Comparative Urodynamic Study in Cadaver of Urethral Pressure Profilometry Between the Artificial Urinary Sphincter UroActive and the AMS800
Aurélien Beaugerie, Elliot Tokarski, Anne Denormandie, Juliette Cotte, Stéphanie Tran, Emmanuel Chartier‐Kastler, Pierre Mozer

TL;DR
This study compares a new adjustable artificial urinary sphincter, UroActive, with the current standard, AMS800, in cadavers to evaluate its ability to manage urinary incontinence.
Contribution
UroActive is a new electronic AUS with remotely adjustable pressure settings, offering a potentially wider range of urethral closure pressures than the AMS800.
Findings
UroActive achieved MUCP values covering the entire range of the three AMS800 PRBs.
There was a strong positive correlation between set pressures and MUCPs in both male and female cadavers.
UroActive remained fully functional throughout the study, with no communication or calibration issues.
Abstract
The artificial urinary sphincter (AUS) is currently the gold standard treatment for stress urinary incontinence in men, and it's also a treatment option for women in Europe. UroActive is a new electronic device that offers remotely adjustable settings, including device pressure. This study aims to compare the range of Maximal Urethral Closure Pressures (MUCPs) covered by UroActive with those covered by the current AMS800 in male and female cadavers. Six cadavers (3 males and 3 females) were implanted with an occlusive cuff (OC) positioned around the bulbar urethra in men and around the bladder neck in women. A MUCP measurement was performed for each of the 3 different AMS800 Pressure‐Regulating Balloons (PRBs): 51–60, 61–70, and 71–80 cmH2O, that were successively connected to the OC. The AMS800 PRB was then replaced by the UroActive Control Unit (CU), and MUCP measurements were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
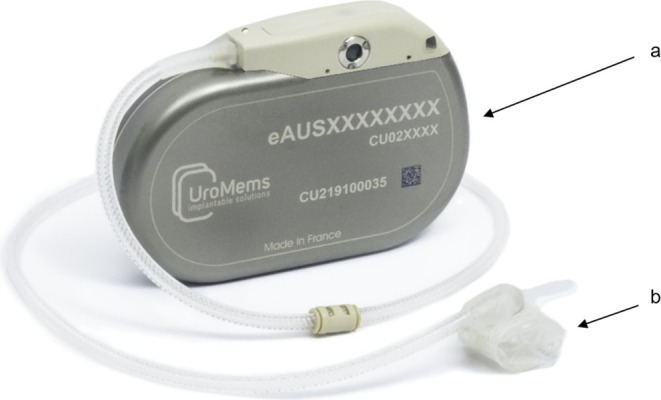 FIGURE 1
FIGURE 1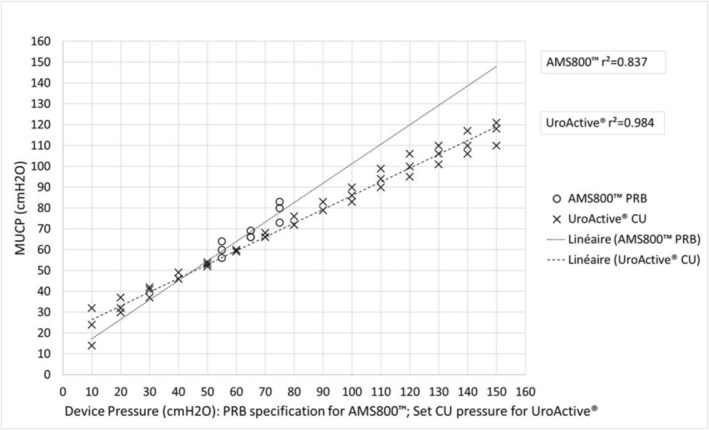 FIGURE 2
FIGURE 2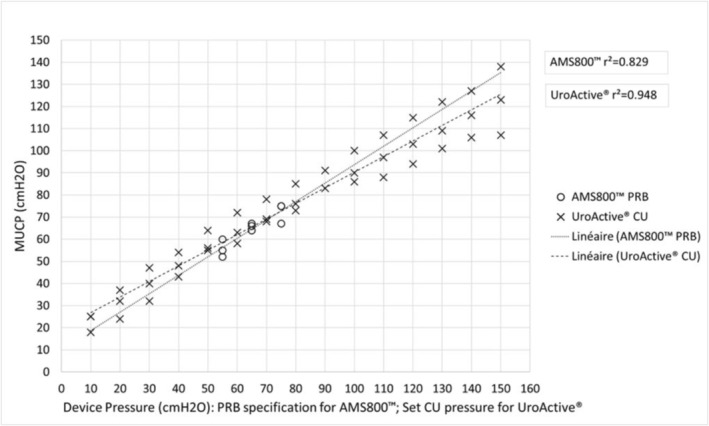 FIGURE 3
FIGURE 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPelvic floor disorders treatments · Urinary Bladder and Prostate Research · Urological Disorders and Treatments
Introduction
1
Stress urinary incontinence is a frequent pathology in both men and women [1, 2] that can lead to a significant social handicap for patients [3]. The Artificial Urinary Sphincter (AUS) is currently the gold standard treatment for stress urinary incontinence in men [4, 5]. It is also a treatment option for women in Europe, particularly in the case of those with sub‐urethral slings failure [6].
The most widely implanted AUS in Europe and the United States is the AMS800 (Boston Scientific, USA). This is an implantable medical device composed of three parts, including a Pressure‐Regulating Balloon (PRB) which pressurizes the system at a constant pressure. The PRB is selected during the surgery and cannot be changed after implantation. There are 3 different PRBs available on the market, the 61–70 cmH_2_O being the most commonly used.
For many years, different AUS have been imagined and developed with the aim of improving the safety, efficiency, and usability of the current device [7, 8, 9]. The UroActive AUS (UroMems, France) is an implantable device that embeds electronic components and a radiofrequency antenna, enabling it to communicate wirelessly with an external programmer. This feature allows the physician to remote adjust device parameters, including device pressure, even after implantation surgery. UroActive is not approved yet for clinical use, but its biocompatibility and safety have already been tested on large animals [10].
The primary objective of this pre‐clinical study is to evaluate the range of maximal urethral closure pressures (MUCP) achievable by UroActive compared to those of the AMS800 in male and female cadavers. The secondary objective is to assess the correlation between the set pressure and MUCP with the UroActive device.
Methods
2
This study was conducted on fresh cadavers at the Surgical and Anatomical School of the Assistance Publique—Hôpitaux de Paris (FR), following approval by the local ethics committee.
First, an AMS800 OC was implanted using the usual technique: around the bulbar urethra via a perineal approach in males and around the bladder neck via a suprapubic laparotomy in females. OC size was selected using the cuff sizer provided in the AMS800 accessory kit. After being purged with isotonic saline solution, OC was placed around the bulbar urethra/bladder neck and its tubing was routed to the right part of the abdomen. Incisions were closed.
Then, the 3 different AMS800 PRB: 51–60, 61–70, 71–80 cmH_2_O were sequentially connected to the OC with a suture‐tie connector provided in the accessory kit. They were prepared and filled with 20 cc of isotonic saline solution. For each PRB, a Urethral Pressure Profilometry (UPP) was performed using the Goby urodynamic station (Laborie, USA) with a 10Fr 2‐way Bohler urethral catheter.
After these 3 UPPs, AMS800 PRB was replaced by the UroActive Control Unit (CU). The CU is a titanium case (see attached Figure 1) that embeds a fluidic reservoir, an automatic pump, a battery, electronic components, and a radiofrequency antenna allowing it to communicate wirelessly.
UroActive device (a, control unit; b, occlusive cuff). [Color figure can be viewed at wileyonlinelibrary.com]
The CU was previously filled with isotonic saline solution and then connected to the implanted OC with a suture‐tie connector. The CU was placed at the same level as the previous PRBs to minimize the influence of the water column above the OC. After device volume/pressure calibration, pressure was set in the UroActive device to close the cuff and UPP was performed. Multiple UPPs were carried out for CU set pressures ranging from 10 to 150 cmH_2_O, with steps of 10 cmH_2_O.
The endpoint used was the MUCP, defined as the highest pressure measured during UPP.
For the primary objective, the MUCPs achievable by UroActive were compared to those of the AMS800 in male and female cadavers.
For the secondary objective, a Pearson correlation analysis was conducted on male and female cadavers to assess the relationship between the device pressures (PRB specification for AMS800; set CU pressure for UroActive) and MUCPs. Statistical analyses were performed using the XLSTAT software, version 2023.1.1 (Addinsoft, New York, USA).
Results
3
Six cadavers were tested, including 3 males and 3 females.
AMS800 OCs, PRBs, and UroActive CU were implanted without any difficulty. OC sizes were 4, 4, and 4.5 cm for males, and 5, 5, and 5.5 cm for females.
For UroActive device, wireless communication between the CU and the clinician programmer was trouble‐free and device calibration was performed without any difficulty in all cadavers.
Results are represented in Figure 2 for males and Figure 3 for females, and detailed below.
MUCP according to device pressure in male cadavers.
MUCP according to device pressure in female cadavers.
Primary Objective
3.1
For male:
- With the AMS800 PRBs, MUCPs ranged from a minimum value of 56 cmH_2_O with the 51–60 cmH_2_O PRB to a maximum value of 83 cmH_2_O with the 71–80 cmH_2_O PRB.
- Using the UroActive CU, MUCPs ranged from a minimum of 14 cmH_2_O at a set pressure of 10 cmH_2_O to a maximum of 121 cmH_2_O at a set pressure of 150 cmH_2_O.
For female:
- With the AMS800 PRBs, MUCPs ranged from a minimum value of 52 cmH_2_O with the 51–60 cmH_2_O PRB to a maximum value of 75 cmH_2_O with the 71–80 cmH_2_O PRB.
- With the UroActive CU, MUCPs ranged from 18 cmH_2_O at a set pressure of 10 cmH_2_O to a maximum value of 138 cmH_2_O at a set pressure of 150 cmH_2_O.
These MUCP measures show that the UroActive control unit achieved MUCPs that encompass the full range of values obtained with the three AMS800 PRBs for both males and females.
Secondary Objective
3.2
For AMS800:
- The correlation coefficient between the PRB pressure‐specification and MUCPs is r ^2^ = 0.837 for males and r ^2^ = 0.829 for females.
For UroActive:
- The correlation coefficient between the set device pressure send to the UroActive CU and MUCPs is r ^2^ = 0.984 for males and r ^2^ = 0.948 for females. So a strong correlation was observed between UroActive set device pressures and MUCPs in both genders.
Discussion
4
Urodynamic Method
4.1
Urethral occlusion can be assessed using various urodynamic methods, including urethral profilometry and leak point pressures, such as Retrograde Leak Point Pressure (RLPP) and Antegrade Leak Point Pressure (ALPP). During the development of this study's design, we evaluated these methods on cadavers in unpublished pilot studies. The RLPP, measured using the Comiter technique [11], provided highly relevant and reproducible results in male cadavers [12, 13]. However, its use in females was limited by the short length of the urethra, which prevented sufficient catheter positioning away from the OC while maintaining an effective seal. We also tested ALPP measurements with bladder filling through transcutaneous or urethral catheters [14], but reliable and reproducible results could not be achieved. Consequently, we have chosen UPP as the urodynamic reference method in this study. This method has already been used in clinical studies to compare AUS in vivo [15, 16].
Study Design
4.2
The implantation site of the OC differs significantly between males and females, leading to varying tissue properties and thickness inside the cuff (urethra vs. bladder neck). Therefore, we have chosen to separate the results by gender. Moreover, for females, OC sizes appear to be smaller in our study than in current clinical practice. In fact, monocentric series report a median implanted cuff size of 7 cm in women, whether implanted by laparotomy [17] or laparoscopy [18]. This is probably due to the absence of vascularization and tissue atrophy in the cadaveric model. This finding is not expected to affect MUCP measurements.
In this study, only the AMS800 OC was used. Consequently, the evaluation of the UroActive sphincter was conducted with a hybrid system composed of the UroActive CU and the AMS800 OC. This approach was chosen to limit potential biases related to changes in OC positioning, allowing us to focus solely on comparing the device pressurization systems: BRPs for the AMS800 versus CU for UroActive.
We limited the study to a maximum device pressure of 150 cmH_2_O with UroActive, in line with its technical specifications, as we believe that applying higher pressures in clinical practice could carry a significant risk of erosion. To balance precision and practicality, we increased the pressure in increments of 10 cmH_2_O, though finer adjustments are technically possible.
UroActive Device
4.3
UroActive is composed of an electromechanical CU connected to a hydraulic OC that adopts the same circumferential occlusion mechanism as the AMS 800. It's a crucial consideration when comparing artificial urinary sphincters. Indeed, the mechanism by which urethral compression is applied directly influences both the closure pressure generated and its distribution along the urethral wall. As demonstrated by Marziale et al., circumferential occlusion provides a distinct sealing behavior compared to clamping systems, particularly within the physiological pressure range of the lower urinary tract. These findings were supported by finite element modeling and validated through benchtop experimentation using urethral phantoms, allowing precise comparison between occlusion strategies [19]. The biomechanical behavior of the urethra under various occlusive loads had previously been characterized in detail through numerical modeling approaches, which served as the foundation for this comparative analysis [20].
UroActive Expected Benefits
4.4
As mentioned in the introduction, the occlusion pressure applied by the AMS800 cuff to the urethra is determined at implantation by the choice of BRP. Urethral occlusion pressure is therefore continuous and non‐modifiable after device activation.
UroActive is an electronic device which embeds automatic functions and can be controlled remotely by the patient via a remote control and configured by the physician via an external clinician programmer. Thus, device pressure could be changed during the day according to patient needs and could be adjusted by the physician during follow‐up visits according to patient continence satisfaction. Lowering the occlusive pressure during phases of low activity, patient sleep for example, could lead to urethral preservation. In a 2001 study conducted between the Mayo Clinic (Rochester, Minnesota, USA) and Baylor (Waco, Texas, USA), Elliott et al. show that nocturnal deactivation of the AMS800 could decrease the risk of urethral atrophy and urinary incontinence, although these results were not statistically significant [21].
The expected benefits of these features are to improve therapy effectiveness while decreasing device revision or explantation rate.
Conclusions
5
UroActive is a new electronic AUS which can be remotely controlled, so that the urethral occlusive pressure can be changed during the day and adjusted to the level of continence, even after device implantation and activation.
This pre‐clinical study demonstrates that the MUCPs achieved with UroActive are across a range that encompasses the values provided by the AMS800 PRBs for both male and female cadavers. Additionally, the strong positive correlation between set device pressures and MUCP observed with UroActive underscores its precise pressure control capabilities.
This study suggests that the UroActive AUS has the potential to offer a new adjustable option for managing stress urinary incontinence, with remote control capabilities that may enhance patient outcomes.
Author Contributions
All authors participated, according to their personnal skills, in the protocol development, the study achievement, the data analysis and the writing of the manuscript. No AI was used.
Conflicts of Interest
Pierre Mozer is co‐founder of Uromems. Aurelien Beaugerie and Emmanuel Chartier‐Kastler are consultants for Uromems.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1V. Ficarra , G. Novara , R. C. Rosen , et al., “Systematic Review and Meta‐Analysis of Studies Reporting Urinary Continence Recovery After Robot‐Assisted Radical Prostatectomy,” European Urology 62 (2012): 405–417.22749852 10.1016/j.eururo.2012.05.045 · doi ↗ · pubmed ↗
- 2M. Abufaraj , T. Xu , C. Cao , et al., “Prevalence and Trends in Urinary Incontinence Among Women in the United States, 2005‐2018,” American Journal of Obstetrics and Gynecology 225 (2021): 166.e 1–166.e 12.10.1016/j.ajog.2021.03.01633727114 · doi ↗ · pubmed ↗
- 3S. Caruso , R. Brescia , M. G. Matarazzo , G. Giunta , A. M. C. Rapisarda , and A. Cianci , “Effects of Urinary Incontinence Subtypes on Women's Sexual Function and Quality of Life,” Urology 108 (2017): 59–64.28652167 10.1016/j.urology.2017.06.025 · doi ↗ · pubmed ↗
- 4B. N. Breyer , S. K. Kim , E. Kirkby , A. Marianes , A. J. Vanni , and O. L. Westney , “Updates to Incontinence After Prostate Treatment: AUA/GURS/SUFU Guideline (2024),” Journal of Urology 212 (2024): 531–538.38934789 10.1097/JU.0000000000004088 · doi ↗ · pubmed ↗
- 5M. Gacci , V. I. Sakalis , M. Karavitakis , et al., “European Association of Urology Guidelines on Male Urinary Incontinence,” European Urology 82 (2022): 387–398.35697561 10.1016/j.eururo.2022.05.012 · doi ↗ · pubmed ↗
- 6A. K. Nambiar , S. Arlandis , K. Bø , et al., “European Association of Urology Guidelines on the Diagnosis and Management of Female Non‐Neurogenic Lower Urinary Tract Symptoms. Part 1: Diagnostics, Overactive Bladder, Stress Urinary Incontinence, and Mixed Urinary Incontinence,” European Urology 82 (2022): 49–59.35216856 10.1016/j.eururo.2022.01.045 · doi ↗ · pubmed ↗
- 7L. Marziale , G. Lucarini , T. Mazzocchi , et al., “Artificial Sphincters to Manage Urinary Incontinence: A Review,” Artificial Organs 42 (2018): E 215–E 233.30074617 10.1111/aor.13164 · doi ↗ · pubmed ↗
- 8M. Wang , Y. Liao , Y. Liu , W. Zhou , and H. Yu , “Development and Future Prospects of the Artificial Urinary Sphincter,” Artificial Organs 47 (2023): 1688–1699.37424277 10.1111/aor.14606 · doi ↗ · pubmed ↗