Adult embryonal rhabdomyosarcoma (botryoid subtype) of the ureter: A case report
Logan Wesemann, Douglas Fair, Kenil Mehta, Glen A. Lau

TL;DR
A rare case of adult embryonal rhabdomyosarcoma in the ureter is reported, with successful treatment and remission.
Contribution
This case report adds to the limited literature on ureteral embryonal rhabdomyosarcoma and its management.
Findings
The patient achieved remission after surgical resection and chemotherapy.
Long-term surveillance is emphasized for monitoring recurrence and complications.
Abstract
Embryonal rhabdomyosarcoma arising from the ureter is exceedingly rare. We report the case of a 20-year-old female who presented with flank pain and hematuria, initially attributed to ureteral stones. Subsequent evaluation revealed an embryonal rhabdomyosarcoma (botryoid subtype) of the ureter. Following surgical resection and chemotherapy, the patient achieved remission and experienced minor complications including neuropathy and bladder irritation. This case highlights the classification and management of ureteral rhabdomyosarcoma. While the prognosis for ureteral rhabdomyosarcoma appears favorable based on limited literature, long-term surveillance is crucial for monitoring recurrence and managing potential complications.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
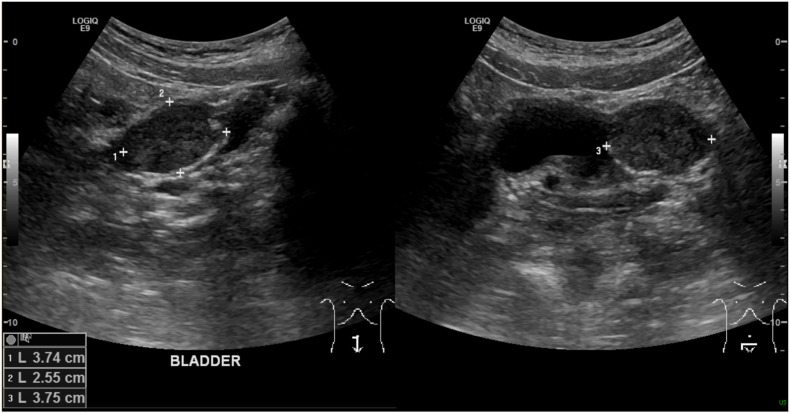 Figure 1
Figure 1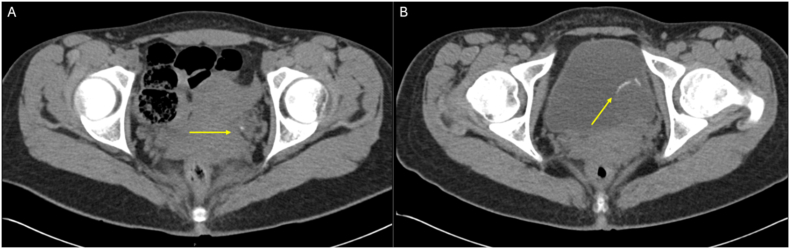 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Teratomas and Epidermoid Cysts · Uterine Myomas and Treatments
Background
1
Rhabdomyosarcoma (RMS) is a malignant soft tissue tumor characterized by the presence of skeletal muscle differentiation, predominantly diagnosed in children and adolescents. It is the most common soft tissue sarcoma in the pediatric population, representing roughly 50% of pediatric soft tissue sarcomas. In adolescents and young adults, it is less common, representing less than 10% of the soft tissue sarcomas in this group1, 2, 3. Rhabdomyosarcoma is classified into several histological and molecular subtypes, with the major categories being embryonal, alveolar, spindle cell/sclerosing, and pleomorphic rhabdomyosarcoma. Embryonal rhabdomyosarcoma is associated with the lack of a poor prognostic translocation (PAX 3/7-FOXO1). One subtype of embryonal rhabdomyosarcoma is a botryoid variant which is characterized as “grapelike” polypoid masses with predilection for mucosa-lined, hollow organs such as vagina, bladder, cervix, and, more rarely, the biliary tract and ear1, 2, 3, 4, 5, 6, 7. And while embryonal rhabdomyosarcoma of the genitourinary tract is not uncommon,8 rhabdomyosarcoma arising from the ureter is extremely rare, with only a few isolated cases reported in the literature9, 10, 11. We present the case and outcome of a 20-year-old female with embryonal botryoid rhabdomyosarcoma of the ureter, including the presentation, management and long-term outcome after treatment.
Case presentation
2
Initial presentation and diagnostic evaluation
2.1
A 20-year-old Caucasian female presented to the emergency department with intermittent left-sided flank pain, hematuria, urinary frequency, and urgency. Initial CT revealed distal left ureteral calcifications with hydronephrosis. Presuming this was a ureteral stone, she was given medical expulsive therapy and discharged home. Two months later, she returned with similar symptoms in addition to left lower quadrant abdominal pain. She reported increased pain and nausea compared to her previous encounter, in addition to passage of large blood clots in her urine over the previous two days. Shown in Fig. 1, a Bladder ultrasound showed hydroureter and a mass measuring 3.8 x 3.7 x 2.6 cm, initially perceived as a thrombus, prompting a repeat CT scan. The repeat CT revealed worsened left-sided hydronephrosis and a new hypoechoic, well-defined ovoid lesion to the left of the bladder with internal calcifications, which was thought to possibly represent a ureterocele. The distal ureter could not be visualized. Fig. 2 shows comparative CT imaging demonstrating significant progression in tumor size with increased calcifications. As the definitive characteristics of the mass could not be established, cystoscopy was performed.Fig. 1. Legend: Transabdominal bladder ultrasonography demonstrating a well-defined, heterogeneous mass measuring 3.8 x 3.7 × 2.6 cm is noted at the left ureterovesical junction. The lesion was initially suspicious for an intravesical thrombus. Associated left-sided hydroureter is visualized superior to the mass.Fig. 1. Fig. 2Legend: (A) Initial axial CT scan of abdomen and pelvis without contrast demonstrated moderate hydroureter tapering to a focal calcification in the distal ureter, originally interpreted as an obstructing calculus. (B) Follow-up CT scan without contrast at two months demonstrating progression of a heterogeneous mass. Note the presence of internal macroscopic fat and peripheral calcifications, suggestive of the osseous components within the botryoid rhabdomyosarcoma.Fig. 2
Cystoscopy revealed a non-cystic, non-penetrable lesion arising from the left ureteral orifice, with no evidence of a ureterocele. A retrograde pyelogram showed the distal 6 cm of the ureter filled with tumor. A biopsy was performed, and a ureteral stent was placed to maintain patency in anticipation of a subsequent surgical resection.
Histologic findings
2.2
Histologic analysis of the biopsy revealed spindle cell stromal proliferation with cells showing scant cytoplasm, nuclear enlargement, and increased mitotic activity, indicating a malignant process. The immunohistochemical stains for Desmin and Myogenin were positive for both markers. PAX3/7-FOXO1 testing was negative. Taken together, the diagnosis of embryonal rhabdomyosarcoma, botryoid subtype, was rendered. Margins were positive for tumor. A staging CT scan of the chest showed no evidence of metastasis.
In North America, pediatric rhabdomyosarcoma guidelines rely on the Children's Oncology Group (COG) risk stratification. This is based on a combination of TNM Pre-Treatment Staging Classification and Clinical Grouping Classification, and more recently histological subtype and/or FOXO1 fusion status and age at diagnosis for Risk Stratification.12 Under the TNM system (based on primary tumor site, size, regional lymph node status and distant metastatic involvement), the ureter is not explicitly categorized. Localized tumors that are less than 5 cm and lymph node negative are either Stage 1 or Stage 2 based on location of tumor. Genitourinary (GU) tumors that are not arising from the bladder or prostate are Stage 1 and GU tumors arising from the bladder or prostate are Stage 2^12^.
Therapeutic intervention and risk stratification
2.3
Following multidisciplinary review, the patient underwent robotic distal ureterectomy (7 cm excision with a bladder cuff), pelvic lymph node dissection, and psoas hitch ureteroneocystostomy. A mid-ureteral psoas hitch and peritoneal flap for bladder closure reinforcement were utilized to ensure a tension-free anastomosis. Pathology of resected ureter confirmed a small (<5 cm) embryonal rhabdomyosarcoma (RMS), botryoid subtype, with R0 negative margins and no nodal involvement (T1aN0M0). Based on the complete resection of the localized disease in an R0 manner before starting chemotherapy, and its proximity to bladder, the patient was classified as Stage 2, Clinical Group I.
Postoperatively, imaging confirmed no evidence of disease or anastomotic leak. After fertility preservation (embryo cryopreservation with her partner), the patient received 14 cycles of chemotherapy, which were alternating cycles of VAC (Vincristine, Dactinomycin, and Cyclophosphamide) with VI (Vincristine and Irinotecan) of adjuvant therapy according to COG protocol ARST1431 Arm A (no maintenance therapy). We did not include radiation for local control because of the R0, negative resection, Clinical Group I status. The patient tolerated the therapy well, experiencing mild flank pain and mild reversible neuropathy during therapy. After completion of therapy, the patient was surveyed with MRI of the abdomen and pelvis and CXR every 3 months for the first two years off of therapy, and then every six months from years three to five. The patient is now greater than 5 years post-therapy and remains disease-free.
Discussion
3
This report is unique for several reasons. The number of currently reported cases is three; thus, this case adds to the limited understanding of the presentation, clinical course, and treatment of ureteral RMS, highlighting the rarity of this diagnosis. In contrast to previously reported cases9, 10, 11—where patients neither exhibited early ureteral stone symptoms nor had a significant history of nephrolithiasis—our patient presented with renal colic and concern for obstructing ureteral calculi. This presentation likely indicates early ureteral obstruction due to tumor involvement of the distal ureteral wall, either with calcifications in the tumor or small ureteral stones, whose passage was impeded by the tumor. The absence of similar findings in earlier cases underscores the unique diagnostic challenge posed by our patient's presentation.
Across all reported cases, including ours, common symptoms mimicked those of ureteral obstruction, including flank pain, nausea, vomiting, and hematuria (see Table 1). Imaging consistently revealed hydronephrosis and/or hydroureter, underscoring the importance of maintaining a broad differential diagnosis in young patients with persistent obstructive uropathy and atypical presentations.Table 1. Summary of previously reported ureteral rhabdomyosarcomas and our case.Table 1. Case yearAgeSexClinical SymptomsImaging Findings (side)StagingTreatmentDisease StatusLearning Points199919FFlank pain, nausea, vomitingHydronephrosis (R)T2aN0M0 CG ISurgical resection, Chemotherapy, and radiationDisease-free 3 years post treatmentMultimodal therapy increases 5-year survival20084FNot discussedHydronephrosis (L)T2aN0M0 CG IIIChemotherapy, radiation, followed by surgical resectionNot discussedConsider initial chemotherapy or radiation to shrink tumor (12 weeks)202329FFlank pain, hematuria, hypertensionHydronephrosis, hydroureter (R)T2aN0M0 CG IChemotherapy followed by surgical resectionDisease-free 18 months post treatmentSurgery and chemotherapy are effective for adult patientsOngoing post-treatment surveillance is crucial2025 (this case)20FFlank pain, hematuria, frequency, urgencyHydronephrosis, hydroureter (L)*T2aN0M0 *CG ISurgical resection followed by chemotherapyDisease-free 4-years post treatmentUreteral RMS may be a favorable site**Establishing formal criteria for ureter may help better risk stratify in the futureAll embryonal botryoid subtype cases currently reported in literature, including our case. CG = Clinical Group.
Our patient did well following surgical resection and chemotherapy, apart from occasional bladder irritation episodes and chemotherapy-induced neuropathic symptoms. All cases appear to have resulted in the successful treatment of the disease, although the long-term sequelae of ureteral RMS has not been described in the literature. Interestingly, all four documented cases have occurred in female patients.
Diagnosis and treatment of ureteral RMS
3.1
Following biopsy, assessment of suspected RMS should include axial imaging for staging and group assignment (after initial surgery resection) and with histological and/or molecular testing, Risk assessment should be made, which can guide chemotherapy and other adjuvant therapy. Further management described in the literature emphasizes multimodal therapy, but the sequence of this is variable in the described cases.
One case of an adult female who presented with one week of constant, dull, right flank pain, associated with intermittent nausea and vomiting. CT urography showed right hydronephrosis as well as a distal ureter filling defect. Biopsy revealed the definitive diagnosis of embryonal RMS botryoid subtype. They performed a nephroureterectomy due to possible tumor seeding from previously stenting the patient. They concluded by mentioning the value of multimodal therapy to increase the 5-year survival rate in patients with RMS.9
The next case involved a 29-year-old pregnant female who presented with right flank pain, hematuria, and hypertension with a urinalysis positive for blood and leukocytes and a significant past medical history of kidney stones. Ultrasound imaging discovered unilateral right hydronephrosis and right hydroureter. Post-partum, the patient's symptoms persisted, after which a CT urogram revealed a thick-walled enhancing segment of the right proximal ureter, which proved to be RMS. After initial chemotherapy, the distal ureterectomy was performed. The authors concluded that surgical intervention and chemotherapy are effective treatment options for patients in this category and should be followed by ongoing post-treatment surveillance for oncologic control.10
The last case involved a 4-year-old female with a larger 8.0 x 4.0 x 2.0 cm RMS initially thought to be originating at the bladder trigone. Biopsy showed a botryoid subtype of RMS. The patient was first treated with chemotherapy and radiation (likely due to larger tumor size), after which the tumor was grossly resected. Gross resection revealed positive margins at the ureter and vagina. They concluded by describing the use of tumor, node, metastasis (TNM) staging to determine proper diagnosis and treatment.11
Surgical approach and technique consideration
3.2
In this case, a distal ureterectomy with a psoas-hitch ureteroneocystostomy was performed to achieve a tension-free anastomosis. Minimizing tension is fundamental to optimizing healing and reducing the risk of stricture or anastomotic failure.13 For distal defects, bladder mobilization with or without a psoas hitch facilitates this objective by reducing the distance between the viable ureteral stump and the bladder. When this mobilization is insufficient to achieve a tension-free repair, a Boari flap can be employed as an adjunct technique.14 For more proximal or extensive ureteral loss, options include transureteroureterostomy or ileal ureter substitution, while mid-ureteral lesions may require a Boari flap with psoas hitch. Regardless of technique, the primary goal is a tension-free, well-vascularized anastomosis.15
Ureteral rhabdomyosarcoma classification
3.3
The classification and treatment of ureteral RMS remain poorly defined in the literature, particularly when compared to other genitourinary (GU) tumors such as bladder and prostate RMS. Molecular markers, such as FOXO1 fusion status, play a crucial role in defining prognosis across all RMS cases. In the case of our young adult female patient, her negative FOXO1 fusion status–a marker typically associated with better outcomes–aligned with her favorable response to treatment. Negative fusion status is increasingly recognized as a prognostic marker, helping to stratify patients into low, intermediate, or high-risk groups, which informs treatment decisions. However, the absence of specific guidance for ureteral RMS presents challenges in how best to incorporate molecular profiling into personalized care.
Additionally, ureteral RMS presents unique challenges in surgical management due to the ureter's proximity to other important structures. Therefore, similar management strategies must be adapted for ureteral tumors, particularly when procedures such as ureteral reimplantation are required. These procedures raise the complexity of treatment and necessitate careful planning to preserve function while ensuring complete tumor resection. Developing a more refined classification for ureteral RMS that acknowledges these surgical challenges will be essential in future guidelines.
Another key issue is the lack of consensus on whether ureteral RMS arises from a "favorable" or "unfavorable" site. The lack of a standardized classification for ureteral rhabdomyosarcoma (RMS) complicates the development of a unified treatment approach. However, excluding one pediatric case with unknown follow-up, reported cases, including ours, demonstrate favorable outcomes. This trend likely reflects early detection, as symptomatic ureteral obstruction from even minimal tumor growth may be prompting clinical evaluation before distant metastasis. This consistent pattern suggests that ureteral RMS might be considered a favorable site. Establishing formal criteria to define ureteral RMS as arising from either a favorable or unfavorable site could improve future risk stratification and guide management decisions.
Conclusion
4
This case highlights the diagnostic challenges of ureteral botryoid rhabdomyosarcoma, a rare malignancy that often mimics common obstructive uropathy. Our patient's five-year disease-free survival underscores the efficacy of multimodal therapy combining radical resection with risk-adapted chemotherapy. However, the lack of a standardized COG classification for the ureter remains a significant gap in oncologic frameworks. Given the favorable outcomes reported here and in existing literature, we propose formalizing the ureter as a "favorable" primary site. Ultimately, a high index of suspicion for atypical obstructive symptoms in young patients is essential for early detection and the refinement of future risk-stratification protocols is warranted.
CRediT authorship contribution statement
Logan Wesemann: Writing – review & editing, Writing – original draft, Methodology, Investigation, Conceptualization. Douglas Fair: Writing – review & editing, Writing – original draft, Validation, Supervision. Kenil Mehta: Writing – review & editing, Writing – original draft, Investigation. Glen A. Lau: Writing – review & editing, Writing – original draft, Validation, Supervision.
Funding
Funding was provided by Rocky Vista University College of Osteopathic Medicine, 255 E Center St, Ivins, UT, 84738, USA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kaseb H.Kuhn J.Babiker H.M.Rhabdomyosarcoma Statpearls 2024 Stat Pearls Publishinghttp://www.ncbi.nlm.nih.gov/books/NBK 507721/
- 2Neha B.Manjunath A.P.Girija S.Pratap K.Botryoid rhabdomyosarcoma of the cervix: case report with review of the literature Sultan Qaboos University Medical Journal 1532015 e 43310.18295/squmj.2015.15.03.022PMC 455428326357564 · doi ↗ · pubmed ↗
- 3Mc Evoy M.T.Siegel D.A.Dai S.Pediatric rhabdomyosarcoma incidence and survival in the United States: an assessment of 5656 cases, 2001-2017 Cancer Med 1232023 Feb 3644365610.1002/cam 4.5211 Epub 2022 Sep 7. PMID: 36069287; PMCID: PMC 993920536069287 PMC 9939205 · doi ↗ · pubmed ↗
- 4Parham D.M.Barr F.G.Classification of rhabdomyosarcoma and its molecular basis Adv Anat Pathol 2062013 Nov 38739710.1097/PAP.0b 013e 3182 a 92d 0d PMID: 24113309; PMCID: PMC 663794924113309 PMC 6637949 · doi ↗ · pubmed ↗
- 5Chen J.Liu X.Lan J.Rhabdomyosarcoma in adults: case series and literature review Int J Wom Health 14202240541410.2147/IJWH.S 352143 PMC 897368835370426 · doi ↗ · pubmed ↗
- 6Sharma A.E.Dermawan J.K.Chiang S.Wexler L.H.Antonescu C.R.Botryoid-type embryonal rhabdomyosarcoma: a comprehensive clinicopathologic and molecular appraisal with cross-comparison to its conventional-type counterpart Am J Surg Pathol 2024 Aug 3010.1097/PAS.000000000000230010.1097/PAS.0000000000002300. Epub ahead of print. PMID: 39210566; PMCID: PMC 12117734 PMC 1211773439210566 · doi ↗ · pubmed ↗
- 7Liu L.D.Peng F.Zheng S.Chen R.Xiao B.Qiao J.Y.A case report of pediatric biliary botryoid rhabdomyosarcoma J Clin Ultrasound 5252024 Jun 63563710.1002/jcu.23676 Epub 2024 Mar 26. PMID: 3853265338532653 · doi ↗ · pubmed ↗
- 8Castle J.T.Levy B.E.Allison D.B.Rodeberg D.A.Rellinger E.J.Pediatric rhabdomyosarcomas of the genitourinary tract Cancers (Basel)15102023 May 22286410.3390/cancers 15102864 PMID: 37345202; PMCID: PMC 1021613437345202 PMC 10216134 · doi ↗ · pubmed ↗