Pulmonary Tumor Thrombotic Microangiopathy in a Patient With Male Breast Cancer: A Report of a Rare Case
Keiichi Miyashita, Yoshiaki Ito, Hideki Kaneko, Kentaro Nabata, Akiko Kawasumi, Yuya Murata, Akira Matsui, Shigeo Okuda

TL;DR
A rare case of pulmonary tumor thrombotic microangiopathy is reported in a male patient with breast cancer, emphasizing the need for early recognition in rare cancers.
Contribution
This is the first English-language report of PTTM arising from male breast cancer.
Findings
PTTM was diagnosed postmortem in a male breast cancer patient with progressive respiratory failure.
Autopsy confirmed tumor emboli and fibrous intimal thickening in pulmonary arteries.
The case underscores the importance of considering PTTM in rare malignancies with unexplained respiratory symptoms.
Abstract
Pulmonary tumor thrombotic microangiopathy (PTTM) is a rare but serious complication that can occur in patients with advanced cancer. It often leads to rapidly worsening respiratory failure and right heart failure and is typically diagnosed only postmortem. While PTTM has been reported in various cancers, it is extremely rare in male patients with breast cancer, which is itself an uncommon malignancy. We report the case of a man with hormone receptor-positive breast cancer who underwent surgery followed by adjuvant chemotherapy. Several months later, he developed progressive dyspnea and increased levels of tumor markers. Although contrast-enhanced computed tomography (CT) scans revealed no evidence of pulmonary thromboembolism, the patient's right heart failure rapidly worsened, and he died shortly after hospital admission. Autopsy revealed classic histopathological features of PTTM,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
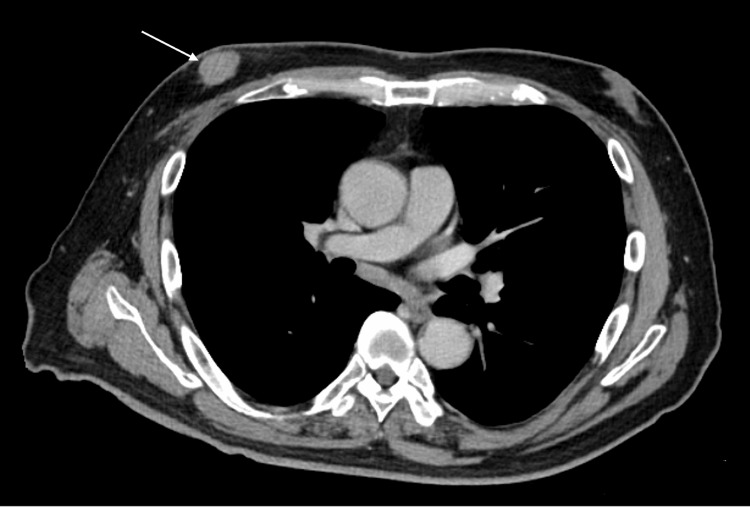 Figure 1
Figure 1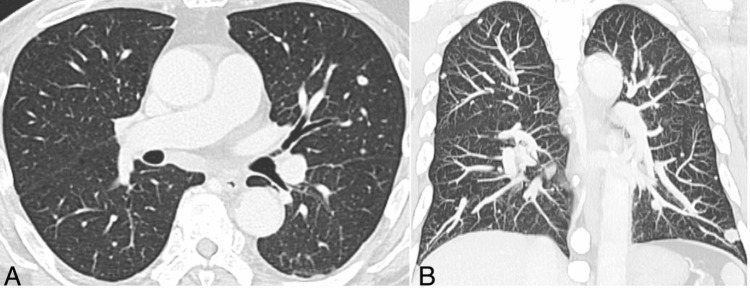 Figure 2
Figure 2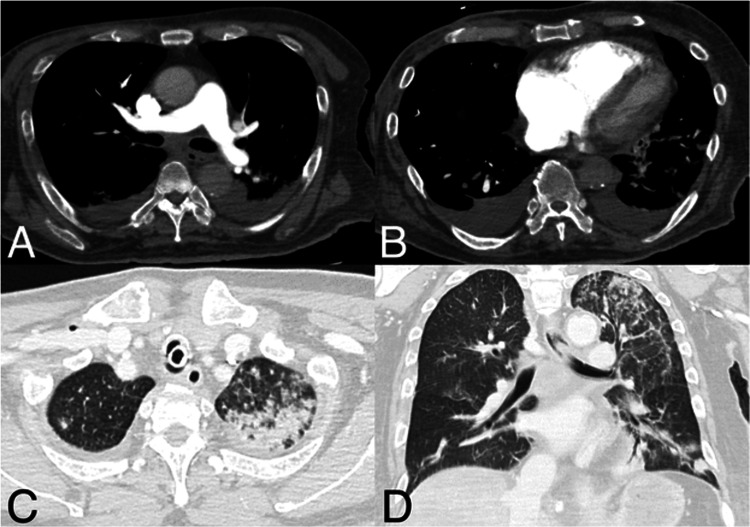 Figure 3
Figure 3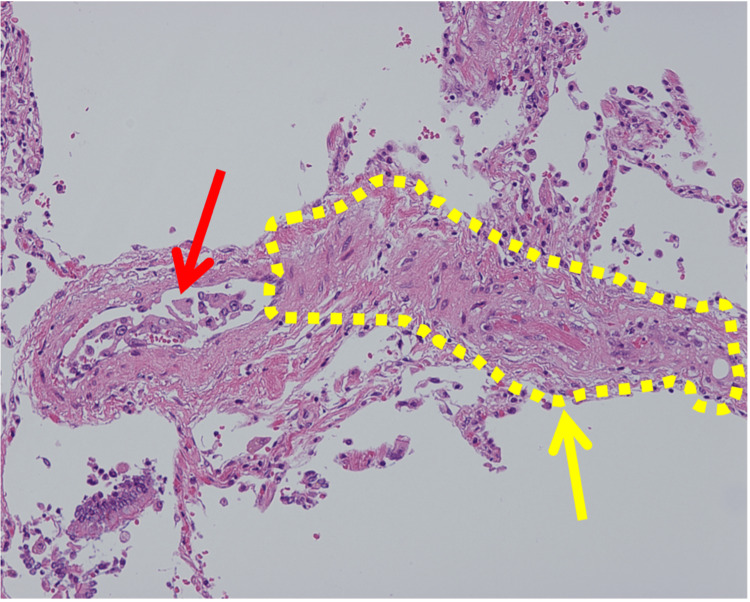 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Chemotherapy-induced cardiotoxicity and mitigation · Complement system in diseases
Introduction
Pulmonary tumor thrombotic microangiopathy (PTTM) was first described as a distinct clinicopathological condition in 1990 [1]. It is a rare and highly lethal complication of malignancy characterized by tumor embolization within the pulmonary vasculature and activation of the coagulation cascade, leading to progressive pulmonary hypertension, acute hypoxemic respiratory failure, and right heart failure, often culminating in death within days [2]. In the clinical setting, the true incidence of PTTM remains uncertain because most cases are diagnosed postmortem. In an autopsy-based series, 21 of 630 carcinoma cases (3.3%) were diagnosed with PTTM [1], suggesting that it is an uncommon but likely under-recognized complication of advanced malignancy. Histologically, PTTM is defined by widespread microscopic tumor emboli accompanied by fibrocellular intimal proliferation and progressive luminal narrowing of small pulmonary arteries, thereby distinguishing it from more common entities such as pulmonary thromboembolism (PTE) [3].
PTTM is most commonly associated with gastric cancer, which accounts for approximately 59% of reported cases. Other primary tumors include breast cancer (approximately 10%) and lung cancer (approximately 6%). The majority of PTTM cases arise from adenocarcinomas [2].
Although breast cancer is a recognized primary site of PTTM, nearly all reported cases involve female patients. PTTM arising from male breast cancer is extremely rare and is largely absent from the English literature. The scarcity of reports on male patients likely mirrors the low incidence of male breast cancer. However, given the extreme lethality of PTTM and the limited number of documented cases of male breast cancer, reporting additional cases is valuable to expand the clinical literature and reinforce awareness that PTTM can occur in breast cancer patients irrespective of sex.
Case presentation
A man in his 70s presented to our hospital in April 2023 with a chief complaint of a right nipple mass (Figure 1). A core needle biopsy confirmed the diagnosis of invasive ductal carcinoma. His past medical history revealed lifestyle-related diseases, including angina pectoris and diabetes; however, he had no family history of breast or ovarian cancer.
Contrast-enhanced axial chest computed tomography on initial presentationContrast-enhanced axial chest computed tomography image showing a well-defined, homogeneously enhancing 2.3-cm mass located immediately beneath the right nipple, representing the primary breast tumor.
In June 2023, he underwent a right mastectomy with axillary lymph node dissection. Postoperative pathological diagnosis revealed luminal B-type invasive ductal carcinoma, which was staged as pT4bN1miM0, pStage IIIB (American Joint Committee on Cancer (AJCC) classification). Given the high risk of recurrence, adjuvant chemotherapy was initiated postoperatively. The treatment plan consisted of four cycles of fluorouracil, epirubicin, and cyclophosphamide (FEC) followed by four cycles of docetaxel (DTX). At the time of disease progression, the patient had completed three cycles of DTX and was still receiving adjuvant chemotherapy.
Eight months after surgery, elevated serum tumor markers (CA15-3: 75.5 U/mL; CEA: 9.8 ng/mL) were noted after the completion of three cycles of DTX. As recurrence or progression during adjuvant therapy is relatively uncommon in breast cancer, postoperative computed tomography (CT) imaging was planned after the completion of the fourth DTX cycle. However, approximately one month later, the patient developed acute respiratory deterioration before scheduled imaging could be performed. Contrast-enhanced CT revealed no evidence of PTE; however, thrombocytopenia and a markedly elevated D-dimer level raised suspicion of disseminated intravascular coagulation (DIC), prompting hospital admission and the initiation of heparin therapy. Pulmonary nodules present prior to surgery had increased in size, suggesting disease progression with pulmonary metastasis (Figure 2).
Chest computed tomography demonstrating multiple pulmonary nodulesChest computed tomography images. (A) Axial view and (B) coronal maximum intensity projection image demonstrating multiple randomly distributed pulmonary nodules in both lungs, with interval increases in number and size compared to the previous examination, suggestive of pulmonary metastases.
On the third day of hospitalization, the patient developed sudden respiratory distress, culminating in cardiopulmonary arrest. Return of spontaneous circulation (ROSC) was achieved after resuscitation efforts. Transthoracic echocardiography (TTE) revealed marked right ventricular strain. Follow-up contrast-enhanced CT ruled out PE but revealed right ventricular enlargement, contrast reflux into the inferior vena cava, a periportal collar sign, edematous thickening of the gallbladder wall, and bilateral pleural effusions, without evidence of pericardial effusion, indicating acute right heart failure secondary to right ventricular overload (Figure 3).
Contrast-enhanced computed tomography on the third day of hospitalizationContrast-enhanced computed tomography findings. (A) No pulmonary thromboembolism is observed in the pulmonary arteries. (B) Right ventricular enlargement, contrast reflux into the inferior vena cava, and bilateral pleural effusions are present. Periportal collar signs and subserosal edema of the gallbladder (not shown) are noted, suggesting acute right heart failure secondary to right ventricular overload. (C, D) Centrilobular nodular opacities, consolidation, and interlobular septal thickening were observed in the left upper lobe, and inflammatory changes and carcinomatous lymphangitis were considered in the differential diagnosis.
Additionally, centrilobular nodular opacities, consolidation, and interlobular septal thickening were observed in the left upper lobe, with inflammatory changes and carcinomatous lymphangitis considered in the differential diagnosis (Figure 3). Despite intensive care, the patient's respiratory and hemodynamic status deteriorated rapidly, leading to death on the same day.
An autopsy revealed PTTM secondary to metastatic breast carcinoma. Histopathological examination revealed classic features of PTTM, including tumor emboli within small pulmonary arteries, fibrous intimal thickening, and fibrin thrombus formation (Figure 4). Further findings included carcinomatous lymphangitis and widespread metastases to the bilateral hilar and tracheobronchial lymph nodes, liver, bone marrow, small intestine, and bilateral adrenal glands. Notably, metastases to the liver, small intestine, and adrenal glands and diffusely to the bone marrow were not clearly identifiable on CT imaging.
Histopathological findings of pulmonary tumor thrombotic microangiopathyHistopathological findings of the lung (H&E staining). The red arrow indicates tumor emboli within a small pulmonary artery, while the yellow arrow highlights fibrocellular intimal proliferation and fibrin thrombus formation within the vessel.
Discussion
While PTTM has most commonly been reported in association with gastric adenocarcinoma, breast cancer is also recognized as a frequent primary tumor site for PTTM [2,3]. However, to the best of our knowledge, no cases of PTTM arising from male breast cancer have been reported in the English-language literature.
Male breast cancer itself is an uncommon entity, accounting for less than 1% of all breast cancer cases [4]. Its rarity likely contributes to the underrepresentation of male breast cancer-associated PTTM in the literature. In addition, many PTTM cases are only diagnosed postmortem, which may further obscure the true incidence of PTTM in male breast cancer patients [2,3].
In our case, the patient presented with a rapidly progressive respiratory decline following a history of high-risk, hormone receptor-positive breast cancer treated with surgery and adjuvant chemotherapy. The clinical picture, including right ventricular overload, elevated D-dimer, and lack of radiographic evidence for conventional PTE, raised clinical suspicion for PTTM, though the diagnosis was only confirmed postmortem. Previous reports note that PTTM commonly shows a laboratory pattern of elevated D-dimer, increased lactate dehydrogenase (LDH), and thrombocytopenia [2,3].
Chest CT findings in PTTM have been reported in the literature, including ground-glass opacities (82%), small nodules (86%), mediastinal or hilar lymphadenopathy (91%), and interlobular septal thickening (81%) [2]. While these findings may occur with notable frequency, they are often mild in appearance and lack specificity, making early diagnosis extremely challenging. Moreover, such findings are not pathognomonic for PTTM and may overlap with other pulmonary pathologies, such as lymphangitic carcinomatosis or interstitial lung diseases.
Given these limitations, additional imaging modalities have been explored to improve diagnostic yield. In particular, dual-energy CT and perfusion scintigraphy can provide functional information about regional pulmonary perfusion [5-8]. In some cases, impaired peripheral blood flow due to tumor emboli may be visualized as multiple wedge-shaped perfusion defects in the lung periphery. Although these findings are also nonspecific, they may offer supportive evidence and help raise clinical suspicion for PTTM when interpreted in the appropriate clinical context. In the present case, however, the patient's clinical condition deteriorated rapidly, and additional advanced imaging modalities were not feasible given the acute clinical course.
Although antemortem diagnosis of PTTM remains challenging, several invasive diagnostic approaches have been reported, including cytologic examination from a wedged pulmonary artery catheter and transbronchial or video-assisted thoracoscopic lung biopsy [9-11]. However, these are often contraindicated due to severe hypoxemia or pulmonary hypertension, which frequently preclude safe tissue sampling.
In clinical practice, PTTM should be suspected when a patient with a known malignancy develops rapidly progressive dyspnea, signs of pulmonary hypertension or right ventricular strain, elevated D-dimer levels with or without thrombocytopenia, and no evidence of conventional PTE on contrast-enhanced CT. The presence of nonspecific CT findings, such as small nodules, interlobular septal thickening, or ground-glass opacities, may further support this suspicion in the appropriate clinical context.
Although the prognosis of PTTM remains poor, early recognition may allow for the timely modification of systemic therapy in selected patients. Prior reports have described temporary clinical stabilization following chemotherapy or targeted agents; however, the overall outcomes remain unfavorable [6-10]. Accordingly, heightened clinical suspicion may offer a limited but potentially meaningful opportunity for therapeutic interventions.
Conclusions
PTTM is a rare but fatal complication of advanced malignancies and remains difficult to diagnose without tissue confirmation. To our knowledge, this is the first English-language report of PTTM arising from breast cancer in males. This case highlights that PTTM may occur in patients with breast cancer, irrespective of sex. Although CT findings are often nonspecific, dual-energy CT or scintigraphy may be helpful in evaluating pulmonary perfusion, which may aid in raising the suspicion of PTTM in the appropriate clinical context.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pulmonary tumor thrombotic microangiopathy with pulmonary hypertension Cancer von Herbay A Illes A Waldherr R Otto HF 587592661990216374710.1002/1097-0142(19900801)66:3<587::aid-cncr 2820660330>3.0.co;2-j · doi ↗ · pubmed ↗
- 2Pulmonary tumor thrombotic microangiopathy: a systematic review Pulm Circ Godbole RH Saggar R Kamangar N 2045894019851000920193103274010.1177/2045894019851000 PMC 6540517 · doi ↗ · pubmed ↗
- 3Pulmonary tumor thrombotic microangiopathy: a clinical analysis of 30 autopsy cases Intern Med Uruga H Fujii T Kurosaki A 131713235220132377454010.2169/internalmedicine.52.9472 · doi ↗ · pubmed ↗
- 4Male breast cancer: a comparative analysis from the National Cancer Database World J Mens Health Elimimian EB Elson L Li H 5065153920213347485110.5534/wjmh.200164 PMC 8255393 · doi ↗ · pubmed ↗
- 5Three cases of pulmonary tumor thrombotic microangiopathy (PTTM): challenge in antemortem diagnosis using lung perfusion blood volume images by dual-energy computed tomography Eur J Radiol Open Kamada H Ota H Terui Y Sugimura K Fukui S Shimokawa H Takase K 100212720203310263410.1016/j.ejro.2020.01.001PMC 7569404 · doi ↗ · pubmed ↗
- 6Improvement of breast cancer-associated pulmonary tumor thrombotic microangiopathy with carboplatin and gemcitabine Cureus Tran H Kamangar N 015202310.7759/cureus.38600 PMC 1023965737284356 · doi ↗ · pubmed ↗
- 7Dramatic improvement of pulmonary tumor thrombotic microangiopathy in a breast cancer patient treated with bevacizumab World J Oncol Kimura A Yamada A Oshi M 5755791420233802240210.14740/wjon 1691 PMC 10681781 · doi ↗ · pubmed ↗
- 8A case report of pulmonary tumor thrombotic microangiopathy caused by lung adenocarcinoma: the importance of clinical diagnosis and monitoring disease progression Cureus Sakano Y Hamakawa Y Yamanaka R Funauchi A Marumo S Fukui M 017202510.7759/cureus.80489 PMC 1199343040225553 · doi ↗ · pubmed ↗