The Baby Triple P online positive parenting programme for mothers accessing community perinatal mental health care (the OPAL study): a feasibility study protocol
Anja Wittkowski, Henna Lemetyinen, Holly E. Reid, Trinity Perruzza-Powell, Lynsey Gregg

TL;DR
This study explores whether an online parenting program can be effectively offered to mothers with perinatal mental health issues and how acceptable it is to them and healthcare staff.
Contribution
This is the first study to examine the feasibility of a self-paced online parenting intervention in a NHS perinatal mental health service.
Findings
The study will assess recruitment, engagement, and retention rates of mothers in an online parenting program.
It will explore changes in maternal mental health, wellbeing, and mother-infant bonding after the intervention.
Interviews with mothers and staff will provide insights into the intervention's acceptability and implementation factors.
Abstract
Perinatal mental health difficulties can negatively impact maternal wellbeing, which in turn can impact the mother-infant bond. Although parenting interventions have been found to be effective, they are often not routinely offered in mental health services as additional psychosocial support. Thus, the aims of this study are a) to examine the feasibility of recruiting mothers, engaging them in an online parenting intervention and retaining them in the study and b) to explore the acceptability of this type of intervention in mothers and specialist perinatal mental health staff. We will also explore any changes in relevant outcomes for mothers. In this uncontrolled feasibility study, women experiencing moderate to severe mental health problems, who are in the later of stage of their pregnancy or mother to a baby up to 12 months old, will be recruited from a perinatal community mental…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
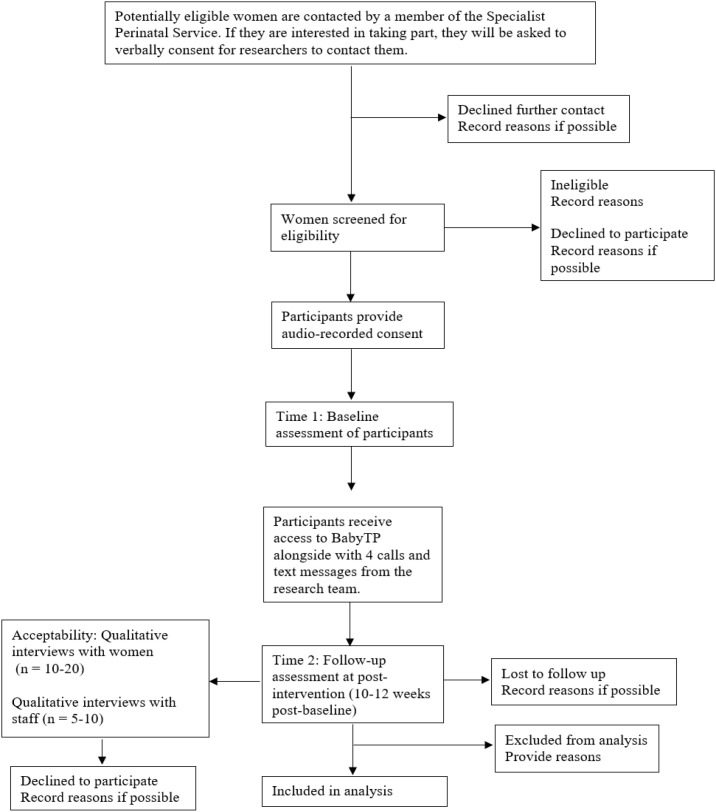 Figure 1
Figure 1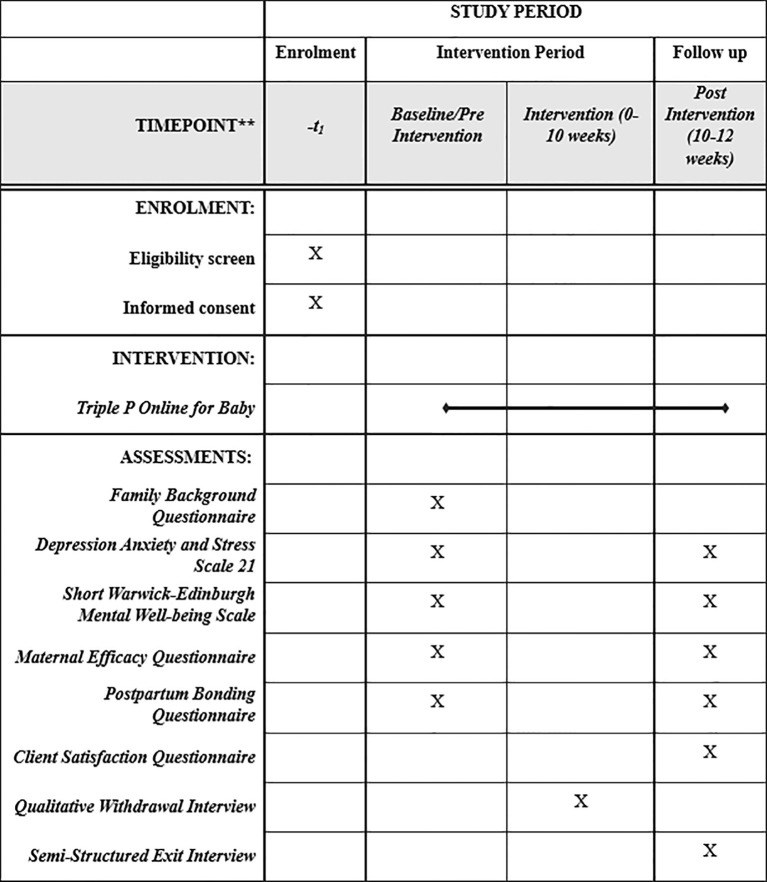 Figure 2
Figure 2| Session number | Session title | Session content |
|---|---|---|
| 1 | Positive parenting | Provides parents with an introduction to positive parenting as an approach to raising infants, factors that have an impact on early child development, and specific parenting strategies for developing a positive relationship with their baby. |
| 2 | Understanding your baby’s development | Parents are introduced to elements that can play a role in their baby’s development and ways they can monitor and keep track of their baby’s behaviour and development. |
| 3 | Developing a positive relationship | Parents learn strategies for developing a positive relationship with their baby and how to teach their baby new skills and behaviours. |
| 4 | Responding to your baby | Parents are helped to understand crying and teach settling techniques. Parents will also learn how to apply parenting strategies to promote positive sleeping habits. |
| 5 | Survival skills | Parents are introduced to changes new parents may experience, some of the early parenting traps, and a variety of coping strategies to manage emotions (e.g., stress, anxiety, sadness). |
| 6 | Partner support | Provides parents with information on common relationship changes new parents may experience and some partner traps. The importance of communication and ideas for maintaining relationship happiness are also introduced. |
| 7 | Conclusion | Parents are encouraged to think about how to implement the skills and knowledge they have learnt during the programme in the future. |
| Indicator | Green | Amber | Red |
|---|---|---|---|
| Recruitment: number of eligible participants recruited within our recruitment window of 29 weeks | ≥ 60% = green | 50–59% = amber | ≤ 49% = red |
| Study retention: proportion of participants completing measures at each data collection point (baseline and follow up) | ≥70% | 50-69% | ≤49% |
| Number | Outcome measure | Rationale | Item numbers and subscales | Scale type | Scoring range (minimum and maximum scores) and interpretation | Psychometric properties |
|---|---|---|---|---|---|---|
| 1 | Depression, Anxiety and Stress Scale-21 (DASS-21; | To measures levels of depression, anxiety and stress | 21 items: | 4- point Likert scale | 0-21 | Cronbach’s alpha-.76-.93 |
| 2 | Short Warwick Edinburgh Mental Wellbeing Scale (SWEMWBS; | To measure well-being | 7 items | 5-point Likert scale | 7-35 | Cronbach’s alpha-.88-.93 |
| 3 | Maternal Efficacy Questionnaire | To measure of parental self-efficacy | 20 items: | 4-point Likert scale | 20-80 | Cronbach’s alpha-.91 |
| 4 | Postpartum Bonding Questionnaire (PBQ; | Measures the difficulties in parent and infant bond | 25 items: | 5-point Likert scale | 0-125 | Cronbach’s alpha-.78-.79 |
- —Medical Research Council10.13039/501100000265
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Digital Mental Health Interventions · Child and Adolescent Psychosocial and Emotional Development
Introduction
1
Parenting interventions have consistently demonstrated strong effectiveness and efficacy in promoting positive developmental outcomes for both parents and children, with benefits ranging from improved parenting skills and reduced child behavioural problems to overall enhanced family functioning (1, 2). Among these interventions, the Triple P–Positive Parenting Program stands out as one of the most extensively researched, evidence-based, and scalable frameworks (3–7). Grounded in social learning theory, cognitive-behavioural, and developmental psychology, Triple P has been shown to reduce coercive parenting, increase parental self-efficacy, and significantly decrease child conduct problems across diverse populations and cultural contexts (3, 4, 7–11). Meta-analytic evidence further indicates that parenting programmes like Triple P foster long-term gains in child emotional regulation, decrease parental stress, and strengthen parent–child relationships, highlighting their value as both preventative and therapeutic tools (3, 4, 7, 8, 12, 13). Collectively, structured, evidence-based parenting interventions play a critical role in supporting family resilience, promoting healthy child development, and reducing the burden of mental health and behavioural difficulties across communities. Although the majority of evidence focuses on parenting programmes for preschool and school-aged children, similar principles of early relational and psychoeducational support underpin interventions designed for infants.
The transition to parenthood represents a major developmental milestone characterised by profound psychological, relational, and practical adjustments (14, 15). New parents frequently experience elevated stress, sleep disruption, and changes in couple functioning, all of which heighten vulnerability to perinatal mental health difficulties, such as depression and anxiety (16, 17). Parental mental health is closely intertwined with the quality of early caregiving behaviours (18, 19). Parental distress can undermine sensitive and responsive caregiving, whereas supporting parents to feel competent, regulated, and emotionally available strengthens the emerging parent–infant bond (20–22). This bond forms the foundation for infants’ emotional regulation, attachment security, and later socio-emotional development (15, 23–25). As interventions that support and strengthen parental wellbeing alongside early relationship-building are vital for fostering healthy developmental trajectories in both parent and child (26), there has been an increased focus by governments, especially in the United Kingdom (UK), to make the provision of early intervention, enhanced perinatal mental health services and support for vulnerable families a national priority (e.g., 27–29).
Triple P for Baby was developed to support new parents (e.g., mothers, fathers, etc.) transitioning to parenthood by targeting known modifiable risk and protective factors (30–32). It promotes realistic expectations about parenthood, the couple’s changing relationship, infant behaviour and development, whilst offering parenting skills training to increase parenting competence and adaptive strategies for emotion regulation. Through Triple P’s underlying self-sufficiency model (3–5, 13) Triple P for Baby also seeks to equip parents with knowledge and skills as well as the confidence to independently manage common parenting challenges. It promotes the development of a strong parent-infant bond, the strengthening of the parents’ coping resources and the improvement of both parents supporting each other whilst drawing on wider social support (30–32).
Triple P for Baby was originally designed as a four-session antenatal group intervention, followed by four postnatal individual telephone support sessions, but it has been delivered individually and postnatally only as well. Triple P for Baby’s acceptability and feasibility and potential benefits have been demonstrated in various studies including randomised controlled trials with primiparous and multiparous parents in diverse settings (e.g., 31–44). For example, a larger UK RCT involving first-time parent couples demonstrated strong compliance and engagement with the programme, indicating its practical acceptability (38). However, a follow-up sensitivity analysis of a sub-sample of data revealed limited effects on the couple relationship, social support and parenting skills. But caution should be exercised in the interpretation of these findings because the sub-sample was underpowered (38). Furthermore, a large UK RCT comparing an enhanced version of Triple P for Baby and Mellow Bumps against standard care in a group of women with complex social and care needs did not demonstrate efficacy for any parenting intervention in improving mental health and wellbeing outcomes for women in this context of heightened social complexity (37).
Despite being a universal parenting intervention, Triple P for Baby has also been explored as an additional treatment for women with mental health problems; for example, in a pilot RCT with mothers experiencing postnatal depression reported high levels of participant engagement and satisfaction (42). Furthermore, a multi-site feasibility RCT evaluated the individually and postnatally delivered intervention in a perinatal mental health setting (psychiatric Mother and Baby Unit) and reported that 75% of mothers completed the intervention, which these mothers also rated as highly acceptable (44). Clinical outcomes signalled potential improvements in parenting competence, bonding, mood and mental health symptomatology, but a full trial in a specialist perinatal mental health setting in the UK has yet to be undertaken. Finally, a full RCT in an urban Kenyan setting, with Afrikan mothers experiencing depression and anxiety, showed improvements in maternal mental health outcomes, but no significant difference was found in maternal self-efficacy between the mothers who did and those who did not access Triple P for Baby (33).
The COVID-pandemic in 2020 accelerated the development of online interventions including a seven-session, self-paced, self-guided, interactive version of Triple P for Baby Online. It is highly accessible (via laptop, tablet or phone) to parents of infants, minimising the need for external childcare to attend the intervention in person and, given its interactive content with brief video-clips, it is also suitable for people with different literacy and educational levels. Online versions of Triple P have been shown to be as effective as other modalities in general population samples (3, 4, 45). In 2022, a national rollout of Triple P Online took place across Australia which allowed all families with children under 12 years of age across the country free access to Triple P’s evidence-based suite of online programmes, including the intervention for parents of babies (46). Similarly, the strength of Triple P for Baby’s existing evidence and its ability to support parental wellbeing and the parent-infant-relationship led the Department of Health and Social Care and NHS England in 2021 to commission the training of 680 practitioners in this intervention as part of the Start for Life/Family Hub offer for 75 local authorities (47). Many local authorities also commissioned the delivery of Triple P for Baby Online to address the Department of Work and Pensions’ Reducing Parental Conflict Programme (48) and the Supporting Families Outcome Framework (49).
With an increasing emphasis on digital approaches to improving mental health care, the proposed project allows us to explore the feasibility and acceptability of this parenting intervention whose online version has not yet been tested in a perinatal mental health context. Triple P for Baby Online is an ideal supplementary intervention to strengthen parenting competence, the parent-infant bond and partner support – important factors which are not always targeted by perinatal mental health services.
Up to 27% of women experience maternal mental illness in the perinatal period (50), with maternal suicide being the leading cause of death for women between six weeks and one year after pregnancy in the UK (51). In the UK, perinatal mental health services have been expanded to improve access to assessment and treatment for women as a public health priority (29, 52, 53). This increased access is expected to minimise the risks that maternal mental illness can pose for the development of bonding and attachment difficulties between mother and baby and any subsequent negative impacts on the child’s development (18, 54, 55).
The type and severity of the woman’s mental health problem in the perinatal period will determine the type of intervention offered (56). In England, 81,975 women were referred to a specialist perinatal mental health service from 04/2023-03/2024, with 66.65% (n=54,635) having a first face-to-face appointment (57). If accepted by a perinatal mental health service women are offered psychological interventions (predominantly focused on the mother) (58–60), usually delivered individually or in a remote group format by two facilitators, depending on mental health severity and safeguarding concerns. Couples therapy to reduce relationship conflict during the perinatal period is not offered consistently, if at all. Parent-infant psychotherapy referrals are made only for bonding difficulties. Given the substantial long-term negative effects of early adverse experiences (18, 55) and the capacity of positive relationships to buffer these effects (61, 62), strengthening the mother-infant-relationship is important (63). However, parenting interventions are not routinely offered in perinatal services, despite their established evidence-base in improving child and parent outcomes and reducing child maltreatment.
By examining the feasibility and acceptability of Triple P for Baby Online as a supplementary intervention, this study is the first step towards insights related to improvements in intervention access and mother and infant support in specialist perinatal services. Thus, the aims of this uncontrolled study are 1) to examine the feasibility of recruiting and engaging mothers with perinatal mental health difficulties in an online parenting intervention and retaining them in the study and 2) to explore the acceptability of this type of intervention in mothers and perinatal mental health staff. We are also interested in exploring any implementation factors associated with engagement and retention and if there is any change over time in outcome measures of maternal mental health, wellbeing, maternal self-efficacy and the perceived mother-infant bond.
Methods
2
Design
2.1
The study is an uncontrolled feasibility study, with a qualitative component exploring the intervention’s acceptability with participating mothers and staff. Indicators for psychological change over a ten-week follow-up period will be explored by pre- and post-intervention outcome measures. This uncontrolled, pre- and post-intervention design was chosen to focus on acceptability and feasibility of the intervention and to collect data to determine if the study procedures, outcome questionnaires and Treatment As Usual (TAU) as a comparative arm for a future trial are feasible.
Figure 1 provides an overview of the study design based on CONSORT guidelines (64). For transparency, this protocol is reported in line with the SPIRIT checklist for protocols of randomised trials (65), although any items related to randomisation and blinding (21a-24c) have been omitted from this protocol because we are describing a non-randomised trial. The TIDieR checklist for the reporting of interventions (66) has also been used (see Supplementary Materials).
CONSORT diagram showing study design.
Ethical approvals and research governance
2.2
The study has been approved by the National Health Service (NHS), Health Research Authority and the Greater Manchester Mental Health NHS Foundation Trust (IRAS ID: 352080). It will be conducted in accordance with the local legislation and institutional requirements. Amendments to ethical approval will be sought in the event of protocol modification. Participants will provide informed consent to participate in the study. The University of Manchester will provide oversight as the study sponsor. All staff will be trained in research governance principles (e.g., Good Clinical Practice, data protection and information governance). A Patient and Public Involvement and Engagement (PPIE) group comprising mothers with lived experience of perinatal mental health difficulties will be consulted on various aspects of the study such as content of the support calls and text messages and the topic guide. The PPIE group will convene at four scheduled meetings during the study and provide support via email between meetings. The intervention is low risk so there will not be a standard provision of ancillary and post-trial care.
Study setting
2.3
In this single site study, participants will be recruited from a specialist perinatal mental health community-based service, covering three large geographical areas in Greater Manchester, England, for women experiencing moderate to severe mental health problems in the perinatal period. Women referred to the service are assessed and, if eligible, assigned to a particular treatment pathway (e.g., the psychology pathway or the occupational therapy pathway). For this study, we will recruit from the psychology pathway. Mothers assigned to this pathway are typically offered individual or group specialist psychological interventions to meet their complex needs.
Inclusion and exclusion criteria for participants
2.4
Participants are eligible if they are a) in the third trimester of pregnancy or the mother or birthing parent of an infant aged birth to 12 months, with whom they live, or have parental responsibility for, b) aged 18 years or older, c) proficient in English to engage with the intervention and complete assessments (and take part in interviews), d) capable of giving informed consent. Participants also need to have been accepted onto the psychology pathway of the service and own or have access to a smartphone, tablet, laptop or computer to access the intervention. As Triple P for Baby Online is a supplementary intervention that participants can engage with alongside any psychological treatment, participants will not be excluded if they engage in other interventions typically offered by this service. Participants will be excluded if they are or become inpatients at the time of recruitment, because inpatient admission usually signals that additional risk factors are present (e.g., suicidal ideation or behaviours) that cannot easily be managed in a community setting.
Sample size considerations and recruitment
2.5
We plan to recruit a minimum of 30 participants, which is a typical and recommended sample size for feasibility studies (67, 68). As codes for the intervention are only available for 100 participants as a minimum, we could recruit up to 100 participants.
Potential mothers will be identified by perinatal mental health staff, such as the team’s clinical psychologist or assistant psychologist. Staff will consider who on their waiting lists or caseloads might be eligible and then provide them with brief information about the study in the form of an advert, or a brief study summary. Members of the research team will also attend weekly referral and allocation meetings to support staff with recruitment and potential participant identification and reduce potential selection bias. If staff have concerns about a woman’s capacity or mental state (e.g., suicidal ideation or behaviours), they would not consider that participant to be eligible.
Mothers (and birthing parents) interested in taking part will be asked for verbal consent to be contacted by a member of the study team who will then contact them to provide further information and conduct an eligibility screening. Alternatively, potential participants can self-refer to the study via a link in the study advert which staff can email to interested mothers. Potential participants will be provided with a participant information sheet and given at least 48 hours to read it. A follow-up phone call will be arranged for a mutually convenient time to answer any questions and discuss their interest in taking part. Reasons for non-participation will be collected and anonymised with potential participants’ verbal consent to inform feasibility and acceptability.
Eligible individuals who decide to participate will be enrolled to the study. A researcher will obtain their audio-recorded informed consent to take part in the study including personal identifiable information (e.g., full name, date of birth) and complete a pseudonymised electronic copy of the consent form. Identifiable information will be stored securely and separately from the study data and deleted once it is no longer needed for study purposes. The audio-recorded consent and the pseudonymised consent form will also be stored separately from one another to maximise data protection. Baseline assessment may also be conducted or started at this appointment (depending on participant preference).
Using convenience sampling, ten to 20 mothers who have participated in the study for at least seven weeks will be invited to take part in interviews to explore study and intervention acceptability qualitatively. If a large number of participants indicate interest in attending an interview, we will prioritise contacting participants with different demographic characteristics and engagement with the intervention and/or the study procedures to capture diverse views and experiences. For staff interviews, we will purposively sample five to ten staff to include a range of job roles and perinatally relevant work experience. Staff are eligible to take part if they are a healthcare professional working for this service (e.g., a clinical or counselling psychologist, CBT therapist, nursery nurse, team leader, assistant psychologist). They will be excluded if they have been in post for less than six months to ensure staff participants are familiar with the service and its service users. Separate consent to take part in an interview will be sought from mothers and staff.
The intervention and its delivery
2.6
In this study, participants will be offered the Triple P Positive Parenting Program for Baby (11, 30–32, 69), which aims to increase parenting skills and confidence in parents of infants (up to 12 months) by targeting the parent-baby bond, increasing the parent’s understanding of infant development, responding to the baby’s cues in a way that supports infant mental health and learning to communicate effectively with the partner/co-parent or another family member. All participants will be offered access to the self-paced Triple P for Baby Online intervention, with content offered in seven brief sessions, which are accessed online as a series of videos featuring parents discussing their experiences of various aspects of parenting in the first year and a narrator sharing factual information about infant development and parenting (see Table 1 for details).
After completion of the baseline measures, the research team will provide participants with a link to register for Triple P for Baby Online. Following registration, participants will have 12 months of access to the intervention via an internet−connected device (e.g., laptop, smartphone, or tablet), at a location and time of their choice. Participants will be asked and encouraged to complete all seven sessions of the intervention within ten weeks (a timeframe chosen to account for busy perinatal periods). Participants’ care and treatment from the specialist perinatal service will continue as usual while they take part in the study; this care might include care-coordination and psychological interventions (e.g., compassion-focused therapy, cognitive behavioural therapy, eye movement desensitisation and reprocessing therapy, dialectical behaviour therapy, cognitive analytic therapy, delivered individually or as part of an online group intervention).
To support and maximise engagement and answer any questions the mother may have about the intervention, study staff will offer encouraging prompts via text messages and brief phone calls to check on their progress (prior to session 1 to help with access, then after sessions 1, 3 and 5). These phone calls will also act as ‘trouble shooting’ support for any technical or comprehension issues and they will also enable the research team to check for any adverse events.
Feasibility outcomes
2.7
Feasibility will be assessed by examining data related to recruitment and study retention (i.e. completion of outcome measures at follow up). To evaluate the suitability of this study to progress to a larger, randomised trial, we will use the red, amber, green (RAG) system and pre-determined progression criteria (70–72). Table 2 provides an overview of our proposed progression criteria. We will also report on a range of feasibility indicators (e.g., number of potential participants found to be eligible, reasons for declining to participate, the extent and pattern of missing data, the number of related adverse events, etc.). In addition, the Triple P Online Management system will allow the research team to monitor participants’ progress through the programme and aggregate relevant feasibility data on engagement (e.g., how many and what sessions were completed, dates of first and last log-ins, number of log-ins per participant).
Acceptability outcomes
2.8
Intervention acceptability will be assessed quantitatively via the Client Satisfaction Questionnaire (73), administered to participants at follow up via the online survey tool, Qualtrics. Participants will be asked to answer 13 questions (rated on a 7-point Likert scale) and three open-ended questions (e.g., Do you have any other comments about the programme)?.
Qualitative exploration of acceptability will be conducted via online interviews with a sub-group of participants and staff. Acceptability in this context will focus on the exploration of attitude towards the intervention, intervention and assessment burden, and facilitators and barriers towards uptake and engagement with the intervention, as informed by Sekhon et al.’s (74) theoretical framework of acceptability.
Separate consent for this aspect of the study will be sought. Interviews will explore participants’ views of the intervention content, mode of delivery, the encouraging phone calls and text messages, and the study procedures, such as assessment burden. We will also conduct exit interviews with mothers who withdraw from the study, if possible.
Questionnaire outcomes
2.9
At baseline, mothers will be asked to complete the Family Background Questionnaire (75), adapted for perinatal populations, which will ask for details of their ethnicity, the age and sex of their baby, family and household composition, their marital and employment status and brief details about characteristics and experiences that may predict attrition and outcome, such as psychiatric history, educational attainment and family support. The type and duration of standard care that mothers have received while participating in the study will be recorded to report what other treatments mothers (or birthing parents) were offered and then accessed; this will test the feasibility of using Treatment As Usual (TAU) as a comparative arm for a future trial.
Participants will also be asked to complete four brief validated questionnaires assessing mood (i.e., depression, anxiety, stress), wellbeing, maternal self-efficacy and the perceived mother-infant bond, chosen for their relevance, their psychometric properties and widespread use in related research (see Table 3 for further details). They will be asked to complete these questionnaires via the online survey tool, Qualtrics, either on their own or with the support of a researcher over a telephone or video call on Microsoft Teams. At follow up (i.e., 10–12 weeks post-baseline), participants will be reminded to complete the same four questionnaires. At the same time, we will also ask them to complete the Client Satisfaction Questionnaire (73). The assessments are anticipated to take up to 30 minutes to complete. Figure 2 provides an overview of all study data collection points.
SPIRIT figure for the study.
Participants will be encouraged and reminded to complete the follow-up questionnaires via email, text message and phone call, and asked if they would prefer to complete the measures with the assistance of a researcher. All data will be pseudonymised and entered into a database, stored on a secure server, by the research assistant and checked for accuracy and quality by the joint project managers.
Safety considerations
2.10
Adverse events will be monitored and reported throughout the study in line with sponsor and site reporting systems. A log of all adverse events will record all unexpected adverse events as well as reports of significant or sustained deterioration in the mental health of the participant caused by the intervention during the trial period (date of first contact to final contact). Any such deteriorations will be designated serious adverse events for the purposes of this study, even when hospitalisation is not required. Adverse events will primarily be self-reported to the research team or identified by the research team as part of their routine assessments. Enquiries about adverse events will be made by the project managers. The research team will determine if the event qualifies for expedited reporting. The intervention is low risk and we do not anticipate stopping the study; however, in the unlikely event that any serious adverse events are attributed to participation in the study, the study will be stopped.
We will inform any participant’s General Practitioner (GP) or family doctor of her participation as well as the named perinatal mental health practitioner (e.g., a Case Manager or a Clinical Psychologist) so that they are aware of the participant taking part in the study. Participants are also informed before providing consent and at the time of formal consenting that if they disclose information to the study team suggesting that either the participant or someone else is at risk of harm, the study team may have to inform authorities, such as the participant’s GP or the police. The participant will be involved in the decision as much as possible.
The research team is trained in adult and child safeguarding and in risk and distress management in perinatal mental health and parenting research contexts. The team has conducted a written risk assessment for the study and developed a Sponsor and Trust approved protocol for managing risk and distress before, during and after participant contact to ensure duty of care towards participants. If a researcher observes potential signs of mental health deterioration, the observation will be shared with the participant’s named mental health practitioner and GP. If the participant is assessed to pose an imminent risk to either herself or to someone else, the risk will be discussed with the Chief Investigator (who is also a registered Perinatal Clinical Psychologist) and, if considered appropriate, the researcher will contact emergency services.
Participants may continue to access the intervention for up to 12 months after registration if they so wish. This means participants can access supplementary aftercare in addition to usual care they are already accessing or entitled to via the perinatal mental health service.
Data analysis
2.11
Participant flow through the study will be reported using the CONSORT diagram (Figure 1). Descriptive summaries will be produced for feasibility and other outcome data (e.g., means and standard deviations or numbers and percentages, including percentages and patterns of missing data). We will use a paired t-test or Wilcoxon signed rank test for pre- and post-intervention questionnaire data and the reliable change index (80, 81) to explore changes in clinical outcomes (i.e., potential intervention benefits). However, given that this is an uncontrolled study, any results in relation to outcomes will be treated with extreme caution.
All interview data will be digitally recorded, transcribed verbatim and then analysed using Framework Analysis (82, 83). Informed by the acceptability of healthcare interventions theoretical framework (74), an initial coding framework will be developed to reflect key service and service user-determined topics covered by the interview schedule. Following data familiarisation, this framework will be augmented to encompass new emerging themes. Initially, a subset of transcripts will be coded independently by a member of the research team, and findings will be discussed by the rest of the research team and the PPIE group to develop a shared theoretical framework. This framework will then be applied to the remaining transcripts. Data will be interpreted and analysed within the final framework to structure and compare participant and staff views about the study and intervention. The trustworthiness of the final analysis will be enhanced through the integration of data from different stakeholders and through researcher triangulation.
Given the small-scale uncontrolled nature of this trial, a data monitoring committee was not deemed necessary. Instead, the research team conducted monthly trial monitoring meetings, and the project managers regularly conducted a review of trial documents.
Discussion
3
This will be the first study to examine the feasibility and acceptability of a self-paced parenting intervention, Triple P for Baby Online, offered to mothers in a NHS perinatal community mental health service. It will also be the first study to explore the possible benefits of this specific parenting intervention, delivered online as a self-paced programme, in mothers with moderate to severe mental health problems in the perinatal period. This study will also allow us to explore any pragmatic issues that will inform a larger trial, such as the recruitment pathway, the acceptability of the intervention and study procedures to mothers as well as perinatal mental health staff. We will identify how the intervention needs to be tailored or refined to meet the needs of this clinical group of service users in specialist perinatal community mental health settings. As it is expected that participants will present with a range of perinatal mental health problems, differences in childrearing practices and parenting concerns and different levels of parenting confidence in addressing these, this study will allow us to gauge the appropriateness of the intervention content and the practicalities of engaging with the sessions during the perinatal period, whilst under the care of a specialist perinatal mental health service.
This study will enable us to determine if progression to a full trial is indicated or not. If it is, then the current study will allow us to consider the needs for any amendments that may help recruitment and retention outcomes (e.g., the timepoint of study enrolment and intervention offer, changes to outcome measures, and content and frequency of the supportive check-in calls and text messages).
Finally, this study will also help us determine what type of training and what level of support our PPIE group members may wish to see to strengthen their involvement and support their engagement with a future trial.
The research team intends to disseminate outcomes from this study in peer-reviewed open access journals and at relevant conferences. Participants will be provided with a lay summary of the findings if they indicated that they wish to receive this information and consented to this information being emailed to them. Recruitment started in May 2025 and is ongoing. The study is set to be completed by end of February 2026.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Barlow J Bergman H Kornør H Wei Y Bennett C . Group-based parent training programmes for improving emotional and behavioural adjustment in young children. Cochrane Database Systematic Rev. (2016) 8:Article CD 003680. doi: 10.1002/14651858.CD 003680.pub 3, PMID: 27478983 PMC 6797064 · doi ↗ · pubmed ↗
- 2Furlong M Mc Gilloway S Bywater T Hutchings J Smith SM Donnelly M . Behavioural and cognitive-behavioural group-based parenting programmes for early-onset conduct problems in children aged 3 to 12 years. Cochrane Database Systematic Rev. (2022) 3:Article CD 008225. doi: 10.1002/14651858.CD 008225.pub 2, PMID: 22336837 PMC 12935172 · doi ↗ · pubmed ↗
- 3Sanders MR . Triple P–Positive Parenting Program: Towards an empirically validated multilevel parenting and family support strategy for the prevention of behavior and emotional problems in children. Clin Child Family Psychol Rev. (1999) 2:71–90. doi: 10.1023/A:1021843613840, PMID: 11225933 · doi ↗ · pubmed ↗
- 4Sanders MR . Development, evaluation, and multinational dissemination of the Triple P–Positive Parenting Program. Annu Rev Clin Psychol. (2012) 8:345–79. doi: 10.1146/annurev-clinpsy-032511-143104, PMID: 22149480 · doi ↗ · pubmed ↗
- 5Sanders MR Markie-Dadds C Turner KMT . Theoretical, scientific and clinical foundations of the Triple P–Positive Parenting Program. Aust Psychol. (2003) 35:136–49. doi: 10.1080/00050060008257960, PMID: 41735180 · doi ↗
- 6Turner KMT Sanders MR . Dissemination of evidence-based parenting and family support strategies: Learning from the Triple P–Positive Parenting Program system approach. Aggression Violent Behav. (2006) 11:176–93. doi: 10.1016/j.avb.2005.07.005, PMID: 41743167 · doi ↗
- 7Sanders MR Kirby JN Tellegen CL Day JJ . The Triple P–Positive Parenting Program: A systematic review and meta-analysis of a multi-level system of parenting support. Clin Psychol Rev. (2014) 34:337–57. doi: 10.1016/j.cpr.2014.04.003, PMID: 24842549 · doi ↗ · pubmed ↗
- 8Li N Peng J Li Y . Effects and moderators of the Triple P–Positive Parenting Program on children’s social, emotional, and behavioral problems: Systematic review and meta-analysis. Front Psychol. (2021) 12:719145. doi: 10.3389/fpsyg.2021.719145, PMID: 34512467 PMC 8427298 · doi ↗ · pubmed ↗