with a p < 0.05 considered statistically significant.
Network analysis
R software (version 4.3.0) was used for network analysis of the cross-sectional data. Using the EBICglasso function (26), symptom network structures for fatigue-related symptom clusters in male and female HIV/AIDS patients were constructed based on Spearman’s rank correlation. Each dimension of the scales served as a node, with edges representing the correlations between nodes. The thickness of the edges indicates the strength of the correlation, with thicker edges representing stronger correlations. The correlation between edges is referred to as edge weight (27). The CentralityPlot function was used to generate centrality measures, including strength (rs), closeness centrality (rc), and betweenness centrality (rb), to evaluate the importance, proximity, and potential of symptoms as bridging symptoms within the network. Strength reflects the importance of a node in the network, calculated as the sum of the absolute edge weights between the node and all other nodes. Nodes with greater strength contribute more significantly to the network structure and play a role in promoting the overall development of the network. Closeness centrality measures how close a node is to all other nodes, calculated by the inverse of the sum of distances between nodes. A higher value indicates that the symptom is closer to others and more likely to be at the center of the network. Betweenness centrality assesses the potential for a node to act as a bridge within the network, measured by counting the number of shortest paths between any two nodes that pass through the node. A higher value suggests that the symptom is more likely to be a bridging symptom (28). Bootstrapping analysis was performed using the Corstability function, with 1,000 non-parametric resampling tests to assess network stability. A stability coefficient greater than 0.25 indicates an acceptable network model stability, and a coefficient greater than or equal to 0.5 indicates good stability (14).
Results
A total of 452 questionnaires were distributed in this study. Among them, 12 were duplicates and 18 were incomplete. After excluding these, 422 valid questionnaires remained, yielding a response rate of 93.36%. A total of 422 patients were included, with an average age of 43.28 ± 12.24 years. Further details can be found in Tables 1–3.
Presence of comorbidities, recent CD4 count, duration since HIV infection, duration of ART, and route of transmission
Prevalence of symptoms in the fatigue-related symptom cluster in HIV/AIDS patients
Among male HIV/AIDS patients, the three most prevalent symptoms in the fatigue-related symptom cluster were fatigue (86.32%), sleep problems (44.63%), and frailty (43.32%). For female HIV/AIDS patients, the most prevalent symptoms were fatigue (73.04%), sexual dysfunction (72.17%), and sleep problems (45.22%). Detailed information can be found in Table 4.
Network analysis of fatigue-related symptom clusters in HIV/AIDS patients
The network centrality indicators reveal that the top three symptoms in terms of strength in the male network are sleep disturbance (D5, rs = 1.61), fatigue severity and type (C1, rs = 1.60), and sleep quality (D1, rs = 1.52). The top three symptoms in terms of closeness centrality are sleep disturbance (D5, rc = 1.52), use of hypnotic drugs (D6, rc = 1.22), and sleep quality (D1, rc = 1.10). The top three symptoms in terms of betweenness centrality are use of hypnotic drugs (D6, rb = 2.00), sleep disturbance (D5, rb = 1.712), and sleep quality (D1, rb = 1.28). In the female network, the top three symptoms in terms of strength are sexual climax (B4, rs = 2.16), daytime function (D7, rs = 1.66), and sexual satisfaction (B5, rs = 1.09). The top three symptoms in terms of closeness centrality are fatigue characteristics (C2, rc = 1.79), daytime function (D7, rc = 1.53), and sleep quality (D1, rc = 1.47). The top three symptoms in terms of betweenness centrality are daytime function (D7, rb = 1.89), sexual satisfaction (B5, rb = 1.84), and sleep quality (D1, rb = 1.65). The symptom network of the fatigue-related symptom cluster in patients with HIV/AIDS is shown in Figure 2, the centrality measures of symptoms within the fatigue-related symptom network in individuals living with HIV/AIDS is shown in Figure 3. Studies have indicated that betweenness and closeness centrality measures tend to be less stable and may not be optimal for assessing node centrality in network analysis (14, 29, 30). Therefore, this study focuses solely on node strength as the criterion for identifying core symptoms. The network analysis results show that the node strength stability coefficient for the male network is 0.60, indicating good stability, while for the female network, the stability coefficient is 0.37, which is considered acceptable. In summary, the core symptoms for male patients are sleep disturbance, fatigue severity and type, and sleep quality. For female patients, the core symptoms are sexual climax, daytime function, and sexual satisfaction.
Symptom network of the fatigue-related symptom cluster in patients with HIV/AIDS.
Centrality measures of symptoms within the fatigue-related symptom network in individuals living with HIV/AIDS.
Univariate analysis of factors affecting sleep problems in HIV/AIDS patients
Univariate analysis of factors, including HIV status of sexual partners, duration of ART treatment, income, employment status, and number of sexual partners, revealed statistically significant differences in PSQI scores among HIV/AIDS patients (p < 0.05). Detailed results are shown in Table 5.
Multivariate linear regression analysis of factors affecting sleep problems in HIV/AIDS patients
Multivariate linear regression analysis identified the HIV status of sexual partners, duration of ART treatment, number of sexual partners, and employment status as independent factors influencing sleep problems in HIV/AIDS patients (p < 0.05). Detailed results are presented in Table 6.
Discussion
Fatigue is the Most common and disturbing symptom reported by HIV/AIDS patients
Fatigue is the most frequently reported and bothersome symptom in HIV/AIDS patients, with the highest prevalence in the fatigue-related symptom cluster. This finding aligns with previous studies (11). HIV-related fatigue (HRF) refers to a subjective experience of tiredness or exhaustion caused by HIV infection, characterized by both physical and psychological fatigue (31). Although HRF does not directly reduce life expectancy, it significantly impacts quality of life, mental health, and treatment adherence, ultimately diminishing treatment outcomes and increasing mortality rates (32, 33). Network analysis results indicate that the node strength for fatigue type and severity (rs = 1.60) ranks second in the male network, suggesting that fatigue holds a central position within the fatigue-related symptom cluster for male HIV/AIDS patients. This emphasizes the need for healthcare professionals to regularly assess symptom changes during follow-up visits, encourage patients to report symptoms proactively, and prevent the onset of HRF. Previous studies have highlighted that unhealthy sleep habits and the misuse of sedative medications can disrupt the sleep patterns of HIV/AIDS patients, leading to poor sleep quality and, consequently, fatigue (34). Therefore, symptom management for fatigue in HIV/AIDS patients should also prioritize addressing sleep issues.
Sleep problems as a CORE symptom in the fatigue-related symptom cluster of HIV/AIDS patients
The prevalence of sleep problems in male HIV/AIDS patients is 43.32%, while in females, it is 45.22%, which is consistent with previous studies (35, 36). Network analysis results indicate that sleep issues are a core symptom within the fatigue-related symptom cluster in HIV/AIDS patients. Sleep problems can occur at any stage of ART and are one of the most prevalent core symptoms. This could be related to the type of antiretroviral medications used, such as efavirenz, a commonly prescribed non-nucleoside reverse transcriptase inhibitor in developing countries. Efavirenz’s main side effects include neuropsychiatric symptoms, and studies show that 68.1% of HIV/AIDS patients using efavirenz experience sleep disturbances (37). Therefore, it is recommended that healthcare providers identify patients with sleep problems early during follow-up visits. For patients suspected of experiencing sleep disturbances due to efavirenz, timely medication adjustments should be considered. Due to gender differences, when managing sleep problems in patients, male patients should be carefully monitored for symptoms of sleep disturbances, while female patients should receive particular attention for improvements in daytime functioning.
Higher prevalence of sexual dysfunction in female HIV/AIDS patients compared to males
The prevalence of sexual dysfunction in female HIV/AIDS patients is 72.17%, significantly higher than in male patients (35.83%), which aligns with previous research findings (38, 39). This may be attributed to the fact that women are more likely to experience psychological stress due to the disease. The stigma associated with HIV makes female patients more vulnerable to social discrimination and human rights violations, which can intensify their psychological burden, leading to greater depression and, ultimately, sexual dysfunction (39). Additionally, with increasing age, women’s estrogen levels gradually decline, negatively affecting sexual desire and arousal. The relaxation of the pelvic floor muscles and the sexual atrophy of reproductive organs further decrease their responsiveness to sexual stimuli, thereby increasing the likelihood of sexual dysfunction (40). Studies have shown that hormonal imbalances during menopause, particularly the reduction in estrogen and testosterone levels, are significantly associated with various aspects of sexual dysfunction (38). As ART becomes more widely accessible, the life expectancy of HIV/AIDS patients has increased, and more female patients are entering menopause. However, there is a lack of knowledge regarding the management of menopausal symptoms among these women (41). Therefore, healthcare professionals should provide specialized identification and support for sexual issues in menopausal women with HIV/AIDS.
The influence of partner’s HIV status on HIV/AIDS patients’ core fatigue-related symptoms
The influence of a partner’s HIV infection status on HIV/AIDS patients
The infection status of a sexual partner is an independent factor influencing sleep problems in HIV/AIDS patients, which contrasts with findings from previous studies. In past research (35, 42), the infection status of sexual partners was not specifically addressed, which may account for the discrepancy in results. When both the patient and their sexual partner are HIV-positive, they are more likely to disclose their status to each other in order to gain emotional support, which can reduce anxiety and depression symptoms (43), improve treatment adherence, and indirectly have a positive effect on the patient’s sleep quality. However, when the sexual partner is HIV-negative, disclosure may lead to negative consequences due to the stigma associated with the disease, such as loss of economic support, blame, abandonment, physical and emotional abuse, discrimination, and family breakdown. As a result, most patients choose to conceal their HIV status from their partner (44). In daily interactions, the fear of being abandoned by their partner or transmitting HIV to a non-infected partner creates significant psychological stress, which in turn affects their sleep quality (45). Therefore, healthcare providers should adopt measures to reduce the stigma surrounding the disease for these patients and encourage them to disclose their HIV status to their sexual partners.
The duration of antiretroviral therapy
The duration of ART is an independent factor influencing sleep problems in HIV/AIDS patients, which is consistent with previous studies (35). The longer the duration of ART, the higher the likelihood that the patient will experience sleep problems. Research has shown that HIV/AIDS patients who have been on ART for 5–9 years and more than 10 years are 5.65 times and 17.85 times more likely to experience sleep problems, respectively, compared to those who have been on ART for less than 1 year (46). Long-term use of antiretroviral drugs can affect the nervous and endocrine systems, and some medications may induce anxiety, depression, or cause discomfort such as nausea and headaches, all of which can disrupt sleep. Additionally, prolonged ART use may lead to significant impacts on the patient’s daily life, including drug resistance. When resistance occurs, patients need to switch their treatment regimen, which can trigger concerns about disease progression and poor treatment outcomes. This ongoing psychological burden can cause mental stress, making it difficult for patients to relax and fall asleep, thereby reducing sleep quality. In contrast to previous studies (35), this research found that a duration of ART treatment between 3 and 5 years had a more pronounced impact on sleep quality in HIV/AIDS patients. The reasons for this difference remain unclear, and further investigation is needed.
Number of sexual partners
The number of sexual partners has been identified as a factor influencing sleep quality among individuals living with HIV/AIDS. However, this finding contrasts with some international studies. For instance, Mazonson et al. (47) found that among older adults living with HIV in the United States, individuals with a single sexual partner reported significantly lower levels of loneliness and depression compared to those with multiple partners. Notably, those with five or more partners exhibited higher levels of loneliness and depressive symptoms, which are known to adversely affect sleep quality (48). The discrepancy between these findings and those from other cultural contexts may be attributed to differing societal attitudes toward sexuality. In Western cultures, more liberal views on sexual relationships may mitigate the psychological impact of having multiple partners. Conversely, in cultures influenced by traditional values, such as those prevalent in China, conservative attitudes toward sexuality may lead to increased psychological distress for individuals with multiple sexual partners, potentially affecting their sleep quality. This cultural conservatism can result in heightened feelings of guilt or shame, which are associated with poor sleep outcomes. Given the limited research on the relationship between the number of sexual partners and sleep quality among HIV/AIDS patients in various cultural settings, further studies are warranted to explore this association comprehensively.
Employment status
Employment status has been identified as a significant factor influencing sleep quality among PLWHA, aligning with findings from previous research (49). Several mechanisms may explain this association. Economically, individuals with stable employment typically experience less financial strain, which can reduce stress levels and promote better sleep. Conversely, unemployment can lead to financial hardship, potentially resulting in maladaptive coping behaviors such as smoking, excessive alcohol consumption, and overeating. These behaviors are known to negatively impact sleep quality. Psychologically, unemployment is often linked to increased levels of anxiety and depression. These mental health challenges are closely associated with sleep disturbances (50). Given these considerations, healthcare providers should pay particular attention to the psychological wellbeing of unemployed PLWHA during follow-up visits. Interventions may include counseling, stress management strategies, and referrals to mental health services to address underlying issues contributing to poor sleep quality.
Limitations
This study has several limitations: (1) The participants were recruited from a single hospital, which may limit the generalizability of the findings. Future research should consider employing a multicenter design to enhance the external validity of the results. (2) As a cross-sectional study, it cannot establish causal relationships or assess the stability of core symptoms over time. Longitudinal studies are needed to examine the temporal dynamics and persistence of these symptoms. (3) The relatively small sample size of female participants may have affected the stability of the network structure analyses for this subgroup. Increasing the number of female participants in future studies would allow for more robust and reliable gender-specific analyses.
Conclusion
This study employed network analysis to construct a symptom network of fatigue-related symptom clusters among individuals living with HIV/AIDS, identifying sleep disturbances as the central symptom within this cluster. Subsequent multiple linear regression analysis revealed that factors such as the HIV status of sexual partners, duration of ART, number of sexual partners, and employment status are independent predictors of sleep disturbances in this population. These findings underscore the importance for healthcare providers to proactively identify patients experiencing sleep disturbances during follow-up visits. Implementing targeted management strategies may prevent the onset of fatigue-related symptom clusters. Moreover, when patients present with such clusters, focused interventions addressing sleep disturbances can not only alleviate the severity of sleep-related symptoms but also mitigate the intensity of other associated symptoms. This approach can enhance the precision and efficacy of symptom management in individuals living with HIV/AIDS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Deeks SG Lewin SR Havlir DV. The end of AIDS: HIV infection as a chronic disease. Lancet. (2013) 382:1525–33. doi: 10.1016/S 0140-6736(13)61809-7, 24152939 PMC 4058441 · doi ↗ · pubmed ↗
- 2Webster P. UNAIDS survey aligns with so-called fourth 90 for HIV/AIDS. Lancet. (2019) 393:2188. doi: 10.1016/S 0140-6736(19)31231-0, 34509217 · doi ↗ · pubmed ↗
- 3Miaskowski C Barsevick A Berger A Casagrande R Grady PA Jacobsen P . Advancing symptom science through symptom cluster research: expert panel proceedings and recommendations. J Natl Cancer Inst. (2017) 109:djw 253. doi: 10.1093/jnci/djw 25328119347 PMC 5939621 · doi ↗ · pubmed ↗
- 4Wilson NL Azuero A Vance DE Richman JS Moneyham LD Raper JL . Identifying symptom patterns in people living with HIV disease. J Assoc Nurses AIDS Care. (2016) 27:121–32. doi: 10.1016/j.jana.2015.11.009, 26790340 PMC 4916902 · doi ↗ · pubmed ↗
- 5Voss JG Barroso J Wang T. A critical review of symptom management nursing science on HIV-related fatigue and sleep disturbance. Int J Environ Res Public Health. (2021) 18:10685. doi: 10.3390/ijerph 182010685, 34682431 PMC 8535986 · doi ↗ · pubmed ↗
- 6Zhu Z Zhao R Hu Y. Symptom clusters in people living with HIV: a systematic review. J Pain Symptom Manag. (2019) 58:115–33. doi: 10.1016/j.jpainsymman.2019.03.018, 30951828 · doi ↗ · pubmed ↗
- 7Tsai YF Hsiung PC Holzemer WL. Validation of a Chinese version of the sign and symptom checklist for persons with HIV diseases. J Pain Symptom Manag. (2003) 25:363–8. doi: 10.1016/s 0885-3924(02)00687-5, 12691688 · doi ↗ · pubmed ↗
- 8Bloch M. Frailty in people living with HIV. AIDS Res Ther. (2018) 15:19. doi: 10.1186/s 12981-018-0210-2, 30445966 PMC 6240180 · doi ↗ · pubmed ↗