Likelihood of Dupuytren Contracture Recurrence After Limited Fasciectomy, Needle Aponeurotomy or Collagenase Clostridium histolyticum: Systematic Review of Prospective Data With 2- to 7-Year Follow-up
Michael Nocek, Dorothy Wakefield, Mark A. Vitale

TL;DR
This study compares the long-term effectiveness of three treatments for Dupuytren contracture, finding that limited fasciectomy has the lowest recurrence rate.
Contribution
The paper provides a systematic review of prospective data comparing recurrence rates of Dupuytren contracture treatments over 2-7 years.
Findings
Limited fasciectomy had the lowest recurrence rate (16.5%) compared to collagenase (32.5%) and needle aponeurotomy (46.4%).
PIP joint contractures had higher recurrence rates than MCP joint contractures across all treatments.
Limited fasciectomy also resulted in fewer reinterventions compared to collagenase and needle aponeurotomy.
Abstract
Compare contracture recurrence after limited fasciectomy (LF), collagenase Clostridium histolyticum (CCH), and needle aponeurotomy (NA) for Dupuytren contracture (DC) using prospectively collected studies with ≥2-year follow-up and assess recurrence by joint (metacarpophalangeal [MCP] vs proximal interphalangeal [PIP]). Systematic review restricted to prospective cohort series or randomized controlled trials treating DC with LF, CCH, and/or NA. Eligibility required ≥2-year, in-person clinical follow-up and explicit definition of contracture recurrence. Exclusions included non-English publications, telephone/questionnaire-only follow-up, no recurrence data at follow-up, and sample size <15 patients. The primary end point was recurrence by treatment. Secondary analyses evaluated recurrence by joint treated and reintervention and complications when reported. Ten studies met criteria,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
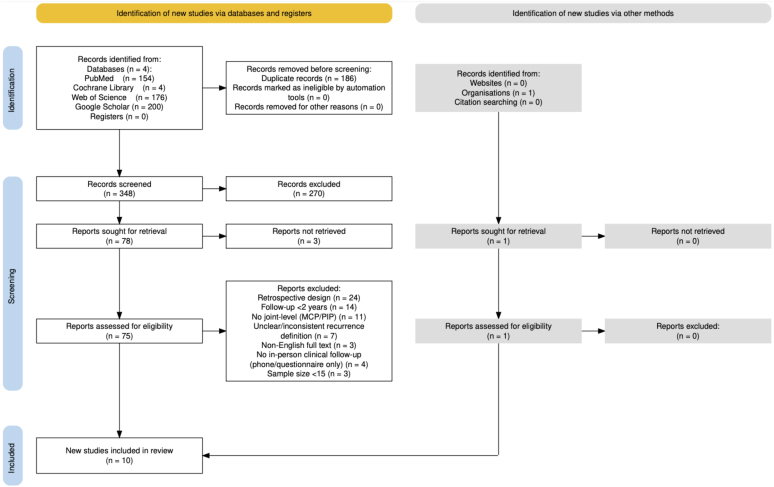 Figure 1
Figure 1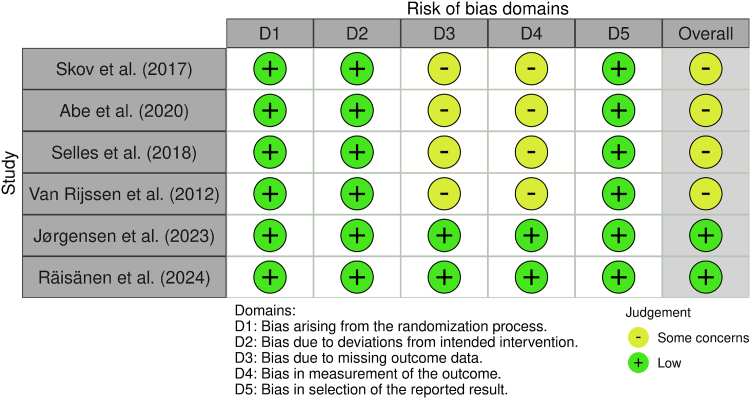 Figure 2
Figure 2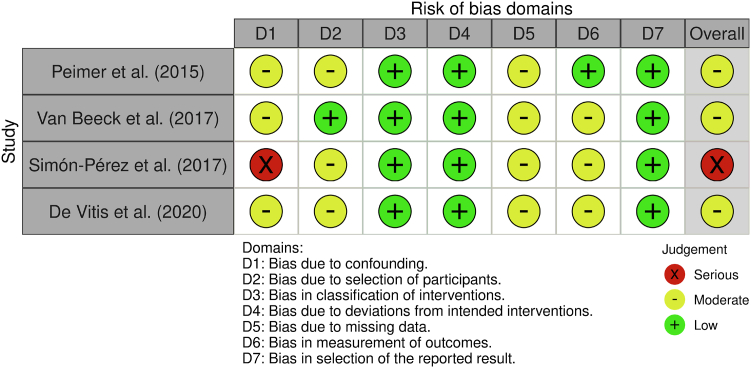 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDupuytren's Contracture and Treatments · Surgical Sutures and Adhesives · Genital Health and Disease
Dupuytren contracture (DC), also known as Dupuytren disease, is a chronic fibroproliferative disorder in which pathologic nodules and cords develop on the palmar fascia of the hand with variable progression to digital flexion contractures. The prevalence of DC varies across populations, seems to be more common in individuals of northern European descent, and has been estimated to occur in approximately 2.3% of the general population.1 When digital contractures develop, they most commonly involve the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints of the ring and little fingers.2 While nodules or mild contractures may have minimal effect on hand function, more severe contractures can impair activities of daily living and warrant treatment.3, 4, 5
Established treatments with demonstrated efficacy include fasciectomy, injection of collagenase Clostridium histolyticum (CCH), and needle aponeurotomy (NA). Fasciectomy surgically removes diseased fascia, with numerous variations including limited fasciectomy (LF), radical fasciectomy, and dermofasciectomy.6, 7, 8 CCH injection, Food and Drug Administration (FDA) approved in 2010,9 is a nonsurgical alternative that uses two enzymes that preferentially cleave type I and III collagen in Dupuytren cords, followed ≥24 hours later by manipulation into extension to rupture the enzymatically weakened cord.10, 11, 12 NA is a percutaneous fasciotomy technique using a hypodermic needle to puncture and partially section the cords under local analgesia, followed by immediate manipulation to rupture the mechanically weakened cords.13^,^14 Although all three methods are effective, none guarantees a permanent “cure”, and recontracture commonly occurs over time.15
It is challenging to counsel patients on the relative durability of these three procedures, as existing published studies are largely retrospective with small sample sizes and lower data quality. Authors have attempted to conduct systematic reviews of existing data to overcome issues related to small sample sizes; however, previous systematic reviews have had notable methodological limitations. For instance, studies included in prior systematic reviews have largely reported outcomes through 2–3-year follow-up,16^,^17 which may undercapture longer-term recurrence beyond 3 years. Many prior reviews have also included retrospective series subject to measurement and selection biases, further skewing recurrence data. Older systematic reviews did not include CCH as a treatment, as it has only been FDA approved for use since 2010.9 CCH was introduced in the European Union in 2011, but was revoked by the manufacturer in 2019,18 further limiting available data on CCH. Furthermore, existing reviews have included inconsistent or no clear definition of recurrence, further clouding results; authors have bemoaned the need for a consistent definition of DC recurrence,17^,^19, 20, 21, 22 and this lack of a clear definition may also in part explain why reported contracture recurrence rates vary so widely within the same treatment. One study showed that applying different definitions to a single data set changed the reported recurrence rates from 2% to 86%.21
We hypothesized that a rigorous systematic review of available publications limited to high-quality, prospectively collected data with a minimum 2-year follow-up would indicate that treatment with LF has the lowest likelihood of recurrence, followed by CCH and NA, and treatment of PIP joint contractures has a higher likelihood of recurrence versus MCP contractures across all treatments.
Materials and Methods
Study identification
This systematic review adhered to the Preferred Reporting Items in Systematic Review and Meta-Analysis (PRISMA) guidelines.23 A comprehensive literature search was conducted to identify studies reporting long-term outcomes of treatment for DC. The search included four databases: PubMed, Cochrane Library, Web of Science, and Google Scholar, covering articles published through December 2024. Search terms included combinations of keywords and MeSH terms: ‘Dupuytren∗’ (where ∗ denotes truncation to capture term variants), ‘Dupuytren’s contracture’, ‘Dupuytren’s disease’, ‘palmar fibromatosis’, ‘fasciectomy’, ‘fasciotomy’, ‘dermofasciectomy’, ‘aponeurotomy’, ‘aponeurectomy’, ‘needle aponeurotomy’, ‘percutaneous needle fasciotomy’, ‘percutaneous needle aponeurotomy’, ‘percutaneous fasciotomy’, ‘percutaneous aponeurotomy’, ‘collagenase’, ‘collagenase Clostridium histolyticum’, ‘xiaflex’, and ‘xiapex’. Reference lists of eligible articles were also reviewed to identify additional relevant studies.
Study inclusion
Studies were eligible for inclusion if they met the following criteria: (1) prospective case series or randomized controlled trial (RCT) in human subjects, (2) treatment of DC with LF, NA, and/or CCH injection, (3) minimum of 2-year clinical follow-up, (4) use of a clearly defined, consistent threshold for contracture recurrence, (5) available data on recurrence outcomes at final follow-up stratified by joint (MCP or PIP), and (6) a sample size of at least 15 patients. A minimum of 2-year follow-up was chosen as contracture recurrence is relatively rare within the first year of treatment.20 For any studies meeting the above criteria that did report on recurrence but not by joint, authors were contacted to determine if they had joint-level recurrence data that could be further analyzed; such studies were included if the data were available. Articles not published in English, lacking recurrence definitions, without in-person clinical follow-up (eg, telephone or questionnaire follow-up only), or without reported contracture recurrence data at final follow-up were excluded. The selection process is summarized in the PRISMA flow diagram (Fig. 1).Figure 1PRISMA flow diagram of study selection: diagram shows the identification, screening, and inclusion of studies, resulting in 10 eligible prospective studies. MCP, metacarpophalangeal; PIP, proximal interphalangeal.
Data extraction
Two independent reviewers screened all titles and abstracts for relevance. Full-text review was conducted for studies meeting initial screening criteria. Discrepancies were resolved through discussion or consultation with a third reviewer. Study characteristic data were extracted from each study (Table 1). Patient demographic and treatment variables were collected, with attention to treatment modality and involvement of the MCP and/or PIP joints (Tables 2 and 3). Other less common types of digital contractures, including distal interphalangeal (DIP) joint contractures, webspace contractures, and abduction/adduction contractures, in addition to secondary deformities, including Boutonnière deformities, were not specifically analyzed. Data were also extracted and stratified by treatment modality: LF, CCH injection, and NA. The primary outcome was contracture recurrence. Secondary outcomes, including reintervention and complication rates, were extracted when available.Table 1. Summary of Study Design and Key Characteristics of Included StudiesFirst Author (Year)Study DesignN (Patients)Intervention(s)Mean Follow-Up (Years)Definition of ContractureDefinition of RecurrenceRecurrence Stratified by Jointvan Rijssen (2012)30RCT93NA, LF5.0≥20° deficit at MCP or PIP≥20° at same jointYesPeimer (2015)31Prospective cohort623CCH5.0≥20° deficit at MCP or PIP≥20° at previously treated jointYesSkov (2017)29RCT43CCH, NA2.0≥20° deficit at PIP≥20° at same jointYesvan Beeck (2017)33Prospective cohort68CCH2.0≥20° deficit at MCP or PIP≥20° at same jointYesSelles (2018)27RCT52NA, LF5.0≥30° deficit at PIP and/or ≥20° at MCP≥20° at same jointYesSimón-Pérez (2018)32Prospective cohort71CCH2.3≥20° deficit at MCP or PIP≥20° at same jointYesAbe (2020)25Prospective cohort70CCH, NA3.0≥30° deficit at MCP or PIP≥20° at same jointYesDe Vitis (2020)26Prospective cohort39CCH7.0≥20° deficit at MCP, any deficit at PIP≥20° at same jointYesJørgensen (2023)28RCT68CCH, NA3.0≥30° deficit at MCP≥30° at same jointYesRäisänen (2024)34RCT302NA, CCH, LF2.0≥20° deficit at MCP or PIP in index through small fingers≥20° at same jointYesTable 2Patient DemographicsPatient DemographicsValue∗Total no. of patients (all studies)1,411No. of men (%)1,202 (85.2%)Average age (years)66∗Values are derived based on the number of patients who completed the primary end point of at least 2 years of follow-up.Table 3. Total Number of Joints Treated by Procedure and Joint TypeMCPPIPTotal# Joints treated by NA235132367# Joints treated by CCH7473091,056# Joints treated by LF18194275# Joints treated (all procedures)1,1635351,698
When data were incomplete or ambiguous, efforts were made to contact corresponding authors for clarification. Disagreements in extracted data were resolved by consensus. Extracted data were then compiled into summary tables for descriptive and statistical analysis.
Risk of bias
Two reviewers independently assessed the methodological quality of each study. RCTs were appraised with version two of the Cochrane risk-of-bias tool for randomized trials (RoB 2.0), covering five domains: randomization, deviations from intended interventions, missing data, outcome measurement, and selective reporting. Nonrandomized prospective studies were evaluated using the Risk of Bias in Non-Randomized Studies of Interventions tool (ROBINS-I), which assesses bias due to confounding, participant selection, intervention classification, deviations, missing data, outcome measurement, and reporting. Each domain was rated as low risk, some concerns, or high risk, following Cochrane Handbook guidelines. Discrepancies were resolved by consensus with a senior author. Assessments are summarized with robvis plots (Figs. 2 and 3).24Figure 2. RoB 2 assessment of randomized controlled trials by bias domain (D1–D5) and overall risk. Green circles indicate low risk of bias, and yellow circles indicate some concerns.Figure 3ROBINS-I assessment of nonrandomized prospective cohort studies by bias domain (D1–D7) and overall risk. Green circles indicate low risk of bias, yellow circles moderate risk, and red circles serious risk.
Statistics
Statistical analysis
The primary outcome was contracture recurrence, which was further analyzed based on treatment type and the affected joint(s) (MCP and/or PIP joint) rather than as a function of digit treated. If a patient had a contracture in a joint that was treated using any modality, that joint was included in the study. Joints that were not treated were excluded from analysis. If both the MCP and PIP joints in the same digit were affected and both were treated, then both joints were included in the study as separate data points. Recurrence was also defined on a per-joint basis. If a patient had a recurrence in only one joint, then only that specific joint was defined as having recurrence. Secondary outcomes included reintervention rate and treatment-related complications. Recurrence, joint treated, and reintervention were treated as binary outcomes for statistical analysis. Pairwise meta-analyses were conducted to compare outcomes between-treatment groups using the SAS BGLIMM procedure with a logit link function. An alpha level of 0.05 was used to determine statistical significance.
Results
Descriptive data
Ten prospective studies met criteria, comprising 1,411 adult patients and 1,698 joints (Table 1).25, 26, 27, 28, 29, 30, 31, 32, 33, 34 None of the 1,698 joints included had prior treatment of their contracture. LF was the only method of fasciectomy reported. One study reporting on NA added simultaneous lipofilling.27 No studies reported concomitant corticosteroid injection at the time of intervention. For one study in which joint-level recurrence data were unavailable in the publication, authors were contacted and provided data on recurrence as a function of joint for inclusion.34
All RCTs demonstrated low risk in randomization and intervention fidelity (D1–D2) but showed some concerns regarding missing data and outcome measurement (D3–D4). As a result, overall risk was rated as “some concerns” for four of six RCTs. Two RCTs achieved a “low risk” rating (Fig. 2).28^,^34 Among nonrandomized studies, moderate risk was common, particularly in confounding, selection, missing data, and outcome measurement (D1, D2, D5, D6). One study was judged to have serious overall risk due to confounding bias (Fig. 3).32
Demographic variables were variably reported (Table 2). Most patients underwent CCH (62.2%), followed by NA (21.6%), and LF (16.2%, Table 3). Patient/joint, follow-up time, and recurrence information were stratified by treatment (Table 4). Overall weighted mean follow-up was 3.8 years (range 2–7 years). ANOVA analysis revealed that weighted mean follow-up time (by number of patients) did not differ between groups (CCH = 4.2 years, NA = 3.4 years, and LF = 3.2 years). Joints treated with LF had the lowest recurrence rate (16.5%), followed by CCH (32.5%) and NA (46.4%).Table 4. Number of Patients/Joint, Follow-Up time, and Recurrence as a Function of Treatment TypeTreatmentNo. of StudiesNo. of Patients, n (%)No. of Joints, n (%)Follow-Up Years, Median (Min, Max)Recurrence Rate (Min, Max)NA6 (Study: A, B, C, D, E, and J)267 (18.9)367 (21.6)3 (2, 5)46.4 (18, 79)CCH8 (Study: B, C, D, F, G, H, I, and J)985 (69.8)1,056 (62.2)3 (2,7)32.4 (5, 92)LF3 (Study: A, E, and J)159 (11.3)275 (16.2)5 (5, 5)16.5 (5, 39)Total9 (Study: A–I)1,4111,6984 (2, 7)
The likelihood of recurrence varied among treatment groups (Table 5). Mixed model analyses showed that joints treated with CCH had a significantly lower likelihood of recurrence compared to NA (OR = 0.64, CI 0.42, 0.98) but had a higher likelihood of recurrence compared to joints treated with LF (OR = 2.7, CI 1.20, 5.99). Joints treated with NA also had a significantly higher likelihood of recurrence compared to LF (OR = 4.55, CI 2.65, 7.81). Across all three treatments, MCP contractures were two-thirds less likely to recur than PIP contractures (OR = 0.34, CI: 0.27, 0.44).Table 5. Likelihood of Contracture Recurrence as a Function of Treatment and Joint TreatedComparisonOdds RatioConfidence IntervalCCH vs NA0.640.42–0.98CCH vs LF2.711.20–5.99NA vs LF4.552.64–7.81MCP vs PIP0.340.27–0.44
Seven studies reported on reinterventions. For LF, 5 of 13 (38.5%) recurrences had a reintervention (2 studies); for NA, 13 of 42 (31%) recurrences had a reintervention (2 studies); for CCH, 146 of 367 (39.8%) recurrences had a reintervention (5 studies). Joints treated with LF had the lowest reintervention rate (1.8%), followed by NA (3.5%) and CCH (13.8%, Table 6). Mixed model analyses showed that joints treated with CCH were nine times more likely to have reintervention than LF (OR 9.15, CI 2.07, 44.88), and joints treated with NA were more than seven times more likely to have reintervention than LF (OR = 7.68, CI 1.6, 41.00, Table 7). The likelihood of reintervention was not significantly different in joints treated with CCH versus NA.Table 6. Reintervention Rates and Number of Joints Requiring Reintervention by ProcedureProcedureTotal Joints TreatedNo. of Joints Requiring Reintervention (%)NA36713 (3.5%)CCH1056146 (13.8%)LF2755 (1.8%)Table 7. Likelihood of Reintervention as a Function of TreatmentComparisonORCICCH vs NA1.430.65–3.08CCH vs LF9.152.07–44.88NA vs LF7.681.60–41.00
The most common complications were digital nerve injury, tendon injury, skin tear, swelling, pain, and bleeding. Data on complications are summarized (Table 8). Statistical comparisons of complications across treatments and joints were not performed as the data on complications were of high heterogeneity in reporting across studies, precluding meaningful comparisons.Table 8. The Ten Most Reported Complications Across All StudiesComplicationNo. of Studies ReportingDigital nerve injury6Skin tear4Pain and swelling4Bleeding4Flexor tendon injury3Allergic reaction2Infection/wound healing2Complex regional pain syndrome2Hyperesthesia1Stiffness1No complications reported2Because complications were inconsistently reported and often not stratified by treatment modality, this table reflects the number of studies reporting each complication rather than incidence or modality-specific frequency.
Discussion
DC is often described as a condition without a “cure”, as contracture recurrence remains common after treatments. The challenge of recurrence has stimulated investigation of alternative therapies to minimize disease progression and/or reduce the likelihood of recurrence.35^,^36 The decision on treatment modality is often made without a clear understanding of what recurrence risk is for a given treatment. Attempts have been made to systematically review the likelihood of recurrence after treatments, but four systematic reviews conducted before 2019 had methodological flaws of retrospective data, short follow-up, small sample sizes, and no objective definition of recurrence, as well as limited inclusion of CCH.17^,^20^,^37^,^38
More recent (2023–2025) systematic reviews have attempted to address these flaws, but all had notable limitations. A 2023 meta-analysis of RCTs with ≥3-year follow-up (n = 347; CCH vs NA) found no differences in recurrence or final flexion contracture, but LF was not evaluated.39 A subsequent 2024 systematic review (11 studies; n = 1,051) reported higher recurrence rate with CCH (25.8%) versus LF (9.3%) and more severe complications with LF (7.3%) versus CCH (0.3%), but included short follow-up (≥3 months) and nonstandard recurrence definitions (two studies used patient perception of need for reintervention).40 A 2025 systematic review of RCTs (11 trials; n = 969) comparing CCH, NA, and LF found no difference in recurrence between CCH and NA, but higher recurrence in CCH versus LF. Interpretation was limited by short-term follow-up (minimum 12 months) and heterogeneous recurrence definitions (eg, counting reintervention as recurrence).41 Another 2025 meta-analysis (15 studies) used time-to-event methods and reported the highest recurrence after CCH (41%), followed by NA (33%) and LF (10%) at 3-year median follow-up. Time-to-recurrence did not differ between CCH and NA, whereas younger age and female sex predicted earlier recurrence. Recurrence analyses, however, included only 245 patients (CCH 66, LF 51, NA 128), and 9 of 15 studies were retrospective, limiting power and internal validity.42 The most recent 2025 meta-analysis of 17 RCTs (n = 1,010) showed LF had the lowest long-term recurrence compared to NA and CCH but had more severe complications; this study was limited by shorter follow-up (max = 3 years) and no explicit recurrence definition.16
The present review addressed these limitations by enforcing a strict recurrence definition, including only prospective studies and requiring ≥2-year follow-up. Among 1,411 patients (1,698 joints), recurrence risk ranked LF < CCH < NA: CCH had approximately one-third lower odds of recurrence than NA; CCH had approximately threefold higher odds of recurrence than LF; NA had roughly fivefold higher odds of recurrence than LF. A mechanistic rationale for this observation is that LF removes the largest burden of diseased tissue, CCH enzymatically degrades cords, removing some burden of disease, and NA divides tissue without removal. Prior reviews consistently found higher recurrence after CCH or NA than LF; to our knowledge, this is the first demonstration of higher recurrence after NA versus CCH.
Furthermore, the current review revealed that, regardless of treatment, the risk of recurrence was two-thirds less likely for MCP contractures compared to PIP contractures at a mean follow-up of 3.8 years, consistent with previous studies. For instance, one prospective cohort study found recurrence rates of 14% for MCP joints and 23% for PIP joints following CCH.43 Similarly, a 10-year follow-up study reported recurrence rates of 54.8% for MCP joints and 100% for PIP joints after CCH.44 These findings suggest that PIP joints are more susceptible to recurrence, regardless of the treatment. This may be partially explained by combined volar plate/collateral ligament contracture with extensor mechanism attenuation in chronic PIP disease. Patient characteristics may influence recurrence, including family history, alcohol use, age at onset, body mass index, and sex.45 Our analysis did not adjust for these variables, and some included nonrandomized studies may reflect confounding by indication.
A secondary end point of this study was the likelihood of reintervention after initial treatment. Seven of the 10 included studies reported on reinterventions. Patients treated with CCH were nine times more likely to have reintervention than those treated with LF, and patients treated with NA were over seven times more likely to have reintervention than those treated with LF. Several factors may influence the likelihood of reintervention independently of contracture recurrence, including perceptions that surgery offers more permanent results and the desire to avoid pain, recovery time, or inconvenience associated with specific interventions. Moreover, the potential for severe surgical complications may contribute to a diminished willingness to undergo repeat surgery. Interestingly, although CCH had a lower recurrence risk than NA, it did have a higher reintervention risk for reasons that are unclear. One potential explanation is that not all reinterventions were necessarily for recurrence. For instance, a joint treated with CCH that resulted in tendon rupture may have been captured as a reintervention; in this case, the reintervention would have been to treat a complication rather than a recurrence.
The most common complications identified in this review were digital nerve injury, tendon injury, skin tears, swelling, pain, and bleeding. The data on complications in the present review were heterogenous and reported inconsistently, precluding meaningful statistical analysis between groups. While the incidence of severe complications was generally low with first-time surgical treatment,25^,^29^,^30 the incidence of severe complications has been reported to be much higher with repeat fasciectomy or dermofasciectomy.46 Ideally, treatments for DC should be chosen not only based on their ability to delay/prevent recurrence but also based on risk of complications and expected recovery time.
This review has limitations. Although we required a ≥2-year follow-up, several studies still had relatively short observation. Long-term surveillance is costly, and emerging biomarkers may offer shorter-horizon surrogates of disease activity before recurrent contractures are evident.47 The LF cohort was relatively small (275/1,698 joints), reducing power for between-treatment comparisons. We sought to apply a uniform, objective recurrence definition, but one study28 had a slightly different definition than the other nine, introducing heterogeneity. A consensus definition remains unsettled: one group defined recurrence as passive extension deficit >20° in ≥1 joint with a palpable cord compared with 6–12 weeks presurgery,21 whereas a Delphi panel endorsed >20° contracture recurrence in any treated joint at 1-year post-treatment relative to 6 weeks post-treatment.19
Future studies should aim to address these limitations by employing longer follow-up periods to capture long-term recurrence data, ensuring more balanced representation between-treatment groups and standardizing treatment protocols and definitions of recurrence to best understand the risks of contracture recurrence after treatments. Nevertheless, the current data may help inform clinicians and patients on the relative likelihood of recurrence after each of these three common treatments.
Conflicts of Interest
Dr. Mark A. Vitale served on the advisory board for Endo Pharmaceuticals, Inc in 2022. The other authors have no relevant conflicts to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Salari N.Heydari M.Hassanabadi M.The worldwide prevalence of the Dupuytren disease: a comprehensive systematic review and meta-analysis J Orthop Surg Res 15120204953311548310.1186/s 13018-020-01999-7PMC 7594412 · doi ↗ · pubmed ↗
- 2Townley W.A.Baker R.Sheppard N.Grobbelaar A.O.Dupuytren's contracture unfolded Bmj 332753820063974001648426510.1136/bmj.332.7538.397PMC 1370973 · doi ↗ · pubmed ↗
- 3Dibenedetti D.B.Nguyen D.Zografos L.Ziemiecki R.Zhou X.Prevalence, incidence, and treatments of Dupuytren's disease in the United States: results from a population-based study Hand (N Y)6220111491582177619810.1007/s 11552-010-9306-4PMC 3092891 · doi ↗ · pubmed ↗
- 4Turesson C.Kvist J.Krevers B.Experiences of men living with Dupuytren's disease-consequences of the disease for hand function and daily activities J Hand Ther 33320203863933147732910.1016/j.jht.2019.04.004 · doi ↗ · pubmed ↗
- 5Wilburn J.Mc Kenna S.P.Perry-Hinsley D.Bayat A.The impact of Dupuytren disease on patient activity and quality of life J Hand Surg Am 3862013120912142370701810.1016/j.jhsa.2013.03.036 · doi ↗ · pubmed ↗
- 6Rodrigues J.N.Becker G.W.Ball C.Surgery for Dupuytren's contracture of the fingers Cochrane Database Syst Rev 2015122015 CD 01014310.1002/14651858.CD 010143.pub 2PMC 646495726648251 · doi ↗ · pubmed ↗
- 7Pandya W.C.A.Bhatti D.Manley O.A longitudinal analysis of 281 cases of dermofasciectomy efficacy in advanced Dupuytren disease cases: a 20-year perspective J Hand Surg Am 50620256566624023768210.1016/j.jhsa.2025.02.007 · doi ↗ · pubmed ↗
- 8Dias J.Tharmanathan P.Arundel C.Collagenase injection versus limited fasciectomy for Dupuytren's contracture N Engl J Med 391162024149915103938345410.1056/NEJ Moa 2312631 PMC 7616701 · doi ↗ · pubmed ↗