Evaluation of Resistance Dynamics in Pseudomonas aeruginosa Isolated From ICUs of a Tertiary-Level Hospital in Eastern India: A Five-Year Study
B. Prince, A. Raj Kumar Patro, Ipsa Mohapatra, Nipa Singh, Subhra Snigdha Panda, Sujit Pradhan, Nirmala Poddar, Pragati Panda, A. Susanna, Rajesh K Dash, Basanti Kumari Pathi, Dipti Pattnaik

TL;DR
This study analyzed antibiotic resistance trends in Pseudomonas aeruginosa from hospital ICUs in eastern India over five years, finding concerning levels of drug-resistant strains.
Contribution
The study provides a detailed five-year analysis of Pseudomonas aeruginosa resistance dynamics in eastern Indian ICUs, highlighting trends in MDR, DTR, and XDR isolates.
Findings
P. aeruginosa showed highest resistance to piperacillin/tazobactam, imipenem, and meropenem.
Resistance to several antibiotics declined over the 2021-2025 period.
Most isolates were from adult ICUs, with a male predominance in cases.
Abstract
Background Pseudomonas aeruginosa, an important nosocomial bacterial pathogen, poses serious healthcare challenges, particularly in ICUs, leading to morbidity and mortality. Moreover, the emergence of multidrug-resistant (MDR), difficult-to-treat resistant (DTR), and extensive drug-resistant (XDR) isolates has resulted in very limited treatment options. Limited data are available on the antibiotic susceptibility patterns of P. aeruginosa in eastern India during the study period. This study aimed to generate insights into the resistance profile of P. aeruginosa over a five-year period. Materials and methods This retrospective study was conducted from 2021 to 2025 in a tertiary care hospital in Bhubaneswar, India. Samples from ICU patients, including respiratory samples, blood, pus, urine, tissue, and swabs, were cultured on appropriate media. Bacterial identification and antimicrobial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
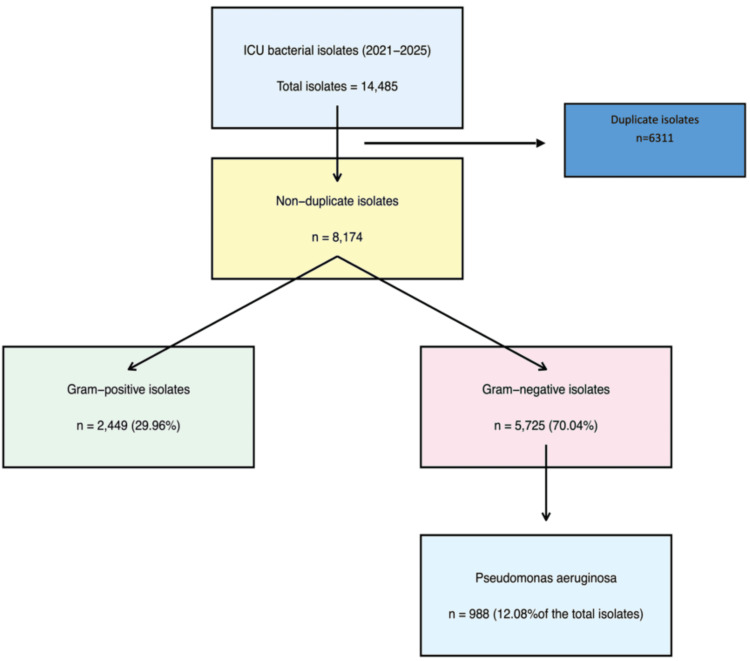 Figure 1
Figure 1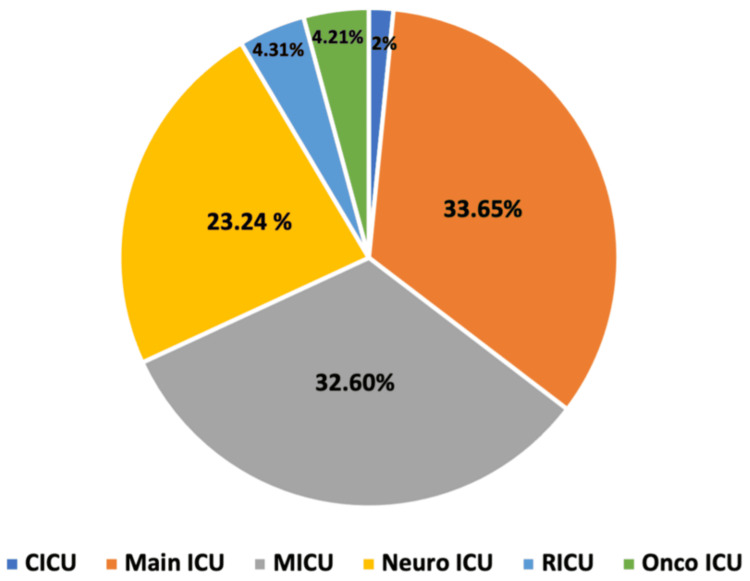 Figure 2
Figure 2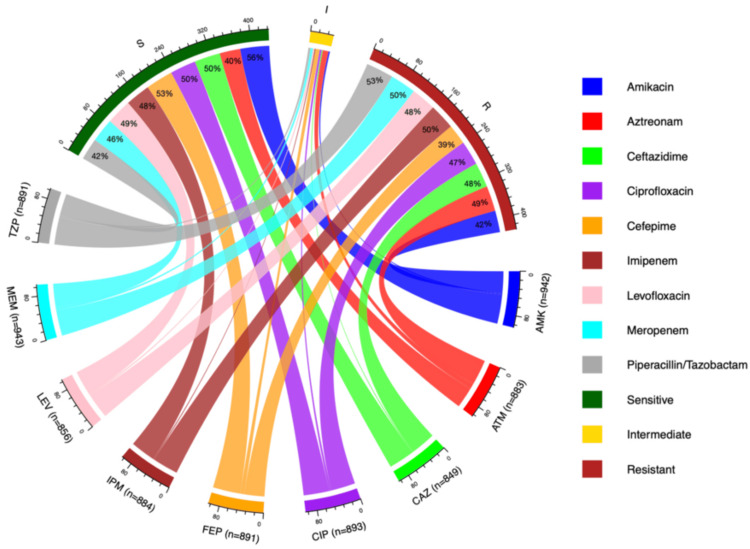 Figure 3
Figure 3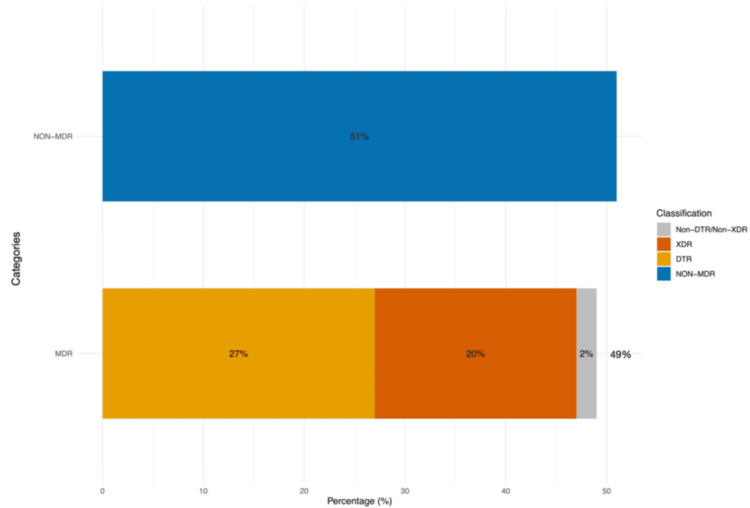 Figure 4
Figure 4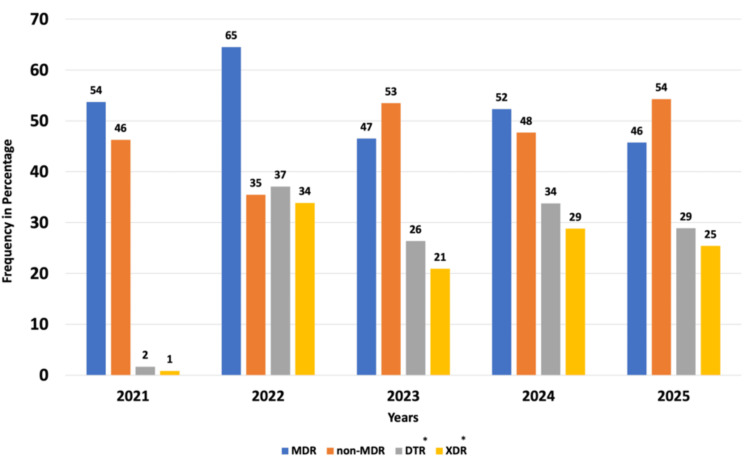 Figure 5
Figure 5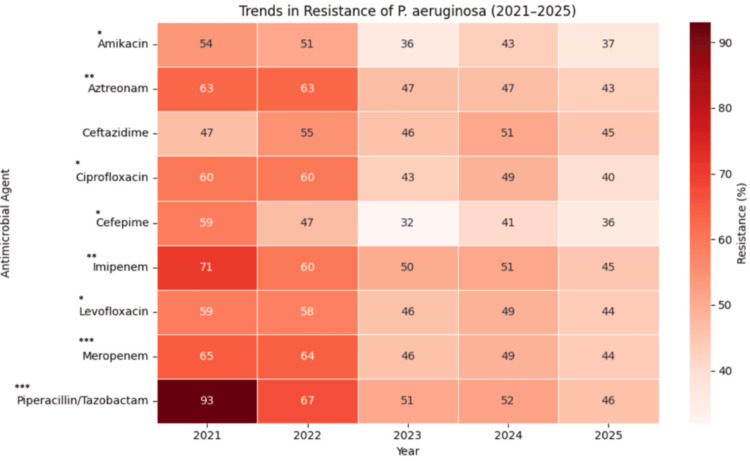 Figure 6
Figure 6| Demographic variables | n = 988 | Percentage (%) |
| Gender | ||
| Male | 659 | 67 |
| Female | 329 | 33 |
| Age (in years) | ||
| 0-10 | 27 | 3 |
| 11-20 | 33 | 3 |
| 21-30 | 59 | 6 |
| 31-40 | 87 | 9 |
| 41-50 | 129 | 13 |
| 51-60 | 217 | 22 |
| >60 | 436 | 44 |
| Category | Test statistic | df | p-Value | Adjusted p-value |
| MDR | 4.27 | 1 | 0.038 | 0.077 |
| Non-MDR | 4.03 | 1 | 0.044 | 0.077 |
| DTR | 19.705 | 1 | 9.037 × 10⁻⁵ | 1.26 × 10⁻⁵ |
| XDR | 21.719 | 1 | 1.26 × 10⁻⁵ | 2.71 × 10⁻⁵ |
| Antibiotic | Test statistic | df | p-Value | Adjusted p-value |
| Amikacin | 8.719 | 1 | 0.003 | 0.012 |
| Aztreonam | 14.331 | 1 | 0.006 | 0.001 |
| Ceftazidime | 0.925 | 1 | 0.336 | 0.336 |
| Ciprofloxacin | 9.189 | 1 | 0.002 | 0.012 |
| Cefepime | 6.655 | 1 | 0.01 | 0.028 |
| Imipenem | 14.295 | 1 | 0.0002 | 0.001 |
| Levofloxacin | 5.312 | 1 | 0.021 | 0.042 |
| Meropenem | 16.056 | 1 | 6.15 × 10⁻⁵ | 0.0005 |
| Piperacillin/tazobactam | 39.217 | 1 | 3.79 × 10⁻¹⁰ | 3.41 × 10⁻⁹ |
| Variables | Total (n = 988) | MDR (n = 486) | Non-MDR (n = 502) | Test statistic | df | p-Value |
| Gender | ||||||
| Male | 659 (67%) | 335 (51%) | 324 (49%) | 1.95* | 1 | 0.16 |
| Female | 329 (33%) | 151 (46%) | 178 (54%) | |||
| Comorbidities | ||||||
| Diabetic | 370 (37%) | 173 (47%) | 197 (53%) | 1.25* | 1 | 0.26 |
| Nondiabetic | 618 (63%) | 313 (51%) | 305 (49%) | |||
| HTN | 480 (49%) | 225 (47%) | 255 (53%) | 1.83* | 1 | 0.18 |
| Non-HTN | 508 (51%) | 261 (51%) | 247 (49%) | |||
| Lifestyle behavior | ||||||
| Alcoholic | 20 (2%) | 11 (55%) | 9 (45%) | 0.09* | 1 | 0.76 |
| Nonalcoholic | 968 (98%) | 475 (49%) | 493 (51%) | |||
| Smoker | 11 (1%) | 6 (55%) | 5 (45%) | 0* | 1 | 1 |
| Nonsmoker | 977 (99%) | 480 (49%) | 497 (51%) | |||
| Outcome | ||||||
| Death | 361 (37%) | 174 (48%) | 187 (52%) | 0.17* | 1 | 0.68 |
| Normal discharge | 627 (63%) | 312 (50%) | 315 (50%) | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Antibiotic Use and Resistance · Nosocomial Infections in ICU
Introduction
In the current era, where antimicrobials are widely available over the counter and extensively used in healthcare, industry, and agriculture, antimicrobial resistance (AMR) has emerged as a serious global crisis. These infections are difficult to treat and often lead to prolonged hospitalization, increased medical costs, significant morbidity, and mortality. In response to the rising burden of AMR, WHO launched the Global Antimicrobial Resistance and Use Surveillance System in 2015 to actively monitor AMR across countries and strengthen findings through systematic data management [1]. In 2019, the United Nations Interagency Coordination Group on AMR reported that drug-resistant infections account for nearly 700,000 deaths annually worldwide, a figure projected to reach approximately 10 million deaths per year by 2050 [2].
AMR can directly or indirectly affect the Sustainable Development Goals (SDGs), which are designed to address global health challenges. Antibiotics are the backbone of therapeutics, and reporting critical trends in AMR is essential for achieving SDG 3, which aims to ensure health and well-being across all age groups [3]. A collaborative global One Health approach has been adopted by quadripartite organizations, including the Food and Agriculture Organization, World Organisation for Animal Health, WHO, and United Nations Environment Programme, to harmonize and improve the health of people, animals, and ecosystems collectively [4]. The Government of India has also launched a nationwide One Health Mission, managed by the Principal Scientific Advisor in coordination with multiple ministries and implemented by the Indian Council of Medical Research (ICMR), to improve health outcomes and address challenges across sectors [5].
Pseudomonas aeruginosa is a significant nosocomial pathogen, particularly in ICUs, due to its broad resistance to multiple antibiotic classes, resulting in multidrug-resistant (MDR) and difficult-to-treat resistant (DTR) isolates [6]. MDR isolates are defined as those not susceptible to at least one drug in ≥3 antimicrobial classes, whereas DTR isolates are those not susceptible to ceftazidime, cefepime, ciprofloxacin, imipenem, meropenem, and piperacillin-tazobactam [7]. Extensive drug-resistant (XDR) isolates are defined as those not susceptible to all but ≤2 antimicrobial classes [8].
Antibiotic resistance in *P. aeruginosa *arises from both intrinsic and acquired mechanisms. Intrinsic resistance includes increased AmpC beta-lactamase production, overexpression of efflux pump genes, and downregulation of outer membrane porins. Acquired resistance, such as mutational drug resistance and acquisition of carbapenem resistance genes via horizontal gene transfer, contributes to increased biofilm formation and resistance to last-resort drugs like carbapenems [9]. Genetic alterations in the *mucA22 *allele result in overproduction of alginate, an exopolysaccharide, enhancing biofilm formation in mucoid strains, which are commonly associated with cystic fibrosis infections [10]. Metallo-beta-lactamases such as blaNDM, blaVIM, and blaIMP, and serine carbapenemases like *blaKPC *and blaOXA, are primarily responsible for carbapenem resistance [11,12].
Carbapenem-resistant P. aeruginosa (CRPA) has been classified as a “high-priority pathogen” on the WHO Bacterial Priority Pathogens List, 2024 [13]. According to the ICMR’s annual report on the Antimicrobial Resistance Research and Surveillance Network 2024, P. aeruginosa exhibits higher resistance levels in ICUs compared with wards and OPDs [14].
Due to limited data on the prevalence and antibiogram of* P. aeruginosa in eastern India during this period, this study aims to provide a detailed analysis of the resistance dynamics of all P. aeruginosa* isolates, including drug-resistant strains, collected from ICU patients in a tertiary healthcare center in eastern India over a five-year period.
Materials and methods
Study setting, study duration, and data gathering
This retrospective study was conducted at a 2,600-bed multispecialty hospital in Bhubaneswar, India, from 2021 to 2025, following approval from the Institutional Ethics Committee (approval KIIT/KIMS/IEC/2389/2025). Data on the isolation and antibiogram of P. aeruginosa from all ICUs were retrieved from the hospital’s laboratory information system over the five-year period. Patient demographics, comorbidities, and risk factors were extracted from hospital records. To avoid duplication, only the first isolate from each patient was included in the analysis.
Isolates not susceptible to at least one drug from ≥3 antimicrobial classes were defined as MDR [7]. Isolates not susceptible to ceftazidime, cefepime, ciprofloxacin, imipenem, meropenem, and piperacillin-tazobactam were classified as DTR [7]. XDR isolates were defined as those not susceptible to all but ≤2 antimicrobial classes [8].
Sample collection and processing
As part of routine clinical care, specimens, including blood, pus, urine, and swabs, were collected under sterile conditions from ICU patients and transported immediately to the laboratory for bacterial identification and antimicrobial susceptibility testing (AST). All samples were initially screened macroscopically and microscopically to assess cellular components and detect bacterial pathogens using Gram stain.
Blood samples were collected in age-appropriate blood culture bottles and incubated in an automated blood culture system (BacT/ALERT 3D; bioMérieux, Marcy-l’Étoile, France) for up to five days or until flagged positive. Subcultures were performed upon a positive signal. Blood, pus, and other body fluids were inoculated onto blood agar and MacConkey agar (HiMedia Laboratories Pvt. Ltd., Thane, India) and incubated aerobically at 37°C for 24-48 hours. Other specimens were processed according to established guidelines [15,16]. Lactose-nonfermenting, oxidase-positive colonies were further identified using the VITEK 2 ID and AST system.
Bacterial Identification and AST using the VITEK 2 automated system
Isolated colonies were suspended in 0.9% normal saline to prepare a homogeneous 0.5 McFarland solution. Density was verified using VITEK^®^ DENSICHEK^® ^(bioMérieux). Bacterial identification and AST were performed using the VITEK 2 Compact system (bioMérieux) with specific ID and AST panels. The antibiotic panel included piperacillin/tazobactam, ceftazidime, aztreonam, imipenem, meropenem, amikacin, ciprofloxacin, and levofloxacin. Results were interpreted as susceptible, intermediate, or resistant according to the Clinical & Laboratory Standards Institute (CLSI) 2025 guidelines [17]. Intermediate results were analyzed as a separate category from susceptible and resistant.
Statistical analysis
Statistical analyses were performed using R software [18]. Associations between gender, comorbidities, risk factors, and patient outcomes with MDR versus non-MDR isolates were assessed using the chi-square test. Trends in resistance percentages over the years were evaluated using Cochran’s Armitage trend test. P-values were adjusted using the Holm-Bonferroni step-down procedure to reduce Type I error from multiple comparisons. A p-value <0.05 was considered statistically significant. AST patterns were visualized using chord diagrams in R [18], and resistance trends (percentages from 2021-2025) were depicted as heatmaps generated in Python [19].
Results
A total of 14,485 bacterial pathogens were isolated from ICUs during 2021-2025, of which data from 8,174 (56.4%) non-duplicate isolates were retrieved for analysis. Among these non-duplicate isolates, 2,449 (29.96%) were Gram-positive, and 5,725 (70.04%) were Gram-negative. Of the Gram-negative isolates, 988 (12.08%; 95% CI: 11.4-12.8) were identified as P. aeruginosa (Figure 1).
Flow chart depicting the prevalence of Pseudomonas aeruginosa
The highest occurrence was observed in adult ICUs (96.26%; 951/988), followed by the pediatric ICU (3.24%; 32/988) and neonatal ICU (0.5%; 5/988). Among adult ICU isolates (n = 951), 320 (33.65%) originated from the main ICU, 310 (32.60%) from the medical ICU, 221 (23.24%) from the neuro ICU, 41 (4.31%) from the respiratory ICU, 40 (4.21%) from the oncology ICU, and 19 (2%) from the cardiac ICU (Figure 2).
ICU-wise distribution of Pseudomonas aeruginosaCICU, cardiac ICU; MICU, medical ICU; Neuro ICU, neurology ICU; Onco ICU, oncology ICU; RICU, respiratory ICU
The majority of isolates were from male patients (67%; 659/988), compared to females (33%; 329/988). Patients were stratified into age groups: 0-10, 11-20, 21-30, 31-40, 41-50, 51-60, and >60 years. The mean age of the study population was 55 ± 17.52 years. Most isolates (436; 44.14%) were obtained from the geriatric cohort (>60 years) (Table 1).
The highest proportion of isolates was obtained from respiratory samples (50.10%; 495/988), followed by urine (14.68%; 145/988) and blood samples (14.27%; 141/988).
Figure 3 depicts the AST pattern of P. aeruginosa over the five-year period from 2021 to 2025. Results were interpreted according to the CLSI 2025 guidelines [17]. Maximum susceptibility was observed for amikacin (56%; 523/942), cefepime (53%; 471/891), ciprofloxacin (50%; 443/893), and ceftazidime (50%; 423/849). In terms of resistance, the highest rates were observed for piperacillin/tazobactam (53%; 473/891), followed by imipenem (51%; 446/884) and meropenem (50%; 467/943).
AST pattern of Pseudomonas aeruginosa over five yearsSusceptible and resistant rates are shown as percentages and interpreted according to the CLSI 2025 guidelines.AMK, amikacin; AST, antimicrobial susceptibility testing; ATM, aztreonam; CAZ, ceftazidime; CIP, ciprofloxacin; CLSI, Clinical & Laboratory Standards Institute; FEP, cefepime; IPM, imipenem; LEV, levofloxacin; MEM, meropenem; TZP, piperacillin/tazobactam
Of the total isolates, 49% (486/988) were identified as MDR, 51% (502/988) as non-MDR, whereas 27% (269/988) and 20% (200/988) were DTR and XDR organisms, respectively (Figure 4).
Prevalence of MDR, non-MDR, DTR, and XDR isolates over 2021-2025 (n = 988)DTR, difficult-to-treat; MDR, multidrug-resistant; XDR, extensive drug-resistant
Figure 5 illustrates the trends over the study period: MDR decreased from 54% (65/121) to 46% (171/374) (adjusted p = 0.0776), while non-MDR increased from 46% (56/121) to 54% (203/374) (adjusted p = 0.0776). DTR and XDR strains also exhibited periodic increases and decreases over the five years (adjusted p < 0.001).
*Trends of MDR, non-MDR, DTR, and XDR isolates over five years (percentages)Cochran’s Armitage trend test was used for statistical analysis. Significant trends are indicated as adjusted p < 0.001.DTR, difficult-to-treat; MDR, multidrug-resistant; XDR, extensive drug-resistant
Table 2 presents the adjusted p-values after Holm-Bonferroni correction for multiple trend tests. To ensure monotonicity, the p-value for the non-MDR group was adjusted so that no later p-value was smaller than a previous one.
After applying the Holm-Bonferroni correction to all nine trends, a highly significant decreasing trend in AMR from 2021 to 2025 was observed for piperacillin/tazobactam (adjusted p < 0.001) and meropenem (adjusted p < 0.001). Additionally, significant decreasing trends were observed for imipenem (adjusted p < 0.01), aztreonam (adjusted p < 0.01), amikacin (adjusted p < 0.05), ciprofloxacin (adjusted p < 0.05), cefepime (adjusted p < 0.05), and levofloxacin (adjusted p < 0.05). No significant trend was observed for ceftazidime (adjusted p > 0.05) (Figure 6).
Trends in resistance patterns (percentages) of Pseudomonas aeruginosa over five yearsCochran’s Armitage trend test was used to assess temporal trends. adjusted p < 0.05; ** adjusted p < 0.01; *** adjusted p < 0.001*
Table 3 presents the adjusted p-values of antibiotic resistance trends using the Holm-Bonferroni step-down correction.
Table 4 shows the association of gender, comorbidities, risk factors, and patient outcomes with MDR status. No significant associations were observed for gender (p = 0.16), diabetes (p = 0.26), hypertension (p = 0.18), alcohol consumption (p = 0.76), smoking (p = 1.00), or death (p = 0.68) with MDR. The chi-square test was used for statistical analysis of these variables.
Discussion
*P. aeruginosa *is a member of the ESKAPE pathogens, namely Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, P. aeruginosa, and *Enterobacter *species, significantly associated with nosocomial infections. Critically ill patients in ICUs are particularly vulnerable to healthcare-associated infections due to multiple comorbidities and compromised immune status. Additionally, the multiple resistance mechanisms and remarkable biofilm-forming ability of *P. aeruginosa *allow severe, persistent infections in susceptible patients. A recent study reported the presence of a novel pap 1 polyesterase in a clinical isolate capable of degrading medical-grade plastics, polycaprolactone, exacerbating the risk in hospital settings [20]. The emergence of CRPA has created numerous therapeutic challenges. Moreover, the worldwide dissemination of drug-resistant strains jeopardizes current treatment regimens, leading to detrimental effects on patient outcomes [11].
In our study, the prevalence of* P. aeruginosa *in ICU settings was 12.08%, which aligns with the findings of Patil et al. (2022) [21], who reported a slightly higher prevalence of 13.66% in ICUs. This study highlights the geriatric cohort (>60 years) as the most vulnerable group, as the majority of isolates were obtained from this population. However, Harsh et al. (2024) [22] documented higher occurrence in the 41-60 age group. These variations may reflect differences in study sites, populations, and time frames.
This study also shows a higher incidence of infection in males compared to females, consistent with Harsh et al. (2024) [22], Venkatasubramanyam et al. (2024) [23], and Thomsen et al. (2023) [24], suggesting that males may be at higher risk. Respiratory samples were the predominant specimen type, indicating a potential risk for conditions such as ventilator-associated pneumonia and chronic obstructive pulmonary disease. In contrast, Bekele et al. (2015) [25] reported a higher incidence of P. aeruginosa in females from urine samples. Therefore, the rate of isolation may depend on specimen type, comorbidities, and patient risk factors.
In this study, 49% of isolates were MDR, 51% non-MDR, 27% DTR, and 20% XDR. Selvam et al. (2025) [26] and Gill et al. (2016) [27] reported 52% and 50% MDR P. aeruginosa, respectively. Eid et al. (2025) [28] reported 21% DTR isolates, indicating the global emergence of DTR strains. Naik et al. (2021) [29] reported 19.5% XDR *P. aeruginosa *from ocular infections in southern India, suggesting similar prevalence across regions. A decline in MDR rates from 54% to 46% was observed in our study, consistent with Butscheid et al. (2025) [30], who reported reduced resistance post-COVID-19. This decrease may reflect active surveillance, robust antimicrobial stewardship, and infection control measures.
Year-wise analysis of DTR and XDR isolates revealed heterogeneous trends. In 2021, DTR and XDR prevalence was lower than in 2022, followed by a decline from 2022 to 2023. A subsequent rise was observed from 2023 to 2024, with a slight decline from 2024 to 2025. These variations likely reflect antibiotic usage patterns, selective pressure, and the evolution of AMR. Shabi et al. (2025) [31] similarly reported heterogeneous trends in DTR and XDR isolates from 2013 to 2022. Differences may also be influenced by COVID-19, hospital admission rates, variable antibiotic use, and regional resistance patterns.
The antibiogram revealed varying resistance across antibiotic classes. Piperacillin/tazobactam resistance was 53% (n = 891), comparable to Venkatasubramanyam et al. (2024) [23], who reported 32% (n = 562), whereas Vara et al. (2024) [32] reported 14% (n = 140) in ICU settings. Imipenem and meropenem resistance were both 50% (n = 884 and n = 943, respectively), consistent with reports by Vara et al. (2024) [32].
This study also demonstrates a decreasing trend in resistance to piperacillin/tazobactam, imipenem, cefepime, meropenem, ciprofloxacin, aztreonam, levofloxacin, and ceftazidime over five years, potentially reflecting judicious antibiotic use. These findings align with Rana et al. (2025) [33], who reported declining resistance to multiple antibiotics from 2023 to 2024, suggesting that this trend is not confined to ICUs but is also seen in wards, OPDs, and emergency rooms.
This study has several limitations. Being single-center, further multicentric studies with larger sample sizes are needed to better understand *P. aeruginosa *prevalence and resistance trends. The retrospective design limited the assessment of associations between gender, comorbidities, and risk factors. Additionally, results are based solely on phenotypic characterization via conventional and automated systems; molecular analysis of resistance mechanisms was not performed, limiting the depth of interpretation.
Conclusions
Despite the persistence of overall AMR, trend analysis revealed a decreasing pattern in our ICUs. This underscores the importance of time-trend analyses for effective antimicrobial surveillance, as pooled data may obscure recent improvements. Although the prevalence of MDR strains decreased slightly during the study period, MDR, DTR, and XDR strains continue to be reported in ICUs, which remains a significant concern. Non-MDR* P. aeruginosa *isolates continue to show an increasing trend in our setting. P. aeruginosa remains a critical nosocomial pathogen in ICU settings, where critically ill patients are highly vulnerable to severe infections. Therefore, continued active AMR surveillance, training of healthcare staff, robust infection prevention and control strategies, and rational antibiotic stewardship are essential to limit the persistence of resistant strains in ICUs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global antibiotic resistance surveillance report 2025: WHO Global Antimicrobial Resistance and Use Surveillance System (GLASS): summary World Health Organization 2025
- 2Antimicrobial resistance: a top ten global public health threat E Clinical Medicine E Clinical Medicine E Clinical Medicine 1012214120213487751210.1016/j.eclinm.2021.101221 PMC 8633964 · doi ↗ · pubmed ↗
- 3AMR and sustainable development goals: at a crossroads Global Health Aslam B Asghar R Muzammil S 732020243941520710.1186/s 12992-024-01046-8PMC 11484313 · doi ↗ · pubmed ↗
- 4The One Health approach—why is it so important?Trop Med Infect Dis Mackenzie JS Jeggo M 88420193115933810.3390/tropicalmed 4020088 PMC 6630404 · doi ↗ · pubmed ↗
- 5National One Health mission 12 2025 https://www.psa.gov.in/one Health Mission
- 6Current trends in the epidemiology of multidrug-resistant and beta-lactamase-producing Pseudomonas aeruginosa in Asia and Africa: a systematic review and meta-analysis Peer J Salleh MZ Nik Zuraina NM Deris ZZ Mohamed Z 013202510.7717/peerj.18986 PMC 1186703740017659 · doi ↗ · pubmed ↗
- 7Moving towards a standardized definition of antimicrobial resistance: a comparison of the antimicrobial susceptibility profile of difficult-to-treat resistance (DTR) versus multidrug-resistant (MDR) Pseudomonas aeruginosa clinical isolates (CANWARD, 2016-2021)Diagn Microbiol Infect Dis Walkty A Karlowsky JA Lagacé-Wiens PR Baxter MR Adam HJ Bay DC Zhanel GG 11613010820243800671010.1016/j.diagmicrobio.2023.116130 · doi ↗ · pubmed ↗
- 8Proposed amendments regarding the definitions of multidrug-resistant and extensively drug-resistant bacteria Expert Rev Anti Infect Ther Rafailidis PI Kofteridis D 1391462020223415288710.1080/14787210.2021.1945922 · doi ↗ · pubmed ↗