Febrile neutropenia caused by the rare organism Phytobacter: first Case Report from India
Anusha Mruthyunjaya Swamy, Prasenjit Das, Indrani Sarkar, Deepak Sundriyal, Amber Prasad, Saugata Hazra, Uttam Kumar Nath

TL;DR
This paper reports the first confirmed case of Phytobacter diazotrophicus bloodstream infection in India, occurring in a breast cancer patient undergoing chemotherapy.
Contribution
The study presents the first molecularly confirmed case of Phytobacter diazotrophicus in India using 16S rDNA sequencing.
Findings
Phytobacter diazotrophicus was identified in a breast cancer patient with febrile neutropenia.
Automated systems like VITEK-2 misidentified the organism as Pantoea, highlighting limitations in current diagnostic tools.
The patient recovered after treatment with blood transfusions, filgrastim, and antibiotics.
Abstract
Phytobacter diazotrophicus is an emerging opportunistic, Gram-negative bacterium, originally recognized as a nitrogen-fixing, plant-associated organism and increasingly implicated in nosocomial infections. We report the first documented case of bloodstream infection due to P. diazotrophicus in an elderly female breast cancer patient with chemotherapy-induced febrile neutropenia. A 62-year-old woman with HER2-positive, cT4bN2M0 breast cancer receiving neoadjuvant trastuzumab, carboplatin, and docetaxel presented with fever, headache, profound fatigue, pallor, and retinal hemorrhages. Laboratory evaluation revealed severe pancytopenia, with a platelet count of 5 × 10⁹/L, an absolute neutrophil count of 0.294 × 10⁹/L, a total leukocyte count of 1.05 × 10⁹/L, and a hemoglobin level of 3.7 g/dL. Blood cultures grew non-lactose-fermented Gram-negative bacilli, initially identified as Pantoea…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
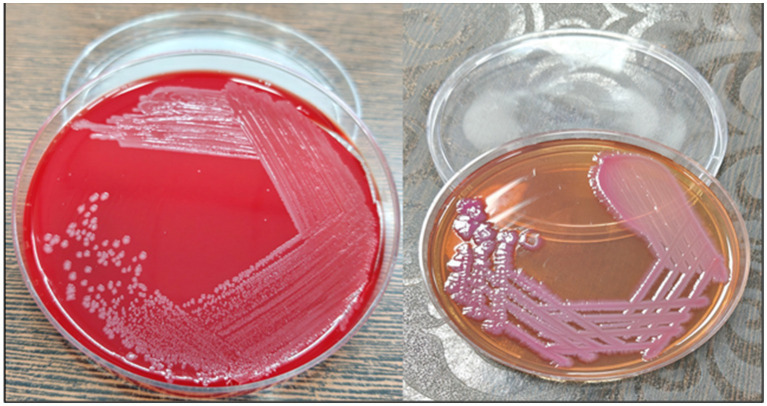 Figure 1
Figure 1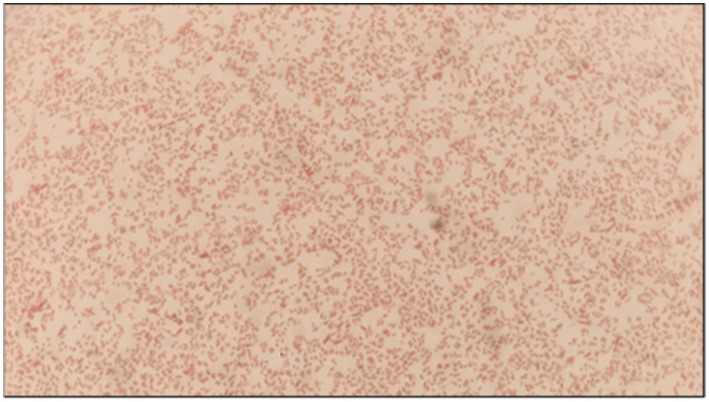 Figure 2
Figure 2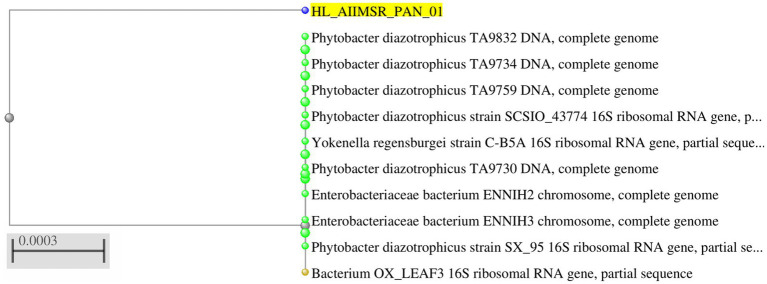 Figure 3
Figure 3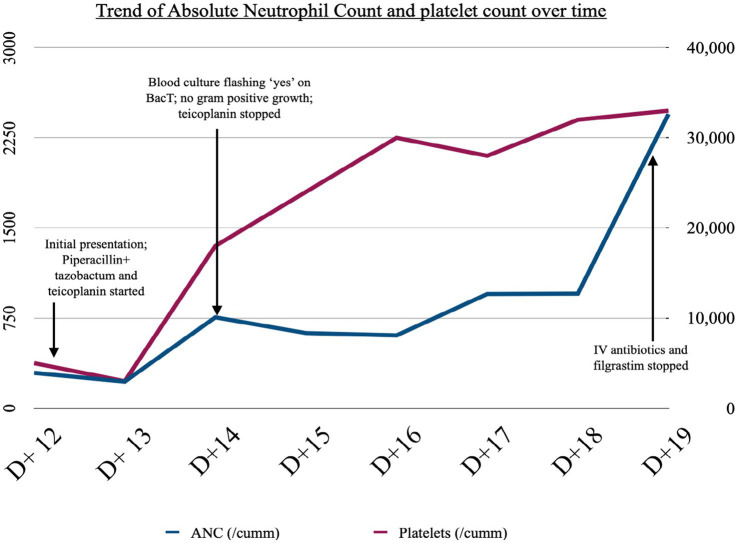 Figure 4
Figure 4| Strain name | ANI value |
|---|---|
| 98.88 | |
| 98.99 | |
| 98.97 | |
| 80.8 | |
| 91.99 | |
| 91.76 | |
| 70 |
| Name of antibiotics | MIC values | Interpretation |
|---|---|---|
| Amikacin | ≤1 | S |
| Gentamycin | ≤1 | S |
| Imipenem | ≤0.25 | S |
| Meropenem | ≤0.25 | S |
| Cefepime | ≤0.12 | S |
| Cefoperazone/Sulbactam | ≤8 | S |
| Piperacillin/tazobactam | ≤1 | S |
| Amoxicillin/Clavulanic acid | ≤0.2 | S |
| Trimethoprim/sulfamethoxazole | ≤20 | S |
| Ciprofloxacin | ≤0.06 | S |
| Colistin | ≤0.5I | I |
| Cefuroxime | ≤1 | S |
| Ertapenem | ≤0.12 | S |
| Ceftriaxone | ≤0.25 | S |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfections and bacterial resistance · Salmonella and Campylobacter epidemiology · Antibiotic Resistance in Bacteria
Background
Phytobacter diazotrophicus, though originally recognized as a plant growth-promoting Gram-negative bacterium, belongs to the Enterobacterales species and has recently been identified as an opportunistic pathogen associated with nosocomial infections (1). This species, as well as the associated genus of Phytobacter, was originally described by Zhang et al. in 2008, from wild rice in China, when it was noticed that P. diazotrophicus helps promote plant growth via nitrogen fixation (2). Its association with human disease was first described in 2018 in a retrospective analysis of preserved bacterial strains, which were traced back to multiple Brazilian sepsis outbreaks in 2010, 2013, and 2015. P. diazotrophicus has also been identified as the culprit behind several multidrug-resistant nosocomial infections (3). Globally, P. diazotrophicus has been isolated from cases of neonatal sepsis or as a contaminant in total parenteral nutrition (TPN) and in the elderly with a compromised immune system. Herein, we report a case of febrile neutropenia caused by P. diazotrophicus bloodstream infection in an elderly breast cancer patient following chemotherapy-induced neutropenia. Initial misidentification by the VITEK-2 system highlights the diagnostic challenges posed by this organism and underscores the importance of confirmatory molecular methods such as 16S rDNA sequencing. The emergence of such nosocomial pathogens represents a growing threat to antimicrobial resistance and poses a significant risk to immunocompromised populations, particularly patients with malignancies. To the best of our knowledge, this is the first reported case from India.
Case presentation
A 62-year-old woman, receiving neoadjuvant chemotherapy with trastuzumab (8 mg/kg loading dose followed by 6 mg/kg), carboplatin (AUC 6), and docetaxel (75 mg/m^2^) for HER2-positive carcinoma of the right breast, stage cT4bN2M0, presented to the hospital on day 12 of the third cycle of chemotherapy with fever, headache, and severe fatigue. On examination, she was conscious, febrile, and had tachycardia (pulse 110/min), severe pallor, and retinal hemorrhages on ophthalmoscopy. Her blood pressure was 130/70 mm Hg, and the systemic examination was normal. On admission, her hemoglobin was 3.7 g/dL, total leucocyte count (TLC) was 1.05 × 10^9^/L, absolute neutrophil count (ANC) was 0.294 × 10^9^/L, and platelet count was 5 × 10^9^/L. Thus, she was diagnosed to have chemotherapy-induced febrile neutropenia (common terminology criteria of adverse events (CTCAEs), grade III). Biochemical parameters, including serum lactate, were normal. Chest X-ray was normal. Blood and urine culture samples were sent, and broad-spectrum IV antibiotic therapy was immediately started with piperacillin-tazobactam (administered as an extended infusion over 3 h) and teicoplanin as per institutional protocol. She also received an injection of filgrastim 300 μg daily to aid neutrophil recovery and transfusion support with packed red blood cells and platelets.
The blood samples were sent in a BacT/ALERT bottle (BioMérieux) for microbiological investigation. It flashed “yes” following a day of incubation. Non-lactose fermenting colonies were cultivated by subculturing the bottle onto blood agar (BA) and Mac-Conkey agar (MAC), as shown in Figure 1. Phenotypic and antimicrobial susceptibility testing (AST) utilizing the automated VITEK-2 (Software:9.04) identification system (BioMérieux, France) initially recognized the isolate as Pantoea. For molecular-level identification, 16S rRNA gene sequencing was performed. Genomic DNA was first isolated, followed by PCR amplification using universal primers (forward primer: 5′-CCTACGGGNGGCWGCAG-3′and reverse primer: 5′-GACTACHVGGGTATCTAATCC-3′; Figure 2). The amplified products were sequenced using the Illumina MiSeq platform with a 2 × 300 bp paired-end V3–V4 sequencing kit. Sequence data were analyzed, and strain identification was carried out using the NCBI database. 16S rDNA sequence analysis indicated that the isolate was closely related to Phytobacter sp. (Figure 3). To achieve species-level identification, average nucleotide identity (ANI) analysis was conducted (4), and the resulting ANI values are presented in Table 1. Genome-based ANI analysis showed that the newly isolated clinical strain exhibited ANI values below the species threshold (95–96%) for all Phytobacter species except Phytobacter diazotrophicus, indicating a close relationship with P. diazotrophicus (5).
Blood agar and MacConkey agar.
Gram staining of Phytobacter sp.
Phylogenetic analysis of Phytobacter sp. based on the 16S rDNA gene.
The minimal inhibitory concentration (MIC) values and their justifications are summarized in Table 2. The results of the antibiotic susceptibility test (AST) were reported in accordance with the 2025 edition (M-100 S35 edition) MIC breakpoint recommendations published by the Clinical and Laboratory Standards Institute.
In view of the lack of Gram-positive growth and an overall improvement in the general condition of the patient, teicoplanin was stopped on day 3 of hospitalization. Piperacillin-tazobactam was continued along with transfusion support and filgrastim. Fortunately, the isolate in our patient was sensitive to most of the antibiotics, including cefepime, ertapenem (MIC ≤0.12), meropenem, and ceftriaxone (MIC ≤0.25), among the rest. There was a complete recovery from pancytopenia on day 7 of hospitalization. Antibiotics were stopped, and the patient was discharged on day 8. Patient subsequently followed up in our outpatient and continued to receive three additional cycles of neo-adjuvant chemotherapy with trastuzumab and single-agent reduced-dose taxane. She did not experience any grade III/IV toxicities and tolerated the rest of her treatment well. She also underwent a right modified radical mastectomy with a complete pathological response and is currently receiving adjuvant trastuzumab. A timeline depicting the clinical course is given in Figure 4.
Timeline of clinical events and trend of ANC and platelet count.
Discussion
The genus Phytobacter belongs to the family Enterobacteriaceae and is characterized by soil-borne diazotrophic species with an endophytic lifestyle, found in association with several plant species such as rice (Oryza rufipogon), oil palm, sugarcane, or switchgrass. It includes four species*: Phytobacter diazotrophicus*, Phytobacter ursingii, Phytobacter palmae, and Phytobacter massiliensis (6). In recent years, reports of multidrug-resistant P. diazotrophicus have been increasing. Most of these cases have been reported from neonatal intensive care units after the use of intravenous fluids or medical devices. Lin et al. isolated this pathogen from a neonatal sepsis patient (7). Another case series from Argentina included two elderly immunocompromised patients and one neonate, in whom the initial phenotypic identification using conventional biochemical tests was compatible with Pantoea spp. Species identification using matrix-assisted laser desorption ionization-time of flight mass spectrometry yielded P. ursingii in the neonate and Phytobacter sp. in the other three patients. On whole-genome sequencing, these were then identified to be P. diazotrophicus (8).
The VITEK 2 system identifies bacteria using biochemical reactions such as sugar fermentation and enzyme activity. Phytobacter and Pantoea share highly similar biochemical profiles, as both are Gram-negative, oxidase-negative, and ferment glucose, resulting in nearly identical metabolic signatures on standard VITEK cards (9). Since Phytobacter spp. are strong lactose-fermenting Gram-negative bacilli, they may resemble E. coli and Citrobacter on EMB Levine agar. Additionally, negative results for lysine decarboxylase, ornithine decarboxylase, and arginine dihydrolase can lead to the misidentification of these strains as Pantoea spp. or Pantoea agglomerans, as was seen in our patient. This has led to an underestimation of Phytobacter spp. in fatal outbreaks (8). Molecular methods (10) are essential for resolving ambiguous bacterial isolates. Sequencing of conserved genes such as 16S rRNA, or preferably gyrB, improves species-level discrimination within the Enterobacteriaceae. Although whole-genome sequencing provides the highest resolution—particularly in outbreak investigations through analyses such as ANI, dDDH, and core-genome phylogeny—its limited availability restricts its routine use. Consequently, accurate identification of Phytobacter spp. remains challenging in clinical microbiology laboratories.
Currently, several case reports and series have confirmed the occurrence of Phytobacter spp. As of July 2024, there were 41 draft or complete genomes of Phytobacter spp. listed at NCBI, of which no less than 25 were of direct human or clinical origin (6). In addition, several case reports describing multidrug-resistant strains of Phytobacter spp. have been published. Worryingly, these strains carried carbapenem resistance genes, bla_NDM − 1_ or bla_KPC_, on plasmids resistant to most β-lactam antibiotics (1, 11). Fortunately, our patient did not harbor any such strains and responded to piperacillin-tazobactam, which was given as an extended infusion over 3 h to achieve maximum therapeutic benefits in our neutropenic patient. Though Phytobacter spp. are commonly associated with the use of contaminated TPN formulations, our patient had not received any form of TPN and did not have a central venous catheter. The current episode in our patient appears to be directly related to the immunocompromised state due to chemotherapy-induced neutropenia.
For the treating physician, early identification of the causative pathogen and initiation of appropriate antibiotics is of utmost importance. This case report highlights the need to be aware of the occurrence of Phytobacter spp., which is not only notorious for causing nosocomial outbreaks but may also lead to delayed diagnosis and treatment due to diagnostic conundrums.
Conclusion
Phytobacter spp. are responsible for outbreaks of Gram-negative infections in the neonatal units and among those with a compromised immune system. However, their true global impact has been underestimated due to misidentification and inherent limitations in the testing procedures. This is the first case report from India with 16S rDNA sequencing-confirmed Phytobacter diazotrophicus bloodstream infection in a patient with febrile neutropenia. The emergence of multidrug-resistant strains can pose serious problems for the clinician, and a high index of suspicion is required for timely diagnosis and intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kubota H Nakayama T Ariyoshi T Uehara S Uchitani Y Tsuchida S . Emergence of Phytobacter diazotrophicus carrying an Inc A/C 2 plasmid harboring bla NDM-1 in Tokyo, Japan. m Sphere. (2023) 8:e 00147-23. doi: 10.1128/msphere.00147-23, 37449846 PMC 10449528 · doi ↗ · pubmed ↗
- 2Zhang GX Peng GX Wang ET Yan H Yuan QH Zhang W . Diverse endophytic nitrogen-fixing bacteria isolated from wild rice (Oryza rufipogon) and description of Phytobacter diazotrophicus gen. Nov., sp. nov. Arch Microbiol. (2008) 189:431–9. doi: 10.1007/s 00203-007-0333-7, 18060384 · doi ↗ · pubmed ↗
- 3Choice S Sherman A Holder K Harrington E. Gram-negative sepsis caused by a rare pathogen Phytobacter ursingii: a case report. BMJ Case Rep. (2024) 17:e 258384. doi: 10.1136/bcr-2023-258384, 38627051 PMC 11029423 · doi ↗ · pubmed ↗
- 4Yoon SH Ha SM Lim J Kwon S Chun J. A large-scale evaluation of algorithms to calculate average nucleotide identity. Antonie Van Leeuwenhoek. (2017) 110:1281–6. doi: 10.1007/s 10482-017-0844-4, 28204908 · doi ↗ · pubmed ↗
- 5Richter M Rosselló-Móra R. Shifting the genomic gold standard for the prokaryotic species definition. Proc Natl Acad Sci USA. (2009) 106:19126–31. doi: 10.1073/pnas.0906412106, 19855009 PMC 2776425 · doi ↗ · pubmed ↗
- 6Michel IR Kulek D Arend LNVS Pillonetto M Smits THM Rezzonico F. Development of two quantitative PCR assays for the detection of emerging opportunistic human pathogens belonging to the genus Phytobacter in routine diagnostics. Diagn Microbiol Infect Dis. (2024) 110:116556. doi: 10.1016/j.diagmicrobio.2024.116556, 39423472 · doi ↗ · pubmed ↗
- 7Lin J Wu J Gong L Li X Wang G. Sepsis caused by Phytobacter diazotrophicus complicated with galactosemia type 1 in China: a case report. BMC Infect Dis. (2024) 24:599. doi: 10.1186/s 12879-024-09458-y, 38898413 PMC 11186240 · doi ↗ · pubmed ↗
- 8Almuzara M Cittadini R Traglia G Haim MS De Belder D Alvarez C . Phytobacter spp: the emergence of a new genus of healthcare-associated Enterobacterales encoding carbapenemases in Argentina: a case series. Infect Prev Pract. (2024) 6:100379. doi: 10.1016/j.infpip.2024.100379, 39006243 PMC 11245914 · doi ↗ · pubmed ↗