Severe Congenital Pulmonary Valve Stenosis Diagnosed in Adulthood: A Case Report
Mehdi Moujahid, Hafsa Erregui, Najat Mouine, Zouhair Lakhal, Aatif Benyass

TL;DR
A 21-year-old adult was diagnosed with a rare heart condition called pulmonary valve stenosis, typically found in children, after experiencing breathing difficulties and chest pain.
Contribution
This case report highlights the rare presentation of congenital pulmonary valve stenosis in adulthood and the challenges of diagnosing and treating it in resource-limited settings.
Findings
Severe pulmonary valve stenosis was diagnosed in a 21-year-old with exertional dyspnea and chest pain.
Transthoracic echocardiography revealed a peak velocity of 4.53 m/s and a systolic gradient of 82.23 mmHg.
Balloon pulmonary valvuloplasty was recommended following diagnostic imaging and multidisciplinary evaluation.
Abstract
Pulmonary valve stenosis is a congenital heart disease that is usually diagnosed during childhood, while presentation in adulthood is uncommon and may lead to delayed diagnosis. We report the case of a 21-year-old patient with no significant medical history who presented with a six-month history of exertional dyspnea and constrictive chest pain. Electrocardiography showed right axis deviation with signs of right ventricular hypertrophy, and chest radiography revealed dilatation of the left pulmonary artery. Transthoracic echocardiography demonstrated severe valvular pulmonary stenosis with a peak velocity of 4.53 m/s and a maximum systolic gradient of 82.23 mmHg, associated with right ventricular hypertrophy and preserved systolic function, without evidence of pulmonary hypertension. Computed tomography pulmonary angiography confirmed focal post-stenotic dilatation of the left pulmonary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
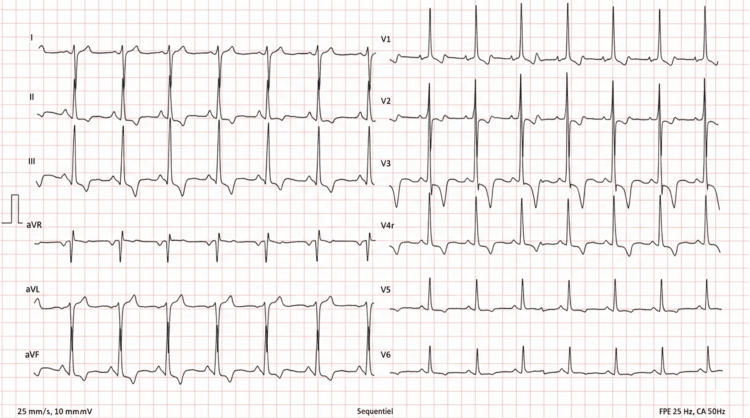 Figure 1
Figure 1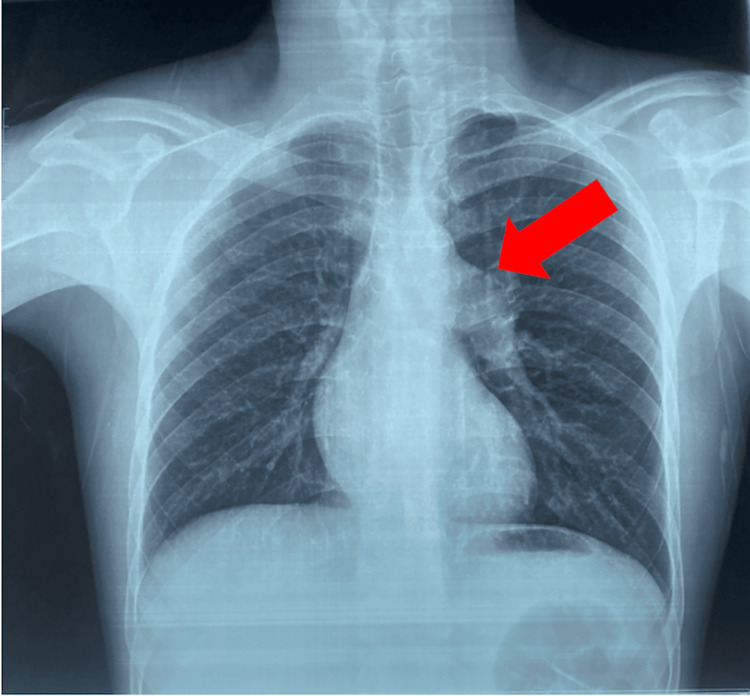 Figure 2
Figure 2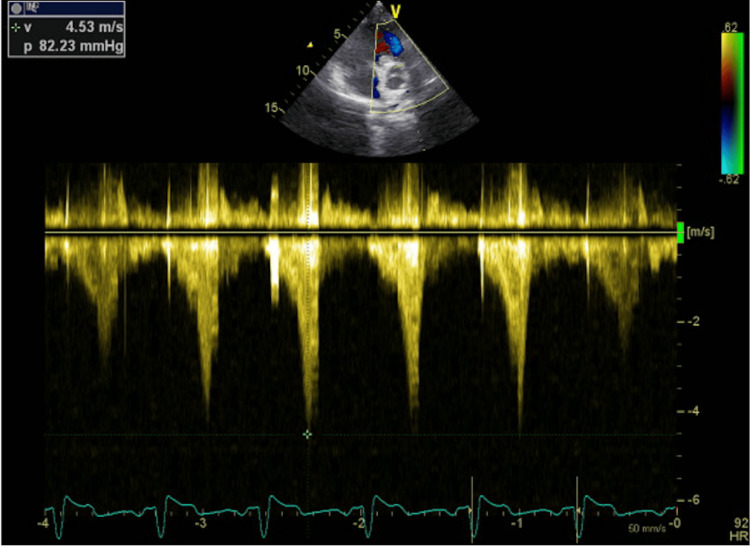 Figure 3
Figure 3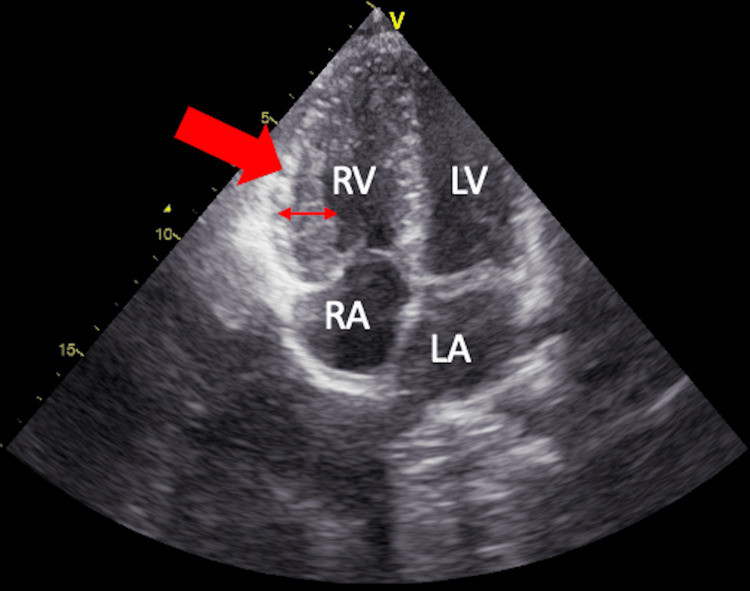 Figure 4
Figure 4 Figure 5
Figure 5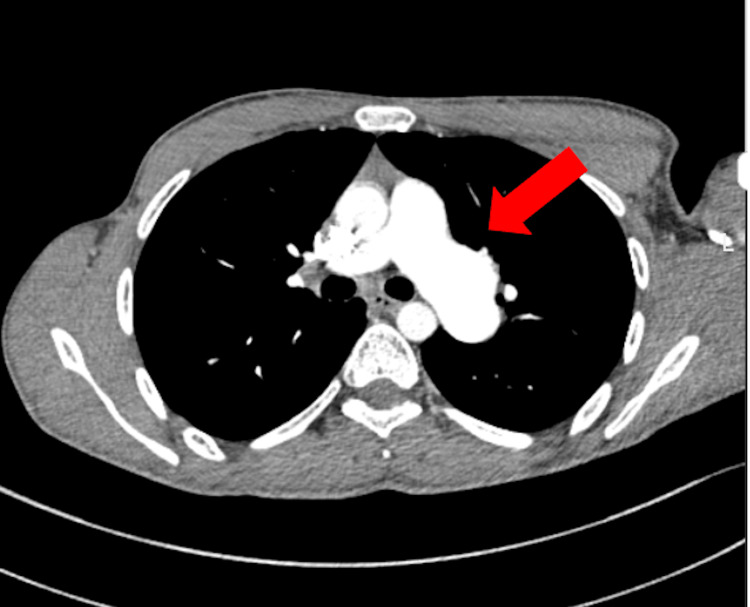 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Cardiac Valve Diseases and Treatments · Congenital heart defects research
Introduction
Congenital pulmonary valve stenosis is a well-recognized congenital heart disease most commonly diagnosed during infancy or childhood, as significant obstruction usually leads to early clinical manifestations. However, mild or moderate forms may remain asymptomatic for years, allowing the condition to go unrecognized until adulthood [1,2].
Congenital heart disease affects approximately 1% of live births, and advances in pediatric cardiology and cardiac surgery have resulted in a growing population of adults living with congenital heart disease (ACHD) [3]. In this population, some congenital lesions, including pulmonary valve stenosis, may present later in life or remain undiagnosed until adulthood.
In adults, pulmonary valve stenosis may be discovered during evaluation for exertional dyspnea, chest pain, or abnormal cardiac findings. Delayed diagnosis can result in progressive right ventricular pressure overload, leading to right ventricular hypertrophy, reduced exercise tolerance, and post-stenotic dilatation of the pulmonary artery. Transthoracic echocardiography (TTE) remains the cornerstone of diagnosis and follow-up, enabling assessment of stenosis severity, right ventricular remodeling, and associated cardiac abnormalities [1-3].
We report a case of severe congenital valvular pulmonary stenosis diagnosed in a young adult, highlighting the diagnostic features, imaging findings, and therapeutic considerations, as well as challenges related to access to interventional treatment in resource-limited settings.
Case presentation
A 21-year-old male patient with no significant past medical history presented with a six-month history of exertional dyspnea (New York Heart Association class II) associated with constrictive chest pain on exertion, occurring even with minimal physical activity. There was no history of syncope, palpitations, or cardiovascular risk factors.
On physical examination, the patient was hemodynamically stable, with a blood pressure of 120/70 mmHg, heart rate of 78 beats per minute, and oxygen saturation of 98% on room air. There was no cyanosis and no digital clubbing. Jugular venous pressure was normal. Cardiac auscultation revealed a systolic ejection murmur best heard at the left upper sternal border. Lung auscultation was normal, and no peripheral edema was noted. Routine laboratory tests were within normal limits, including complete blood count, renal function, and electrolytes. Cardiac biomarkers, including troponin and B-type natriuretic peptide (BNP), were not elevated. Electrocardiography demonstrated right axis deviation with features consistent with right ventricular hypertrophy (Figure 1).
Electrocardiographic Findings in Severe Pulmonary Valve StenosisTwelve-lead electrocardiogram showing right axis deviation and features consistent with right ventricular hypertrophy, including tall R waves in the right precordial leads and deep S waves in the lateral leads. These findings reflect chronic right ventricular pressure overload secondary to severe pulmonary valve stenosis.
Chest radiography showed a prominent left pulmonary artery segment without pulmonary congestion (Figure 2).
Posteroanterior Chest Radiograph Showing Left Pulmonary Artery DilatationA prominent left pulmonary artery segment (red arrow) is seen, consistent with post-stenotic pulmonary artery dilatation in the setting of severe pulmonary valve stenosis. No signs of pulmonary congestion are observed.
TTE revealed severe valvular pulmonary stenosis with a peak velocity of 4.53 m/s and a maximum systolic gradient of 82.23 mmHg across the pulmonary valve (Figure 3). The right ventricle was hypertrophied with preserved systolic function (Figure 4). No other significant valvular abnormalities were identified, and there were no echocardiographic findings suggestive of pulmonary hypertension.
Continuous-Wave Doppler Echocardiography Demonstrating Severe Pulmonary Valve Stenosis.A markedly increased transvalvular flow velocity is seen, with a peak velocity of 4.53 m/s and a maximum systolic gradient of 82.23 mmHg, consistent with severe pulmonary valve stenosis. The Doppler profile reflects significant right ventricular outflow tract obstruction.
Apical Four-Chamber TTE Showing Right Ventricular HypertrophyRight ventricular hypertrophy (red arrow) is seen with preserved cavity size. The left-sided cardiac chambers appear normal. These findings reflect chronic right ventricular pressure overload secondary to severe pulmonary valve stenosis.RV: right ventricle; LV: left ventricle; RA: right atrium; LA: left atrium; TTE: transthoracic echocardiography
Computed tomography pulmonary angiography (CTPA) demonstrated focal dilatation of the left pulmonary artery without evidence of pulmonary embolism, supporting post-stenotic pulmonary artery dilatation (Figures 5, 6). Differential diagnoses such as pulmonary embolism, subvalvular obstruction, and other causes of right ventricular outflow tract obstruction were considered and excluded based on echocardiographic and computed tomography findings
Sagittal CTPA Showing Post-Stenotic Dilatation of the Left Pulmonary ArteryMarked dilatation of the left pulmonary artery (red arrow) is seen, consistent with post-stenotic pulmonary artery dilatation secondary to severe pulmonary valve stenosis. No evidence of pulmonary embolism or associated aortic coarctation is observed.CRPA: computed tomography pulmonary angiography
Axial CTPA Showing Left Pulmonary Artery DilatationMarked dilatation of the left pulmonary artery (red arrow) is seen, consistent with post-stenotic pulmonary artery dilatation in the setting of severe pulmonary valve stenosis. No intraluminal filling defects suggestive of pulmonary embolism are observed.CTPA: computed tomography pulmonary angiography
Following a multidisciplinary medico-surgical discussion, balloon pulmonary valvuloplasty was recommended. However, as this procedure was not available at our institution, the patient was referred to a center abroad where the intervention was performed. At the time of writing the report, post-intervention outcomes were not yet available.
Discussion
Pulmonary valve stenosis is most commonly congenital and typically results from commissural fusion, leaflet thickening, or valve dysplasia. The severity of obstruction determines the timing of presentation. While severe forms usually manifest early in life, delayed presentation in adulthood may occur in patients with slowly progressive disease or good right ventricular adaptation [1,2]. In adults, congenital heart disease may remain asymptomatic for many years or be incidentally detected, with clinical presentation largely depending on the severity of the underlying lesion [3].
In adults, symptoms such as exertional dyspnea, chest pain, or syncope reflect the limited ability of the pressure-loaded right ventricle to increase cardiac output during exertion. Electrocardiographic findings often include right axis deviation and signs of right ventricular hypertrophy, as observed in our patient. Chest radiography may show post-stenotic dilatation of the pulmonary artery, a supportive feature in the appropriate clinical context [2].
TTE is the first-line imaging modality for diagnosis and severity assessment. Current guideline-based thresholds classify pulmonary valve stenosis as severe when the peak transvalvular velocity exceeds 4.0 m/s or the peak systolic gradient is greater than 50 mmHg. In our case, the measured peak velocity of 4.53 m/s and gradient of 82.23 mmHg clearly indicated severe stenosis, associated with right ventricular hypertrophy but preserved systolic function and no evidence of pulmonary hypertension. CTPA supported the diagnosis by demonstrating focal post-stenotic dilatation of the left pulmonary artery and excluding pulmonary embolism [3,4].
Management of severe pulmonary valve stenosis depends on symptom status, stenosis severity, and valve morphology. Percutaneous balloon pulmonary valvuloplasty is considered the preferred treatment for symptomatic patients with severe valvular stenosis and favorable anatomy because of high success rates and acceptable safety. According to current European Society of Cardiology (ESC) guidelines for adult congenital heart disease, balloon pulmonary valvuloplasty is recommended as first-line therapy for symptomatic severe valvular pulmonary stenosis (Class I recommendation), with procedural success rates exceeding 90% in suitable valve anatomy. Surgical intervention is generally reserved for patients with dysplastic valves, associated subvalvular or supravalvular obstruction, or when percutaneous treatment is not feasible [2,3,5,6].
In the present case, a multidisciplinary heart team recommended balloon pulmonary valvuloplasty. However, the lack of local availability of this technique required referral abroad, illustrating real-world barriers to guideline-directed care in resource-limited settings. At the time of publication, post-procedural outcomes were not available.
This case emphasizes the importance of considering congenital heart disease in young adults with exertional symptoms and highlights the central role of echocardiography in diagnosis and management planning. Early recognition and timely intervention are essential to prevent long-term right ventricular dysfunction and improve functional status.
Conclusions
Severe congenital pulmonary valve stenosis may remain clinically silent until adulthood and should be considered in young adults presenting with exertional symptoms. TTE plays a pivotal role in establishing the diagnosis, assessing severity, and guiding management. Balloon pulmonary valvuloplasty is the treatment of choice for symptomatic severe valvular stenosis when feasible. This case highlights the importance of early recognition and the challenges of access to advanced interventional therapies in resource-limited settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Task force 1: The changing profile of congenital heart disease in adult life J Am Coll Cardiol Warnes CA Liberthson R Danielson GK 117011753720011130041810.1016/s 0735-1097(01)01272-4 · doi ↗ · pubmed ↗
- 2Congenital heart disease in adults. First of two parts N Engl J Med Brickner ME Hillis LD Lange RA 25626334220001064876910.1056/NEJM 200001273420407 · doi ↗ · pubmed ↗
- 32020 ESC guidelines for the management of adult congenital heart disease Eur Heart J Baumgartner H De Backer J Babu-Narayan SV 5636454220213286002810.1093/eurheartj/ehaa 554 · doi ↗ · pubmed ↗
- 42020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines Circulation Otto CM Nishimura RA Bonow RO 0143202110.1161/CIR.000000000000092333332150 · doi ↗ · pubmed ↗
- 5Percutaneous balloon pulmonary valvuloplasty: state of the art Catheter Cardiovasc Interv Rao PS 7477636920071733027010.1002/ccd.20982 · doi ↗ · pubmed ↗
- 6Long-term results after balloon pulmonary valvuloplasty Circulation Mc Crindle BW Kan JS 19151922831991204004410.1161/01.cir.83.6.1915 · doi ↗ · pubmed ↗