Biomarker guided combination strategies and perioperative integration for immune cold microsatellite stable colorectal cancer
Nan Yao, Wenqiang Li, Ning Duan, Fuzhou Han, Guoyong Yu, Jun Qu

TL;DR
This paper explores strategies to convert immune-cold microsatellite stable colorectal cancer into immune-responsive states using combination therapies and biomarker guidance.
Contribution
The paper introduces novel frameworks for biomarker-guided treatment selection and perioperative integration in MSS CRC.
Findings
Combination therapies like anti-angiogenic/VEGFR + ICI show progression-free survival benefits in some MSS CRC cases.
Dual-checkpoint inhibitors demonstrate durable responses in pretreated MSS mCRC patients.
Biomarker-anchored selection and perioperative integration may improve outcomes in biologically selected MSS CRC contexts.
Abstract
Most colorectal cancers (CRC) are microsatellite stable (MSS) and show little benefit from single-agent immune checkpoint inhibition (ICI). A rapidly expanding body of work now focuses on combination strategies to remodel the tumor microenvironment (TME) and convert immune-“cold” MSS disease into an immune-responsive state. We synthesize (i) biological liabilities that underpin MSS immune resistance; (ii) clinical evidence across key combination classes—anti-angiogenic/VEGFR + ICI (randomized AtezoTRIBE suggests a progression-free survival benefit when atezolizumab is added to FOLFOXIRI + bevacizumab), multikinase TKI + PD-1/PD-L1 (mixed activity and geographic/site heterogeneity; LEAP-017 was negative for overall survival), dual-checkpoint or next-generation CTLA-4 backbones (phase-1 botensilimab + balstilimab with durable responses in heavily pretreated MSS mCRC), EGFR- or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
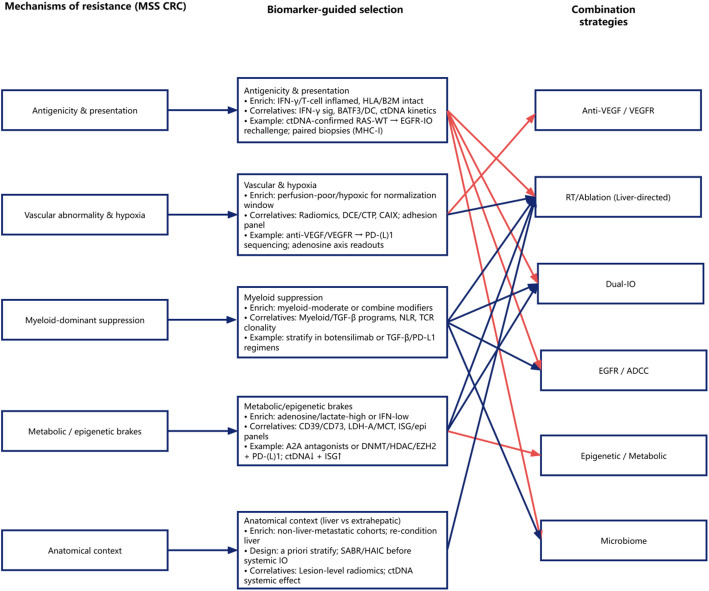 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Colorectal Cancer Treatments and Studies · Cancer Cells and Metastasis
Introduction
Immune checkpoint blockade (ICB) is transformative in MSI-H/dMMR CRC, yet > 85% of CRC are MSS/pMMR and have minimal responses to PD-(L)1 or CTLA-4 monotherapy [1, 2]. In MSS disease, multiple layers of immune exclusion converge: low neoantigenicity and defective cross-presentation limit priming; WNT/β-catenin signaling, TGF-β–rich stromal programs (often CAF/CMS4-skewed), and aberrant vasculature collectively suppress dendritic cell recruitment and T-cell trafficking [3–6]. VEGF-driven endothelial anergy (reduced ICAM-1/VCAM-1), hypoxia/HIF-1α, and perivascular fibrosis further gatekeep lymphocyte entry [5]. The myeloid compartment is dominant and suppressive—M2-like TAMs, MDSCs, and TANs elaborate IL-10, TGF-β, arginase and ROS, while chemokine axes (e.g., CXCL8–CXCR1/2) perpetuate exclusion [7, 8]. Metabolic and epigenetic brakes—adenosine–A2A, IDO1/tryptophan catabolism, lactate/acidic pH, and repressive chromatin states—dampen type-I/II interferon programs and cytotoxic effector function [9–11].
Clinically, hepatic metastases impose a uniquely tolerogenic niche: antigen is filtered through Kupffer cells and sinusoidal endothelial cells, with antigen-presenting cell skew and PD-L1/galectin-9 up-regulation that delete or exhaust circulating tumor-specific T cells and blunt systemic ICI effects; by contrast, extrahepatic-dominant disease shows relatively higher immune responsiveness [12, 13].
While liver metastases can create a tolerogenic niche through macrophage polarization, antigen sequestration/deletion, and systemic T-cell dysfunction, the presence of hepatic disease in clinical cohorts should also be interpreted with epidemiologic nuance, as it is an aggregate marker that often correlates with higher tumor burden, more aggressive disease kinetics, and tumor-intrinsic programs (e.g., CMS2/CMS4 under CMS subtyping) that themselves shape outcomes. Therefore, an observed “liver effect” in immunotherapy-treated MSS CRC may reflect a true immunologic barrier, a prognostic confounder, or both. To reduce conflation of metastatic site with tumor biology, we reorganized the evidence synthesis into (i) mechanistic/translational data supporting liver-driven systemic immune suppression, (ii) clinical association studies, and (iii) studies incorporating adjustment or stratification by tumor burden surrogates and tumor-intrinsic features where available. Importantly, primary tumor sidedness (right vs. left) correlates with molecular background and metastatic patterns and should be considered when interpreting hepatic metastasis as a modifier of immunotherapy benefit. Future trials and real-world analyses should prespecify interaction testing (liver vs. non-liver; sidedness; molecular subtype) and incorporate tumor burden metrics (e.g., number/volume of metastatic lesions, LDH) to better disentangle barrier versus confounding effects.
These insights motivate combination regimens that (i) normalize vasculature (anti-VEGF/VEGFR) to open trafficking windows [14]; (ii) reprogram myeloid networks (e.g., CSF1R, CXCR1/2, TGF-β traps) to restore antigen presentation [6, 7, 15, 16]; (iii) increase antigen release/visibility (RT/SABR, oncolytic or EGFR/HER2-directed ADCC, bispecifics such as CEA-TCB) [17–19]; and (iv) relieve metabolic/epigenetic brakes (A2A antagonists, IDO-pathway, DNMT/HDAC modulators)—ideally converting MSS tumors into sustained, IFN-rich inflamed TMEs [9–11]. Embedding biomarker-anchored selection (active liver involvement, T-cell-inflamed signatures, and on-treatment ctDNA kinetics) and sequence timing (e.g., short VEGF-normalization windows before ICI) will be critical to translate this biology into durable clinical benefit [12, 14].
Scope and search
We conducted a prespecified narrative review of biomarker-guided combination strategies to overcome resistance in MSS/pMMR colorectal cancer. We searched PubMed/MEDLINE, Embase, Web of Science, Cochrane CENTRAL, ClinicalTrials.gov, and ASCO/ESMO/AACR abstracts from 1 Jan 2015 to 31 Oct 2025. Queries combined CRC + MSS/pMMR + immunotherapy (PD-1/PD-L1/CTLA-4) with major partners (anti-VEGF/VEGFR, EGFR/ADCC, liver-directed RT/ablation, epigenetic/metabolic, microbiome); key trial/drug names (e.g., AtezoTRIBE, LEAP-017, CAVE, botensilimab+balstilimab, REGONIVO/REN-series) were added to capture signal-defining studies. Inclusion: prospective trials, peri-operative/window studies, or comparative cohorts that enrolled MSS populations (or extractable MSS subgroups) and reported ORR/PFS/OS and/or human correlatives (e.g., ctDNA dynamics). Exclusion: MSI-H/dMMR-only cohorts, case reports/very small series, and purely preclinical work. Two reviewers screened records with consensus resolution. Evidence is summarized by design tier—A: randomized; B: prospective non-randomized; C: retrospective comparative with adjustment; D: exploratory signals/correlatives—with mixed-population trials labeled and reported by their MSS-specific results.
Mechanisms of resistance in MSS CRC
Antigenicity and presentation
Most MSS tumors carry low neoantigen loads and often harbor defects in the antigen-presentation axis (e.g., down-modulated HLA class I, B2M loss, impaired IFN-γ/JAK–STAT signaling) [20–24]. Oncogenic programs like WNT/β-catenin suppress dendritic-cell recruitment (via reduced CCL4/CCL5 and CXCL9/10) and blunt priming in tumor-draining nodes, yielding a T-cell–excluded phenotype even when PD-1/PD-L1 is blocked [25, 26].
Vascular abnormality and hypoxia
VEGF-driven “endothelial anergy” lowers ICAM-1/VCAM-1 and tightens the endothelial barrier, throttling lymphocyte trafficking [5, 27]. Hypoxia and HIF-1α foster acidosis and perivascular fibrosis, further limiting infiltration. Short-lived “vessel normalization” with anti-VEGF/VEGFR therapy can transiently reopen the gate for immune recruitment—most useful when synchronized with T-cell–activating strategies (ICB, vaccines, RT/ablation) [27–29].
Myeloid-dominant suppression
M2-skewed TAMs, granulocytic/monocytic MDSCs, and TANs accumulate under CXCL8–CXCR1/2, CSF1/CSF1R, and GM-CSF axes. They secrete IL-10, TGF-β, ARG1 and ROS, quenching CD8⁺ cytotoxicity and dendritic cross-presentation while siphoning nutrients (arginine, cysteine). Targetable hubs include CXCR1/2, CSF1R, and TAM-reprogramming approaches (CD40 agonism, PI3K-γ inhibition) [8, 15, 30–32].
Metabolic/epigenetic brakes
Tumor and stromal cells generate lactate (LDHA) and adenosine (CD39/CD73), activating A2A signaling and acidifying the TME—both dampen TCR signaling and IFN programs [33–36]. Tryptophan catabolism (IDO1/TDO2→kynurenine→AhR) reinforces exhaustion [37, 38], and repressive chromatin states (DNMT/HDAC/PRC2 activity) silence antigen-presentation and Th1 chemokines. Combinatorial tactics include A2A antagonists, CD73 blockade, metabolic buffering, and epigenetic “priming” (DNMT/HDAC inhibitors) to restore antigenicity and inflamed gene signatures [39–43].
Anatomical context
Active liver metastases create systemic tolerance: hepatic myeloid cells and LSECs cross-present antigen in a tolerogenic fashion, delete/disable circulating CTLs, and skew cytokine milieus toward IL-10/TGF-β [44–46]. However, in clinical cohorts, liver involvement may also proxy higher tumor burden and tumor-intrinsic programs; therefore, observed associations likely reflect both immunologic barrier effects and prognostic confounding, motivating prespecified interaction analyses (liver vs. non-liver; sidedness; molecular subtype) and inclusion of burden metrics (e.g., LDH, lesion number/volume). Clinically, multiple VEGFR-IO and dual-IO regimens show attenuated benefit when liver disease is untreated, whereas responses concentrate in non-liver-metastatic or liver-controlled cohorts—supporting aggressive liver-directed therapy (resection, ablation, radiation, or effective hepatic arterial strategies) to “unlock” systemic ICI [47–50].
A mechanism-to-biomarker-to-therapy framework is summarized in Fig. 1.
Fig. 1. Mechanism-based, biomarker-guided combination strategies for immune-cold MSS colorectal cancer. Conceptual framework linking key resistance mechanisms in MSS colorectal cancer (left) to biomarker-guided selection/monitoring domains (middle) and corresponding combination strategy modules (right).* MSS* microsatellite stable,* CRC* colorectal cancer,* ctDNA* circulating tumor DNA,* EGFR* epidermal growth factor receptor,* VEGF* vascular endothelial growth factor,* VEGFR* vascular endothelial growth factor receptor,* RT* radiotherapy,* ADCC* antibody-dependent cellular cytotoxicity,* ICI* immune checkpoint inhibitor,* IO* immuno-oncology,* IFN-γ* interferon gamma,* HLA* human leukocyte antigen,* B2M* beta-2 microglobulin,* MHC-I* major histocompatibility complex class I,* DCE* dynamic contrast-enhanced,* CTP* computed tomography perfusion,* CAIX* carbonic anhydrase IX,* TGF-β* transforming growth factor beta,* NLR* neutrophil-to-lymphocyte ratio,* TCR* T-cell receptor,* LDH-A* lactate dehydrogenase A,* MCT* monocarboxylate transporter,* ISG* interferon-stimulated genes
Evidence across combination classes
Key representative trials across combination classes and their biomarker roles are summarized in Table 1.
Table 1. Representative clinical studies of combination strategies for MSS/pMMR metastatic colorectal cancerStrategyStudyauthorReferencesBiomarker roleResultsAnti-angiogenic + ICIFOLFOXIRI + Bev±Atezo vs. FOLFOXIRI + BevCarlotta AntoniottiAntoniotti et al. AtezoTRIBE. Lancet Oncol. 2022;23:876–887PrognosticPFS improved: 13.1 vs. 11.5 months; HR = 0.69 p = 0.012Radiotherapy/ablation + ICITNT(FOLFOX→CRT)±Pembro vs. TNT(FOLFOX→CRT)Osama E. RahmaRahma et al. NRG-GI002 (pembro arm). JAMA Oncol. 2021;7:1225–1230.MonitoringNAR 11.53 vs. 14.08, p = 0.26;pCR 31.9% vs. 29.4%, p = 0.75;G3–4 AEs 48.2% vs. 37.3%Dual-checkpoint or next-generation IO backbonesBotensilimab+BalstilimabAndrea J BullockBullock et al. BOT + BAL in MSS mCRC (Ph1). Nat Med. 2024;30:2558–2567.PrognosticORR 17%;mPFS 3.5 months༛mOS 20.9 monthsEGFR/HER2-targeted + ICICetuximab + AvelumabErika MartinelliMartinelli et al. CAVE trial. JAMA Oncol. 2021;7:1529–1535.PredictivemOS 11.6 months; mPFS 3.6 months༛ORR 7.8% ༛DCR 65%Epigenetic/metabolic re-programming + ICIEntinostat+ PembrolizumabNilofer Saba AzadAzad et al. ENCORE-601 (enti+pembro) in MSS mCRC. JCO 2018;36(15_suppl):3557.MonitoringRR 6%(1/16), mPFS 86days, SD 9/16Microbiome and barrier modulation + ICITislelizumab + Fruquintinib + FMTWensi ZhaoZhao et al. RENMIN-215 update. AJCR 2024;14:5351–5364.MonitoringORR 20%(4/20);DCR 95%༛mOS 13.7 months
Selected trials and cohorts are summarized by strategy class, regimen, and key efficacy outcomes. ICI, immune checkpoint inhibitor; IO, immuno-oncology; FOLFOXIRI, fluorouracil (5-FU), leucovorin, oxaliplatin, and irinotecan; FOLFOX, fluorouracil (5-FU), leucovorin, and oxaliplatin; TNT, total neoadjuvant therapy; CRT, chemoradiotherapy; Bev, bevacizumab; Atezo, atezolizumab; Pembro, pembrolizumab; EGFR, epidermal growth factor receptor; HER2, human epidermal growth factor receptor 2; FMT, fecal microbiota transplantation; PFS, progression-free survival; OS, overall survival; mPFS, median progression-free survival; mOS, median overall survival; ORR, objective response rate; DCR, disease control rate; RR, response rate; SD, stable disease; HR, hazard ratio; NAR, neoadjuvant rectal score; pCR, pathological complete response; AEs, adverse events; G, grade.
Anti-angiogenic (anti-VEGF/VEGFR) + ICI
Rationale. Vascular normalization increases antigen trafficking and T-cell infiltration; VEGF blockade also reduces Treg/MDSC recruitment [14, 27, 51]. AtezoTRIBE (first-line, randomized Phase II). Adding atezolizumab to FOLFOXIRI + bevacizumab in previously untreated mCRC improved PFS: 13.1 vs. 11.5 months; HR 0.69 (80% CI 0.56–0.85). Safety was manageable with more neutropenia/diarrhea but no new signals. This provides proof-of-concept for chemo + anti-VEGF + PD-L1 intensification up-front, in an unselected population with majority MSS [52]. TKI + PD-1 in refractory MSS. The US regorafenib + nivolumab phase-2 trial treated 70 of 94 enrolled; ORR 7%, PFS 1.8 months [47]; all responses occurred in patients without liver metastases.
Geographic and site-of-disease heterogeneity has been repeatedly observed, with poorer outcomes in liver-dominant disease and modest benefit overall.
LEAP-017 (lenvatinib + pembrolizumab, randomized Phase III). In 480 previously treated pMMR/MSS mCRC patients, OS 9.8 vs. 9.3 months; HR 0.83 (95% CI 0.68–1.02) did not meet the prespecified significance threshold, confirming no statistically significant OS improvement versus regorafenib or trifluridine/tipiracil. Safety was as expected for the class [53].
Radiotherapy/ablation (RT/SABR) + ICI
Rationale. RT enhances antigen release, MHC-I expression and type-I IFN signaling, potentially driving abscopal effects with PD-(L)1. Thermal ablation/SABR may achieve similar immunogenic cell death [54].
Clinical picture. In locally advanced rectal cancer (LARC) enriched for pMMR/MSS, adding pembrolizumab to TNT/CRT did not improve the neoadjuvant rectal (NAR) score in a randomized phase-2 trial, despite acceptable safety—underscoring that pMMR tumors require deeper biological selection or different sequencing [55].
In oligometastatic disease, early studies show feasibility and occasional systemic responses; however, dose/fractionation and IO timing (pre- vs. post-RT) remain unresolved in MSS-focused randomized data [56, 57].
Dual-checkpoint or next-generation IO backbones
Rationale. CTLA-4 (priming) + PD-1 (effector rescue) increases T-cell breadth; Fc-engineered CTLA-4 (e.g., botensilimab) may enhance intratumoral Treg depletion and myeloid re-programming.
Phase-1 botensilimab + balstilimab. In 148 heavily pretreated MSS mCRC patients (MSS expansion; 101 response-evaluable), ORR 17% (95% CI 10–26), DCR 61%, median PFS 3.5 months, and durable responses were reported with manageable immune toxicity, with activity enriched in patients without active liver metastases [58, 59].
EGFR/HER2-targeted + ICI
Rationale. Cetuximab (IgG1) can trigger ADCC, facilitate antigen cross-presentation and prime for PD-L1 blockade; HER2-targeted agents may also engage immunity.
CAVE/CAVE-2 (EGFR rechallenge). In RAS wild-type mCRC previously benefiting from anti-EGFR, cetuximab + avelumab showed disease control and signs of activity as a rechallenge strategy (n ≈ 77 in CAVE). ctDNA-confirmed RAS/BRAF WT status appears to enrich benefit.
Randomized MSS-specific confirmation is needed [60, 61].
Epigenetic/metabolic re-programming + ICI
DNMT/HDAC inhibitors, adenosine A2A antagonists, tryptophan/IDO pathway inhibitors, and lactate transport blockade are being tested to lift transcriptional/metabolic brakes and restore interferon signaling. While the mechanistic rationale is strong, definitive randomized signals in MSS CRC remain pending; rational triplets (e.g., VEGF + epigenetic modulator + PD-1) in adaptive platforms may be required to identify synergistic windows [42, 62–65].
Microbiome and barrier modulation + ICI
Gut microbiota shape APC programming and T-cell tone. Early MSS CRC experiences using FMT or targeted pro-/post-biotics are small but feasible with rigorous donor safety. Prospective trials integrating shotgun metagenomics/metabolomics with IO readouts (and ctDNA) are a high-yield path forward [66–68].
Biomarker-guided selection
Prognostic, predictive, and response-monitoring biomarkers In MSS CRC, many candidate biomarkers are discussed under the umbrella of “biomarker-guided selection,” yet their evidentiary roles differ. We therefore distinguish: (i) prognostic biomarkers that correlate with outcomes irrespective of treatment, (ii) predictive biomarkers that modify the likelihood of benefit from a specific therapeutic class, and (iii) pharmacodynamic/response-monitoring biomarkers that capture early on-treatment biological response. For example, ctDNA kinetics and clearance are robust markers of tumor burden dynamics and treatment response, and can serve as early readouts to support continuation, escalation, or mechanism switching; however, ctDNA clearance alone does not inherently specify whether a VEGF-, EGFR-, or RT-anchored combination is the optimal initial strategy. Where predictive evidence is limited in MSS CRC immunotherapy combinations, we explicitly label biomarkers as hypothesis-generating and prioritize trial designs incorporating prospective stratification and interaction testing.
Disease topology (liver vs. extrahepatic). Across regorafenib + nivolumab and RIN (regorafenib + ipilimumab + nivolumab), responses were essentially absent with active liver metastases and concentrated in non-liver-metastatic disease [47, 69]. This consistent pattern argues for a-priori stratification by liver involvement in trial design and for liver-directed “re-conditioning” strategies when feasible [49, 70].
Transcriptional inflammation. T-cell-inflamed IFN-γ signatures and myeloid/TGF-β programs may define “heatable” niches vs. profoundly excluded tumors; embedding tissue and liquid-biopsy correlatives is essential [71, 72].
ctDNA kinetics. On-treatment ctDNA decline/clearance provides an early, mechanism-anchored readout that may predict durable benefit and enable adaptive dose/sequence optimization across platforms [73, 74].
Oncogenic drivers and CMS. RAS/BRAF status, CMS subtypes and WNT-β-catenin activation correlate with exclusion; such features should guide inclusion/enrichment or rational combination choice (e.g., EGFR-IO rechallenge in ctDNA-confirmed RAS-WT) [75, 76].
Radiomics and peripheral immunology. Baseline and delta-radiomics capturing perfusion/texture and peripheral TCR clonality/myeloid ratios can complement ctDNA in MSS-focused trials [77].
Surgical and locoregional integration (peri-operative and oligometastatic care)
Curative intent for oligometastatic MSS CRC still hinges on resection/ablation/SABR. Rational IO integration for surgeons includes:
Timing.
Neoadjuvant priming (e.g., short “vascular normalization” window with anti-VEGF ± PD-1) to improve T-cell trafficking before resection/ablation [78].
Post-ablation/SABR consolidation PD-(L)1 to exploit antigen burst and potential systemic immunity [79].
Peri-operative immunology. Surgical stress can transiently suppress anti-tumor immunity; window-of-opportunity designs should sample PBMCs, TME biopsies, and ctDNA (pre-op; POD1-3; POD7-14; 6–8 weeks) to document whether we are truly “heating” tumors [80, 81].
Anatomical site strategy. In liver-dominant disease, consider hepatic re-conditioning (e.g., liver-directed RT/SABR in trials) before systemic dual-IO; extrahepatic-dominant patients may preferentially enter next-gen CTLA-4 + PD-1 or VEGFR-IO arms [70, 82].
Multidisciplinary governance. Build immune-toxicity readiness (hepatitis/colitis algorithms) into ERAS pathways; calibrate peri-operative steroids to avoid blunting IO priming when alternatives exist [83, 84].
What negative trials teach Us
The LEAP-017 result—no statistically significant OS improvement of lenvatinib + pembrolizumab over SOC—highlights several design lessons [53]:
- (i)Histology alone is not enough—stratify/enrich by metastatic pattern (liver vs. extrahepatic) and inflammatory gene programs [47, 85];
- (ii)Align endpoints with biology—incorporate ctDNA clearance, depth/duration of response, treatment-free survival [14, 86];
- (iii)Optimize sequence/dose—leverage the vascular-normalization window and RT fractionation to maximize immunogenicity [87, 88];
- (iv)Embed window-of-opportunity cohorts to mechanistically validate “heating” beyond radiology [89, 90].
Practical implications for today’s clinic
Outside trials: There is no broad guideline endorsement for IO combinations in unselected MSS mCRC at present [91].
Within trials (priority scenarios):
Non-liver-dominant refractory MSS mCRC → botensilimab + balstilimab or VEGFR-IO-based arms with translational cores [58, 74].
Up-front fit patients → intensification frameworks modeled on AtezoTRIBE (chemo + bevacizumab ± PD-L1) with explicit discussion of investigational status [52].
Oligometastatic disease → RT/ablation + ICI protocols that test dose/sequence and capture paired tissue + ctDNA serials [55, 56, 92].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rahma OE, Yothers G, Hong TS, Russell MM, You YN, Parker W, Jacobs SA, Colangelo LH, Lucas PC, Gollub MJ, Hall WA, Kachnic LA, Vijayvergia N, O’Rourke MA, Faller BA, Valicenti RK, Schefter TE, George S, Kainthla R, Stella PJ, Sigurdson E, Wolmark N, George TJ. Use of Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer: Initial Results From the Pembrolizumab Arm of a Phase 2 Randomized Clinical Trial. JAMA Oncol. 2021;7(8):1225–1230. doi: 10.1001/jamaoncol.2021.1683. Erratum in: JAMA Onc · doi ↗ · pubmed ↗
- 2Marron TU, Galsky MD, Taouli B, Fiel MI, Ward S, Kim E, Yankelevitz D, Doroshow D, Guttman-Yassky E, Ungar B, Mehandru S, Golas BJ, Labow D, Sfakianos J, Nair SS, Chakravarty D, Buckstein M, Song X, Kenigsberg E, Gnjatic S, Brown BD, Sparano J, Tewari A, Schwartz M, Bhardwaj N, Merad M. Neoadjuvant clinical trials provide a window of opportunity for cancer drug discovery. Nat Med. 2022;28(4):626–629. doi: 10.1038/s 41591-022-01681-x. Erratum in: Nat Med. 2022;28(8):1723. 10.1038/s 41591-022-01948- · doi ↗ · pubmed ↗