Surgery as a greedy job: The valorization of the worker's professionalism for women in surgery
Maria Irene Bellini, Pasquale Passalacqua

TL;DR
The paper explores how long working hours in surgery disproportionately affect women, leading to burnout and hindering career progression.
Contribution
It highlights the impact of greedy jobs on women in surgery and suggests flexible working hours and technology as potential solutions.
Findings
Greedy jobs in surgery are common and mainly affect female and younger surgeons.
Long working hours lead to burnout, reduced research time, and hinder career progression for women.
Flexible working hours and technology could help reduce the negative impacts of greedy jobs.
Abstract
Greedy job is referred to a condition in which companies and/or institutions require employees to work beyond agreed-upon working hours or beyond agreed standards. With the current shortage of surgeons and increased number of women entering a surgical career, it is fundamental to consider their needs, distress, and motivation factors to implement the surgical workforce. A systematic search was performed to review literature addressing working hours disrespect and greedy jobs in surgery, aiming to report the current evidence with regards to the different impact on general surgeons. Greedy job in surgery is common and its consequences are predominantly affecting female gender and younger generation. Prolonged working hours were associated with burnout incidence, reduced time for research and eventually jeopardizing education. Furthermore, job satisfaction, earning and career progression…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
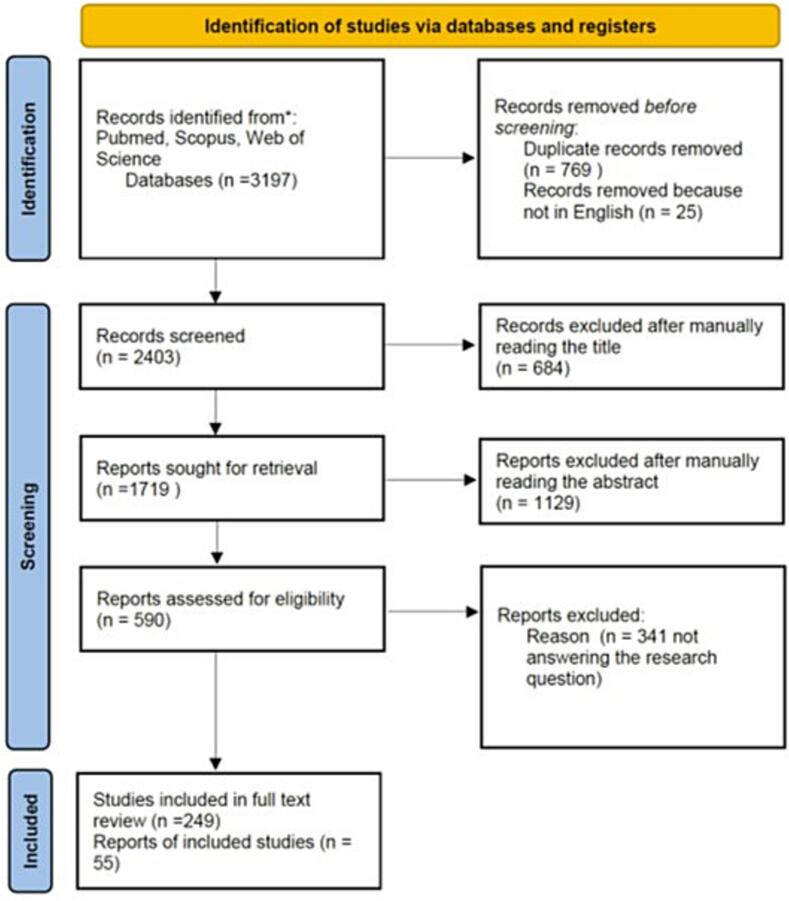 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiversity and Career in Medicine · Dental Education, Practice, Research · Emotional Labor in Professions
Introduction
Discrimination against women pursuing careers in the surgical field has deep historical roots, dating back to the very beginnings of the profession. This prejudice is starkly illustrated by figures like Sir James Paget, a prominent 19th-century British surgeon, who cautioned against women's entry into surgery could lead to the “disorganization of society,” fundamentally reflecting anxieties that challenging and defying traditional, defined gender roles would affect the established social order. Strikingly, despite over a century and a half of societal and professional evolution, this inherent bias remains a palpable reality: a survey conducted as recently as 2020 revealed in fact that only 67% of male surgeons expressed confidence in the professional competence of their female colleagues [1]. This lingering skepticism is often rationalized through a lens of gender-oriented societal norms, which disproportionately focus on women's assumed familial responsibilities and the perceived lifestyle implications these responsibilities have on their professional commitment and availability. This perspective subtly, yet powerfully, suggests that women's professional capabilities are inherently compromised by their roles outside of the operating room, perpetuating a cycle of discrimination that has plagued the surgical field since its inception.
The persistence of such attitudes highlights the systemic and cultural barriers that continue to impede true gender equality within surgery [2], therefore, as a professional field, it remains largely male-dominated, well beyond a simple pipeline issue.
Although such opposition, remarkable efforts have been paving the way to change, and in fact currently, women represent >50% of the medical workforce in many Western Countries, especially if we consider professionals aged <50 years [3]. However, despite these encouraging data, substantial gender gap persist, in a profession where restriction for duty hours have been controversial, including the downsides commonly hindered by “greedy” jobs.
As per 2023 Nobel Prize Claudia Goldin definition [4], greedy jobs identify situations in which companies and/or institutions require employees to work beyond agreed-upon hours or beyond certain standards. Employees of both sexes might face difficulties in meeting these demands, resulting in a conflict between work and life balance. In particular, it has been recognized as a possible cause of discrimination in accessing higher-skilled and more remunerated positions, especially for women.
These phenomena fall within the metaphor of the so-called “glass ceiling”, which refers to the socio-cultural barriers [5], usually invisible and insurmountable, that prevent minorities from opportunities for professional and career development, as well as the “sticky floor”, a discriminatory employment model that keeps the same individuals at the lower rungs of the job ladder, with limited mobility.
The aim of this review is to explore the current evidence in literature regarding women working in general surgery according to the implications of a “greedy job” definition, highlighting the discriminations implied and aiming at possible system developments for the valorization of each worker's professionalism.
Methods
A systematic search was performed within the PubMed, Scopus, and Web of Science electronic databases. Only original articles in English published from 2000 to date, and reporting on the work condition identifiable as greedy job, as previously described [4], were considered. Search terms included combinations of the keywords “greedy work”, “women in surgery” and “working hours”. The question we aimed to answer was “What are the implications of prolonged working hours for women surgeons?” Focus was posed on conditions associated with less than full time work, flexibility, career and salary progression and work-life conflicts, seen as mainly affecting women. We included all the articles written in English, with no zone restriction and reporting on general surgery and its subspecialties. Papers written in languages other than English, focusing on COVID-19 and disciplines other than general surgery were excluded from the analysis. We then narratively synthesized the themes extracted and summarized the findings in Table 1. The PRISMA diagram for the search is reported in Fig. 1.Table 1. Study characteristics, aims, and main findings.Table 1. AuthorYearCountryMethodObjectivePercentage of FemaleParticipants(Female/Total Participants)Main findingsAntiel et al.2013USASurveyImpact of duty hour regulations on QoL and burnout on surgical interns50/156 (32)Satisfaction from being a surgeon was high, but 1 in 7 considered givingup their careerArora et al.2008USASurveyProgram Directors views regarding duty hours(10)A group of PDs reported having no reduction in clinical duties, no protected time, and minimal salary compensationAshrafi et al.2024PakistanSurveyTo assess the optimum working hours for surgical interns and supervisors27/33 interns (82)The majority of residents and supervisors recommended reduced working hoursBalch et al.2010InternationalSurveyAssessments of burnout and QoL1037/7757 (15)Burnout and other measures of surgeon distress correlate directly with increasing work hours and nights on callBaldwin et al.2009USASurveyTo assess activities residents engage in, and how much time per week they spend in each activity378/617 (60)Activities outside of work and sleep hours correlate highly with residents' mood, learning, and satisfactionBarden et al.2002USASurveyHow the surgical residency training program at New York Hospital was modified to comply with Code 405 mandatesN/AReduction in resident work hours has salutary effects on perception of quality of life and basic education for surgical residentsBarger et al.2006USASurveyTo address the impact of extended-duration work shifts on patient safety in a large and more diverse population of interns(53)Extended-duration work shifts were associated with an increased risk of significant medical errors, adverse events, and attentional failures for fatigueBendorf et al.2010USASurveyTo evaluate working hours issues and identify factors impacting breast surgeon incomes and job satisfaction(41)Significantly higher job satisfaction scores among dedicated breast surgeons, despite the lower salariesBennett et al.2017USASurveyTo assess underreporting duty hours among surgical residents466/1003 (46)Female respondents more often cited exceeding duty hours owing to the guilt about leaving the hospitalBessen et al.2025USARetrospective analysisEvaluation of EHR use by surgeons30/91 (33)Women surgeons had a greater EHR burden than men, that might contribute to gender gap in career advancement and burnoutBilimoria et al.2016USASurveyTo assess adherence to duty hour requirements in the Standard Policy arm and examine how often and why duty hour flexibility was used in the Flexible Policy arm (FIRST Trial)1501/3795 (40)There were differences in duty hours worked by residents in the Flexible vs Standard Policy arms of the FIRST trial, but it appeared that residents generally used the flexibility for patient care and educational opportunities selectivelyBoerjan et al.2010NetherlandsSurveyTo observe the influence of gender and number of working hours on health, social support and job-related autonomy74/254 (29)Social support by supervisors strongly predicted health; men and senior residents were healthier than women and junior residents, respectively, and a high level of support by colleagues predicted health in female residentsBrown et al.2021USASurveyTo assess WLB and burnout for trauma surgeons84/291 (29)Females have higher burnout rate, with 43% being satisfied with WLB. Factors associated with a satisfying WLB were: lifestyle and fair compensation; midcareer, increased hours at work, decreased awake hours at homeChokshi et al.2009USASurveyTo explore the following 4 domains: demographics, time allotment, research activities, and effects of stressors36/314 (12)Female are more active in research than men, however, this involvement decreases as other profess-sional responsibilities increaseCoverdill et al.2006USASurveyHow surgical residents and faculty assessed the first year of the Accreditation Council for Graduate Medical Education duty-hour restrictions47/252 (19)Residents, especially female residents, view the restrictions more favorably than facultyDahlke et al.2018USASurveyTo assess differences in how male and female general surgery residents utilize duty-hour regulations and experience aspects of burnout and psychological well-being2831/7395 (38)Female more frequently stayed in the hospital >28 h or worked >80 h in a week and more frequently felt fatigued and burned outDholakia et al.2025New ZealandSurveyTo quantify the prevalence of burnout in surgical specialists and registrars at a tertiary center and identify contributory factors67/110 (61)Contributory factors were frustration with management, lack of resources and long working hours, with predominance towards fatigue and service provision over career progression among the registrar groupDossa et al.2019CanadaRetrospective analysisTo determine whether male and female surgeons have similar earnings for each hour spent operating in a fee-for-service system162/705 (23)Even when equal hours are worked, female surgeons earn less than male surgeons and have fewer opportunities to perform the most lucrative surgical proceduresDyrbye et al.2011USASurveyBurnout and career satisfaction1043/7858 (13)WHC appear to be a major contributor to surgeon burnout and are more common among women surgeonsDyrbye et al.2012USASurveyTo evaluate the relationship between WHC and the personal and professional characteristics of surgeons879/6240 (14)Hours worked per week, having children, sex, and work location or were independently associated with an increased risk for WHCElmore et al.2016USASurveyBurnout289/664 (44)69% surveyed met the criterion for burnout; of these 73% were womenGifford et al.2014USASurveyTo determine how often categorical general surgery residents seriously consider leaving residency112/288 (39)Women were more likely to continue to have serious thoughts of leaving as residency progressed for sleep deprivation and difficult interaction with facultyGoitein et al.2008USASurveyTo determine the effects of the resident WHL on the professional lives of faculty77/282 (28)Women were more than twice as likely as men to report a decrease in time for research or other academic pursuits because of WHLs and more than three times as likely to report an increased sense of responsibility for supervising patient careGray et al.2019USASurveyComparison of responses between men and women to detect any differences in career goals, salary expectation, and perspectives towards salary negotiation at a resident level.177/407 (44)Overall career goals were similar for men and women; however, women had lower future salary expectations and a significantly more negative view of salary negotiationHoffmann et al.2017Canada and SwitzerlandSurveyTo compare 2 surgical training programs with the potential to identify opportu- nities for program enhancement30/105 (29)Although residents and consultants in both institutions fear negative influence of reduced working hours on the training program, this was not the case Canada's residentsHughes et al.2023Canada and USAInterviewsFactors influencing surgeons' wellbeing8/17 (47)Women may have experienced respect and recognition issues more often than menHughes et al.2024InternationalSurveyTo utilize the concepts of stressors, satisfaction72/ (32)Paperwork and documentation were sources of frustration as well as problems with billing, coding and reimbursementIrani et al.2005USASurveyTo determine perceptionsof the effects of the ACGME dutyhour requirements65/238 (27)Residents report an improved QoLJanczewski et al.2024USASurveyTo assess factors associated with WLC and well-being2253/5133 (44)Female trainees were more likely to experience WLC, associated with career dissatisfaction, burnout, thoughts of attrition, and suicidalityKang et al.2015KoreaSurveyTo evaluate the level of occupational stress of Korean surgeons compared to other professions100/621 (16)Young age and female gender were found to be related to a high occupational stress scaleKawase et al.2024JapanSurveyTo assess factors affecting marriage and pregnancy/childbirth(100)Age at the first childbirth is higherKevric et al.2018AustraliaSurveyTo provide contemporary data on the mental health of surgical trainees and identify risk factors relating to poorer mental health outcomes34/83 (41)Hours of overtime worked, particularly unpaid overtime, were strong predictors of a poorer scoreKhorfan et al.2020USASurveyTo investigate the long-term effect of flexible duty-hour policies on resident outcomes1494/ (40)Residents in flexible duty-hour programs reported significantly fewer lapses in continuity than standard policy residentsKinslow et al.2020USASurveyTo identify the prevalence and nuances of reported burnout in general surgery resident to better understand which factors contribute the greatest risk39/81 (48)Both female and community-affiliated residents were at increased risk of reporting suicidal ideation.Kiyasu et al.2024JapanSurveyTo identify the problems trainees face during surgical training194/758 (26)Main identified issues related to long working hours and harassmentKuerer et al.2007USASurveyBurnout and career satisfaction108/548 (20)Burnout was more common among respondents <50 years and women. Devoting <25% of time to research, lower physical QoL, and ≤50 years were associated to burnout.Lachance et al.2014CanadaSurveyTo assess residents' and professors' perception on the implementation of a 16-hour workday restriction75/142 (49)Residents and professors perceive a mild negative effect on the educational environment and quality of care, whereas their perception on QoL is opposite.Leu et al.2020Australia and SwitzerlandSurveyTo characterize the prevalence of burnout and to identify individual and system-related predispositions for burnout202/412 (49)Reduced free time activities and augmented working hours increase the risk of burnout, whereas having children, salary satisfaction, and regulated weekly working hours decrease the same riskLund et al.2022USASurveyTo investigate the relationship between gender, gendered microaggressions, and burnout44/109 (40)Gendered microaggressions mediate the relationship between gender and burnoutMaruscak et al.2012CanadaSurveyTo compare the anticipated career practice patterns of surgical residents in the context of work-hour guidelines84/274 (31)More females plan to limit their postcall duty hours and to take a parental leave compared with their male resident colleagues.Mayer et al.2001USASurveyTo explore residents on views of parental leave and part-time practices or flexible working hours27/71 (38)2/3 surgeons would like to have more time off during trainingNagaraj et al.2022USASurveyTo evaluate the impact of duty hours and service obligations on surgical residents' general wellbeing(64)Higher service obligation scores led to overall lower wellness scores regardless of the number of hours reportedNiederee et al.2003USASurveyTo investigate surgical faculty and residents' attitudes towards duty-hour restrictions3033/1314 (23)Most residents support duty hours restrictions; surgical faculty are less supportive (more males). 70% women favor duty-hour restrictions, because of effects on personal livesOgawa et al.2018JapanSurveyTo collect data of depressive symptoms among residents429/1241 (65)A working week of 80 to 99.9 h was associated with a 2.83 fold higher risk and 100 h or more was associated with a 6.96-fold higher risk of developing depressive symptoms compared with a <60 h working week. No differences among sexesRasmussen et al.2020USASurveyTo assess experiences during medical school, residency, current surgical practice and work-life balance141/336 (42)Female surgeons were less likely to be satisfied with their career and they report significantly more bias during their professional development and careerSeidenstein et al.2024USASurveyTo assess marital status, relationship dynamics, personal life choices, the challenges and rewards of dual-healthcare relationships56/105 (53)Women were more likely to report at least one negative effect of a dual-healthcare relationshipShahi et al.2022NepalSurveyTo assess burnout41/147 (28)Being unmarried and hours of work per week (≥80 h) were significantly associated with high burnoutTabrizian et al.2011USASurveyTo investigate the reason for noncompliance with the work-hour regulation by surgical residents54 (38)Non-compliance with the work-hour regulation remains high and the reasons are multifactorial, as feeling guilty when leaving the hospital or told to stay lateTawfik et al.2021USASurveyTo determine factors associated with WLI1637/4370 (37)Largest gender disparities were observed in physicians aged 45 to 54 years, with youngest child aged ≥23 years and working <40 h per weekTroppmann et al.2009USASurveyTo study career dissatisfaction and inability to achieve work-life balance178/895 (20)No difference among sexes for career satisfaction, but 59% believed worked too muchVon Websky et al.2012SwitzerlandSurveyTo assess trainee's satisfactionN/ANo difference among sexes, but increasing working hours were significantly associated with dissatisfactionYutzie et al.2005USASurveyTo gain perspective regarding general surgery career choices while examining gender differences.5/90 (6)More women worked 40 h per week; no difference in income for fellowship-trained surgeons, but a disparity in income favored non–fellowship-trainedmenZhang et al.2021USASurveyTo assess burnout rates among breast surgeons453/660 (69)Breast surgeons who have been in practice for 5–9 years have particularly high overall burnout ratesZheng et al.2025USASurveyTo understand the current landscape of family planning among trainees155/234 (66)Work hours and female gender were associated with delayed childbirth. Females were significantly more impacted by time and career/education goalsLegend: ACGME: Accreditation Council for Graduate Medical Education; EHR: electronic health records; PD: program director; PTF: part-time clinical faculty; QoL: quality of life; WHC: work-home conflicts; WHL: workhour limitation; WLB: work-life balance; WLI: work-life imbalance.Fig. 1PRISMA flow diagram.Fig. 1
Results
The original search identified 3197 papers. After duplicate removal, selection for English language and exclusion for a different focus, the final inclusion for review consisted of 55 papers. The majority of the studies were surveys (n = 52), from the USA (n = 37) and of good evidence quality (Table 2).Table 2. Quality of evidence in the selected papers for the systematic review according to the Newcastle–Ottawa Scale.Table 2. AuthorSelectionComparability/ExposureOutcomeTotalEvidence qualityAntiel et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodArora et al.^⁎⁎⁎^^⁎⁎⁎^6SatisfactoryAshrafi et al.^⁎⁎⁎^^⁎⁎⁎^6SatisfactoryBalch et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodBaldwin et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodBarden et al.^⁎⁎⁎^^⁎⁎⁎^6SatisfactoryBarger et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodBendorf et al.^⁎⁎^^⁎⁎⁎^5GoodBennett et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodBessen et al.^⁎⁎⁎^^⁎⁎^^⁎⁎^6GoodBilimoria et al.^⁎⁎⁎^^⁎⁎⁎^6SatisfactoryBoerjan et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodBrown et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodChokshi et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodCoverdill et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodDahlke et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodDholakia et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodDossa et al.^⁎⁎⁎^^⁎⁎⁎^^⁎⁎^8GoodDyrbye et al. 2011^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodDyrbye et al. 2012^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodElmore et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodGifford et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodGoitein et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodGray et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodHoffmann et al.^⁎⁎⁎^^⁎⁎⁎^6SatisfactoryHughes et al. 2023^⁎⁎⁎^^⁎⁎⁎^^⁎^7GoodHughes et al. 2024^⁎⁎⁎^^⁎⁎⁎^6SatisfactoryIrani et al.^⁎⁎^^⁎⁎⁎^5SatisfactoryJanczewski et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodKang et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodKawase et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodKevric et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodKhorfan et al.^⁎⁎⁎⁎^^⁎⁎^^⁎⁎⁎^9Very goodKinslow et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodKiyasu et al.^⁎⁎⁎^^⁎⁎⁎^6SatisfactoryKuerer et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodLachance et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodLeu et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodLund et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodMaruscak et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodMayer et al.^⁎⁎⁎^^⁎⁎^5SatisfactoryNagaraj et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodNiederee et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodOgawa et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodRasmussen et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodSeidenstein et al.^⁎⁎^^⁎⁎⁎^5SatisfactoryShahi et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodTabrizian et al.^⁎⁎^^⁎⁎⁎^5GoodTawfik et al.^⁎⁎⁎^^⁎⁎^^⁎⁎⁎^8GoodTroppmann et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodVon Websky et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodYutzie et al.^⁎⁎⁎^^⁎⁎⁎^6SatisfactoryZhang et al.^⁎⁎^^⁎⁎^^⁎⁎⁎^7GoodZheng et al.^⁎⁎⁎^^⁎⁎⁎^6Satisfactory
Primary themes identified in relation to an excess of working hours were: 1) burnout incidence; 2) impact of flexible policies and research time; 3) repercussion in education; 4) job satisfaction; 5) earning discrepancy between genders; 6) risk for health and wellness; 6) effects on parenthood and childcare.
- Burnout incidence and quality of life in relation to prolonged working hours [6], [7], [8], [9], [10], [11], [12], [13], [14], [15], [16], [17], [18], [19], [20], [21], [22], [23], [24], [25]. Burnout is defined as emotional exhaustion, depersonalization, and low sense of personal accomplishment, eventually leading to attrition at work and desire to leave the job.
Burnout occur more frequently among young/mid-career surgeons aged <50 years. Prolonged working hours or ≥2 nights on call per week are consistently associated to poor work-life balance and work-home conflicts, thus surgery was not deemed a good career option any longer for up to 1 in 7 of the survey respondents.
It has been reported that women surgeons are at greater risk of family/work imbalance and burnout, with a frequent expectation that work should be prioritized over private life, a conception unfortunately also affecting the future of recruitment, as those who leave the profession look for specialties that are conducive to a more controllable lifestyle.
A general perception of a better quality of life from both genders respondents was reported with standard implementation of duty-hour restrictions; reasons to reduce working hours were more commonly associated to personal and family demands in females and to financial considerations or physical limitations in men.
- Impact of flexible policies and research time [26], [27], [28], [29]: work hour limitations seem to affect women differently from men, as women face a more than twice decrease in time for research or other academic pursuits, and a more than three times increased sense of responsibility for supervising patient care, in comparison to male colleagues.
Furthermore, women often report exceeding working hours limitations because of administrative work, rather than proper education, with a higher electronic health record burden. Given also the need for protected time to conduct research, involvement with other responsibilities decreases the possibility to actively participate in academic projects, with female sex showing an unmet interest preventing career progression.
-
Repercussion of duty-hour restriction in education [30], [31], [32], [33]. Working hours restrictions are perceived differently by the program directors, attendings and interns, in fact more faculty than residents report warnings about a negative impact on residency education and readiness for surgical autonomy. It is interesting to report that some program directors actually favor prolonged working hours, well beyond the law-restriction. Yet, both male and female residents generally favor the working hour limitations, although in some reports females also feel more frequently unprepared for surgical training and the profession. This might be a consequence of a less supportive program or presence of bias inherent to the surgical environment, especially regarding workers adopting less than full time training.
-
Job and career satisfaction [34], [35], [36], [37], [38], [39], [40], [41], [42]: literature shows that a working week between 31 and 45 h has the highest proportion of satisfaction and that activities outside of work and sleep hours correlate highly with residents' mood, learning, and satisfaction.
Reimbursement is considered inadequate given the unpredictability and irregularity of surgeons' work hours, and women tend to be more dissatisfied with their career progression. Interestingly, breast surgeons were found to have a higher degree of job satisfaction, in consideration of the predictability of their working hours, a different setting when compared to professionals involved with emergency surgical consults during night or weekend hours.
- Earning discrepancy between genders [43], [44], [45], [46], [47]: research shows that even when equal hours are worked, female surgeons earn less than male surgeons and have fewer opportunities to perform the most lucrative surgical procedures. Additionally, if no difference in income for fellowship-trained surgeons is observed, a disparity in income favors non–fellowship-trained men. Reasons might be various, like for example that women are more frequently underemployed, i.e. perform nursing tasks, with disrespect to their training. As a consequence, often women conceive lower salary expectations and a more negative view of salary negotiation in general.
Additionally, women frequently perform free tasks, like for example serving on committees and in administrative roles, with an increased amount of assignments, taking up time to devote to the surgical operations. With the necessity of being productive, this extra load could easily lead to an excess in working hours with no remuneration, or even worse, creating a salary gap with male colleagues.
- Excessive working hours and risk for health and wellness [48], [49], [50], [51], [52]: fatigue resulting from long shifts is commonly described among surgeons, leading to an increased risk of avoidable errors, adverse events, and attentional failures towards patient's care in clinical activity. Additionally, fatigue has been reported also to cause illness to surgeons, not only in the body, but also in terms of mental health.
Suicidality attempts and fatal events among surgeons occur and are recognized as an unfortunate consequence of an excess of fatigue and prolonged working hours. It is important to mention that dissatisfaction with the ability to maintain healthy habits appears to be more frequently associated with female gender and junior residents, while male and senior trainees generally report themselves in a better health status. To this regard, supervisor's support appears of fundamental importance for residents and workers, in fact a higher social support in the working environment is proved to lead to a higher probability of wellness.
- Excess of working hours and effects on parenthood and childcare [53], [54], [55], [56], [57], [58], [59]: to spend more time with family tends to be a reason for reducing working hours, especially for women and for surgeons in their 40s. Very often it is reported that the use of professional child care exceeds the number of working hours, meaning a discrepancy between the amount of hours required at work and those provided by child care.
Prolonged working hours are also known to be significantly associated with delay of childbearing, more significantly in women: trainees working over 80 h per week tend to delay childbirth more than those reporting less than 80-h workweeks.
Discussion
The present review shows that certain aspects of the surgical profession are identifiable with those described by Goldin for greedy jobs [4]. In particular, there is evidence of a direct correlation of working beyond duty hours with burn out incidence [7], poorer health status [49], decreased productivity [60] and lower career satisfaction [61]. Literature also highlights a more detrimental effect of greedy jobs on women, being accompanied by a gender pay-gap [45] and delay in childbearing and parenthood [12].
Despite flexible policies being in place from a few years [62], there has been an unconscious bias towards those healthcare professionals who were unable to remain longer outside the agreed working hours [41], arguing it might interfere with patient's care continuity [35], [60]. Yet, as reported also in the present review, such a culture has instead a detrimental effect, leading to attentional failures during lectures, rounds, and clinical activities. Furthermore, fatigue-related preventable adverse events could result in a fatality not only for patients [48], but also for workers, thus it is not recommendable to exceed established working hours standards [20], [50].
An important finding of the present review is that women tend to be involved more frequently in administrative roles [36], leading to a potential limitation in undertaking clinical work, going to theatre and being involved in prolonged and challenging cases. Literature reports in fact that female surgeons are often underemployed in comparison to their male peers, even after accounting for subspecialty and seniority [63], with a lower number of complex procedures in their portfolio. Arguments commonly listed to explain such a difference comprehend reduced availability for competing obligations. Yet, this motivation might be seen as discriminatory, in fact on this basis only, there should not be any effect on the complexity of cases that a surgeon could perform. On the contrary, flexible time workers are often hindered in their productivity evaluation assessment and career advancement [64].
In other words, there cannot be an automatic correlation between lower availability to exceed the expected working hours, and a reduction in career advancement and seniority [40] which inevitably leads to salary and promotion gaps [36], [47]. Instead, it is necessary to determine whether, based on the circumstances of the specific case (type of operations performed, methods of performance, etc.), the proportional relationship between recognized seniority and hours of attendance at work is rational or rather constitutes discrimination against those not exceeding their working hours duty [65].
Another consideration deriving from the data reported on the present review, is that the number of hours worked and unpaid overtime are associated with poorer mental health outcomes among surgical trainees [50]; these hours are often attributable to excessive administrative work, a burden that could be avoided with the supply of technology, for example with the use of artificial intelligence to help doctors in reducing tasks not immediately requiring human interaction. To this purpose, women surgeons had a greater electronic health record load than men [36]: for instance, literature shows that residents aged <30 years are more likely to exceed duty hours to complete charting/documentation, and females more often cited guilt about leaving the hospital as to why they exceed duty hours [35], [37], [66]. These findings indeed exacerbate the culture of an “old boys club” where women are prevented from entry because of their possible commitment to family and childcare [67] and social impediments for being fully devoted to the surgical career.
This flexibility is also with regards to tenure and promotion procedures of academic faculty, in order to allow accommodation of personal and family responsibilities, while continuing career progression [36]. There is evidence in fact, that surgeons do not significantly reduce clinical productivity after maternity or other types of leaves, so childbearing should not be discouraged or delayed [68], as instead it is reported frequently in case of surgery.
Finally, a remarkable finding is that both men and women agreed that they would be more interested in a surgical career if residency programs strictly adhered to the 80-hour work week [69]; thus interventions targeted to avoid the risks of a “greedy job” would indeed appeal more aspiring candidates to enter the profession or not to leave training. This would also overcome the current lack of vocations and ensure a more sustainable recruitment, given that the quality of care and level of procedural experience could be maintained with the introduction of initiatives seeking to decrease working hours in excess, reducing burnout and improving work-life balance.
This review presents some limitations: first, literature was mainly from the USA, therefore findings might be specific to this setting and more difficult to be generalized in other healthcare contexts. Secondly, they refer mostly to the period of implementation of the 80-hours worktime directives. Third, despite the evidence of greedy job in surgery, there has been paucity of reports specifically looking at this concept, thus the need to fill the gap by a look at the current evidence.
Recommendations
Flexibility and avoidance of “greedy” work hours are essential in surgery. The increasing use of technology, which allows for remote working, offers a key solution by reducing constraints related to space and time.
Work-commitments after the regular business hours should be discouraged, moving meetings and related issues to typical workdays. A fundamental cultural shift is needed, promoting an “anti-greed” perspective to close the gap in availability between men and women for additional work requests.
Suggested interventions for policymakers, clinicians and employers to mitigate work-home conflicts include:
- •Allocating protected time: for instance, assigning two protected weekday days annually for personal matters.
- •Improving the work environment: modernizing resident workspaces and providing additional meal funds [64], [70].
- •Prioritizing quality over quantity: valuing the quality of time spent at work more than the sheer number of hours.
- •Recognition of administrative roles in surgical careers as equally important to research and clinical tracks would ensure their contribution is better appreciated in terms of promotion and salary.
- •Increasing operator interchangeability, though not strictly timing procedures, is a potential solution. This supports female surgeons in gaining equivalent operating room skills [69], fostering their contribution to the ward organization, and preventing exclusion or discrimination due to an inability to work excessive hours.
Conclusion
Surgeons, while focusing on removing illness from patients, should protect their own rest, personal life, mental and physical health. This review highlights the impact of disregarding working hours in surgery, especially on women, leading to burnout, poor health, low productivity, decreased career satisfaction, gender pay-gap, and delayed parenthood. Respecting regular working hours directives is crucial for long-term careers and to overcome the lack of vocation to prospective surgeons. We advocate for personalized, sustainable working hours towards worker-centered care, identifying priorities for future research.
CRediT authorship contribution statement
Maria Irene Bellini: Writing – original draft, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Pasquale Passalacqua: Writing – original draft, Formal analysis.
Declaration of competing interest
The other author declares no conflict of interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ross S.B.Jadick M.F.Spence J.De Reus H.Sucandy I.Rosemurgy A.S.Men surgeons’ perceptions of women surgeons: is there a bias against women in surgery?Surg Endosc 34112020512251313190766310.1007/s 00464-019-07294-9 · doi ↗ · pubmed ↗
- 2Bellini M.I.Amabile M.I.Saullo P.Zorzetti N.Testini M.Caronna R.D'Andrea V.A woman's place is in theatre, but are theatres designed with women in mind? A systematic review of ergonomics for women in surgery J Clin Med 11122022349610.3390/jcm 11123496 PMID: 35743578; PMCID: PMC 922516935743578 PMC 9225169 · doi ↗ · pubmed ↗
- 3ENPAM report 2024
- 4Goldin C.Understanding the gender gap: An economic history of American women 1992 Oxford University Press
- 5Bellini M.I.Adair A.Fotopoulou C.Graham Y.Hutson A.Mc Nally S.Changing the norm towards gender equity in surgery: the women in surgery working group of the Association of Surgeons of Great Britain and Ireland’s perspective J R Soc Med 112820193253293141493610.1177/0141076819854194 PMC 6699022 · doi ↗ · pubmed ↗
- 6Antiel R.Reed D.Van Arendonk K.Wightman S.Hall D.Porterfield J.Effects of duty hour restrictions on core competencies, education, quality of life, and burnout among general surgery interns JAMA Surg 148520134484552332540410.1001/jamasurg.2013.1368 · doi ↗ · pubmed ↗
- 7Balch C.Shanafelt T.Dyrbye L.Sloan J.Russell T.Bechamps G.Surgeon distress as calibrated by hours worked and nights on call J Am Coll Surg 211520106096192085164310.1016/j.jamcollsurg.2010.06.393 · doi ↗ · pubmed ↗
- 8Barden C.Specht M.Mc Carter M.Daly J.Fahey T.Effects of limited work hours on surgical training J Am Coll Surg 195420025315381237575910.1016/s 1072-7515(02)01242-5 · doi ↗ · pubmed ↗