Behavioural withdrawal during an acute stress test as a marker of psychobiological vulnerability in hereditary angioedema
Luca Ranucci, Francesca Perego, Aida Zulueta, Clara Gino, Azzurra Cesoni Marcelli, Lorenza Chiara Zingale, Laura Adelaide Dalla Vecchia, Beatrice De Maria, Alessandra Gorini

TL;DR
This study finds that patients with hereditary angioedema who withdraw during a stress test show worse disease control and unique stress responses.
Contribution
Early withdrawal during a stress test is identified as a novel marker of psychobiological vulnerability in hereditary angioedema patients.
Findings
Non-completers showed poorer disease control and worse quality of life compared to completers.
Non-completers reported higher stress, pain, and unpleasantness during the stress test.
Non-completers had distinct cardiovascular and inflammatory responses to stress.
Abstract
Hereditary angioedema due to C1-inhibitor deficiency (HAE-C1INH) features clinical heterogeneity and stress-triggered attacks. Behavioral tolerance to acute stress may reveal vulnerability profiles beyond standard clinical descriptors. This study aimed to characterize stress response patterns and compare groups based on behavioral tolerance. HAE-C1INH patients underwent the Socially Evaluated Cold Pressor Test (SECPT) and were stratified as Completers or Non-completers (early withdrawal). Stress appraisal, cardiovascular parameters (heart rate, HR; systolic/diastolic arterial pressure, SAP/DAP), and plasma cytokines (IL-1β, TNF-α, IL-6) were assessed. Disease control and quality of life were measured via Angioedema Control Test (AECT) and Angioedema Quality of life (AE-QoL) questionnaires. Twenty patients were enrolled (15 Completers and 5 Non-completers). Non-completers showed poorer…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
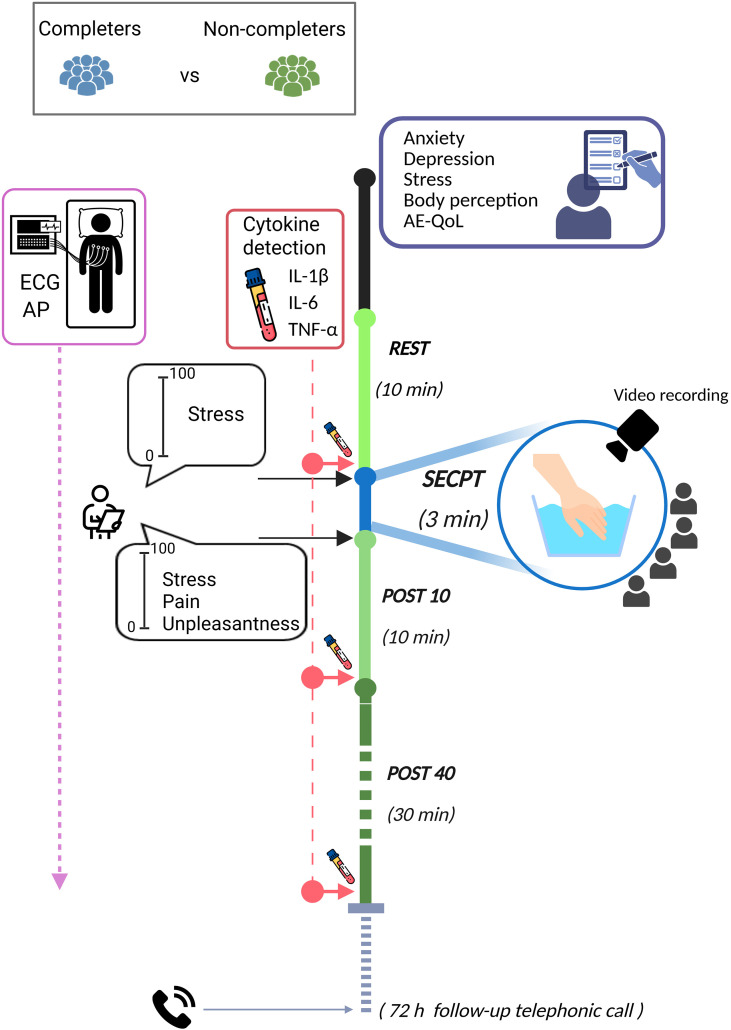 Figure 1
Figure 1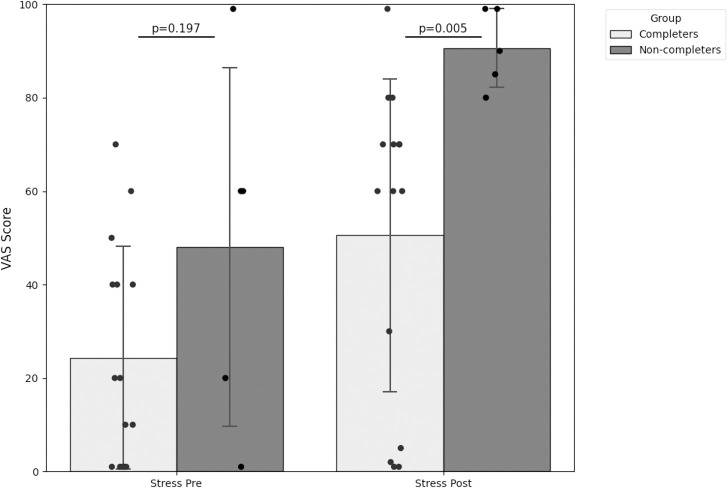 Figure 2
Figure 2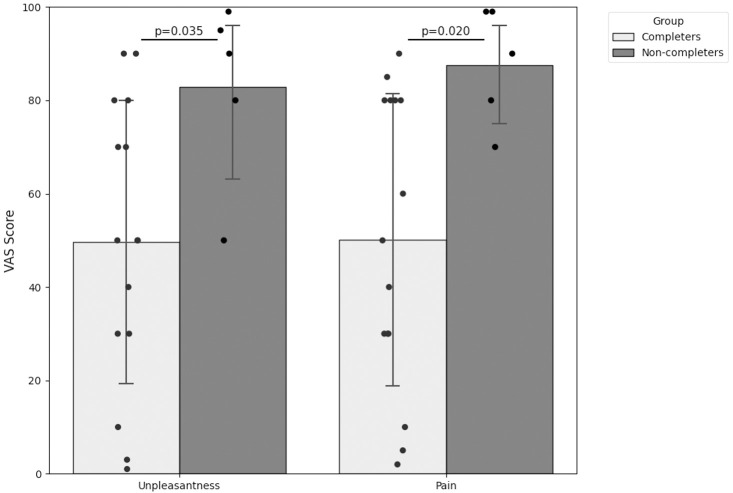 Figure 3
Figure 3| Variables | HAE Total (n=20) | Completers (n=15) | Non-completers (n=5) |
|---|---|---|---|
| Age, yrs | 44.7 ± 14.8 | 45.0 ± 14.6 | 44.0 ± 17.1 |
| Sex, n males/females | 9/11 | 8/7 | 1/4 |
| BMI, kg·m-2 | 25.0 ± 3.8 | 25.3 ± 3.3 | 23.9 ± 5.5 |
| Education, yrs | 14.0 ± 4.0 | 14.2 ± 3.8 | 13.4 ± 5.1 |
| Age at diagnosis, yrs | 18.6 ± 12.4 | 21.5 ± 12.7 | 10.0 ± 6.5 |
| Years from diagnosis, yrs | 26.3 ± 11.3 | 23.7 ± 9.9 | 34.2 ± 13.0 |
| Attack rate in the last 6 months, n | 2.9 ± 8.8 | 3.34 ± 10.2 | 1.6 ± 1.7 |
| No LTP, n (%) | 2.0 (10.0) | 2.0 (13.3) | 0 (0) |
| AE-QoL | 29.3 ± 12.2 | 25.9 ± 6.2 | 39.6 ± 20.1 |
| Functioning | 5.7 ± 3.0 | 4.7 ± 1.7* | 8.6 ± 4.3 |
| Fatigue/Mood | 9.6 ± 4.7 | 8.4 ± 3.4* | 13.2 ± 6.8 |
| Fears/Shame | 11.3 ± 4.6 | 10.5 ± 3.5 | 13.6 ± 7.1 |
| Food | 2.7 ± 1.7 | 2.3 ± 0.6 | 4.2 ± 3.0 |
| AECT | 13.5 ± 3.5 | 14.5 ± 2.2* | 10.6 ± 5.5 |
| HADS_A | 7.3 ± 4.5 | 7.2 ± 4.1 | 7.6 ± 6.1 |
| HADS_D | 3.1 ± 3.3 | 2.9 ± 3.4 | 3.8 ± 3.3 |
| FAS | 3.9 ± 0.7 | 4.0 ± 0.6 | 4.0 ± 0.8 |
| BAS | 37.7 ± 7.2 | 37.4 ± 7.4 | 38.6 ± 7.1 |
| MAIA | |||
| Not-Worrying | 2.5 ± 1.1 | 2.4 ± 1.1 | 3.1 ± 1.0 |
| Noticing | 3.3 ± 1.1 | 3.2 ± 1.0 | 3.6 ± 1.2 |
| Not-Distracting | 2.2 ± 0.8 | 2.3 ± 0.8 | 2.1 ± 0.6 |
| Attention Regulation | 2.7 ± 1.1 | 2.7 ± 1.0 | 2.6 ± 1.3 |
| Emotional Awareness | 3.5 ± 1.1 | 3.4 ± 1.2 | 3.6 ± 1.0 |
| Self-Regulation | 2.7 ± 1.4 | 2.9 ± 1.4 | 2.1 ± 1.3 |
| Body Listening | 2.5 ± 1.3 | 2.6 ± 1.3 | 2.1 ± 1.5 |
| Trusting | 3.3 ± 1.1 | 3.4 ± 1.0 | 2.7 ± 1.4 |
| PSS | 17.1 ± 7.2 | 16.9 ± 7.2 | 18 ± 8.2 |
| Grit-S | 3.8 ± 0.5 | 3.7 ± 0.5 | 4.2 ± 0.6 |
| PCS | 19.7 ± 12.6 | 20.5 ± 13.7 | 17.4 ± 9.5 |
| Helplessness | 7.0 ± 6.1 | 7.0 ± 6.6 | 7.0 ± 4.8 |
| Rumination | 9.1 ± 4.8 | 9.9 ± 5.1 | 7.0 ± 3.6 |
| Magnification | 3.5 ± 2.5 | 3.6 ± 2.8 | 3.4 ± 1.5 |
| Experimental phases | Completers (N = 15) | Non-completers (N = 5) | p |
|---|---|---|---|
| REST | |||
| HR, bpm | 59.3 ± 8.6 | 67.0 ± 13.6 | 0.152 |
| SAP, mmHg | 122.8 ± 16.4 | 119.2 ± 12.9 | 0.666 |
| DAP, mmHg | 77.8 ± 11.1 | 76.4 ± 6.6 | 0.792 |
| SECPT | |||
| HR, bpm | 66.5 ± 8.1 | 75.2 ± 12.7 | 0.090 |
| SAP, mmHg | 148.9 ± 18.3 | 128.3 ± 18.0 | 0.042* |
| DAP, mmHg | 92.4 ± 12.7 | 82.9 ± 9.5 | 0.144 |
| POST10 | |||
| HR, bpm | 58.5 ± 6.3 | 65.1 ± 10.9 | 0.110 |
| SAP, mmHg | 122.7 ± 17.4 | 119.7 ± 13.1 | 0.729 |
| DAP, mmHg | 78.1 ± 11.3 | 79.4 ± 6.4 | 0.810 |
| POST40 | |||
| HR, bpm | 58.6 ± 7.1 | 64.3 ± 9.4 | 0.161 |
| SAP, mmHg | 129.8 ± 15.2 | 113.2 ± 5.2 | 0.049* |
| DAP, mmHg | 82.4 ± 12.9 | 79.2 ± 8.7 | 0.618 |
| Experimental phases | Completers (N = 15) | Non-completers (N = 5) | p |
|---|---|---|---|
| REST | |||
| IL-1β, pg/ml | 19.5 ± 29.5 | 25.4 ± 26.2 | 0.431 |
| TNF-α, pg/ml | 4.3 ± 1.1 | 3.7 ± 2.0 | 0.394 |
| IL-6, pg/ml | 2.3 ± 1.1 | 3.4 ± 1.2 | 0.090 |
| POST10 | |||
| IL-1β, pg/ml | 19.4 ± 29.3 | 23.9 ± 21.9 | 0.379 |
| TNF-α, pg/ml | 4.1 ± 0.9 | 3.9 ± 2.4 | 0.643 |
| IL-6, pg/ml | 2.5 ± 1.1 | 3.5 ± 1.2 | 0.099 |
| POST40 | |||
| IL-1β, pg/ml | 19.6 ± 29.5 | 24.0 ± 23.9 | 0.379 |
| TNF-α, pg/ml | 3.8 ± 0.9 | 4.6 ± 2.0 | 0.926 |
| IL-6, pg/ml | 2.2 ± 0.7 | 3.5 ± 1.1 | 0.014* |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoagulation, Bradykinin, Polyphosphates, and Angioedema · Complement system in diseases · Hemophilia Treatment and Research
Introduction
Hereditary angioedema due to C1-Inhibitor deficiency (HAE-C1INH) is a rare, genetic condition characterized by unpredictable and potentially life-threatening swellings (1, 2). Such unpredictability leads to a substantial burden, manifesting as anxiety, depression, anticipatory worry, and reduced Quality of Life (QoL) (3–5), which often persists during attack-free periods (6). Although current therapeutic options, such as On-Demand (ODT) and Long-Term Prophylaxis (LTP) therapies, can effectively control clinical manifestations, attacks may still occur, and the disease burden frequently remains elevated (7).
This persistent burden is compounded by the remarkable and largely unexplained clinical heterogeneity of HAE-C1INH, with phenotypes ranging from asymptomatic to symptomatic with a high variability of the number of attacks that can be frequent and highly debilitating (8). The determinants of individual susceptibility to specific attack triggers are unclear. Consequently, there is a critical need to move beyond standard clinical descriptors and identify novel biomarkers capable of capturing this heterogeneity and stratifying patient vulnerability with the aim of implementing further preventive strategies.
Notably, patients frequently report psychobiological stress as an attack trigger (9), and increased attack rates have been documented during major population-level stressors (10–12). These observations point to a vicious cycle in which stress precipitates attacks, and these attacks in turn amplify stress and illness-related anxiety (9). Given this complexity, research should focus on a multidimensional framework, where biological, psychological, and behavioral domains are interpreted as co-occurrent phenomena that represent the patients’ experience (9).
To address this gap, through a multidimensional lens, we employed the Socially Evaluated Cold Pressor Test (SECPT), a validated acute stress paradigm that robustly activates both the sympathetic–adrenomedullary (SAM) and hypothalamic–pituitary–adrenal (HPA) systems (13). Crucially, beyond physiological indices, the SECPT provides a behavioral marker of stress endurance, defined as task completion versus early withdrawal. In healthy subjects, where approximately 15% of participants fail the task (14), early withdrawal has been linked to greater pain sensitivity, higher perceived stress, and blunted cardiovascular reactivity (CVR) (14, 15). Previous evidence also showed that, during SECPT, HAE-C1INH patients exhibit heightened perceived stress and elevated baseline inflammation compared to healthy controls despite having comparable CVR (16).
We reasoned that early withdrawal in HAE-C1INH patients, provides a behavioral index of stress intolerance that may capture inter-individual differences not detectable through standard clinical descriptors. Therefore, the aim of this study was to characterize and compare the stress reactivity patterns in HAE-C1INH patients associated with SECPT completion to identify potential markers of vulnerability.
Materials and methods
Participants
We considered the cohort of HAE-C1INH patients that were studied for the FRoSEn study (16). In this pilot study HAE-C1INH patients were consecutively enrolled during ambulatory visits from June 2023 to April 2024 at the IRCCS Istituti Clinici Scientifici Maugeri of Milan. Inclusion criteria were: (i) a documented diagnosis of HAE-C1INH and (ii) an age between 18 and 65 years. Exclusion criteria included: (i) presence of any other chronic disease requiring chronic treatment (e.g., hypertension, diabetes, autoimmune diseases), (ii) an active acute illness, (iii) SARS-CoV-2 infection in the previous 3 months (17), (iv) HAE attack occurring in the week preceding the experimental session and (v) HAE attack in the following 72 hours (a posteriori exclusion).
A formal sample size calculation was not applicable due to the lack of data for comparison in HAE-C1INH patients. All analyses were exploratory due to the pilot sample size.
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the IRCCS Istituti Clinici Scientifici Maugeri (approval number 2774 CE; date of approval 31 May 2023) and was registered on ClinicalTrials.gov (NCT06414252). All participants provided written informed consent before their inclusion in the study.
Study procedure
An overview of the experimental protocol is provided in Figure 1, while a detailed description of the protocol is presented elsewhere (16). Briefly, experimental sessions were conducted in a quiet room with a comfortable temperature, between 9 a.m. and 12 p.m. to control for diurnal variations in biochemical parameters, and participants were instructed to avoid consuming caffeine prior to the experimental protocol. All participants underwent a medical visit to verify the inclusion and exclusion criteria and to collect demographic and clinical data. A venous catheter was subsequently inserted to allow for repeated blood sampling, avoiding multiple punctures. Participants were also instrumented for continuous monitoring of heart rate (HR) and non- invasive arterial blood pressure (AP).
Schematic representation of the experimental protocol. The figure was created in Biorender.com.
In summary, the protocol consisted of the following phases (Figure 1):
REST (Baseline): a set of questionnaires assessing sociodemographic and psychological variables was administered, then a 10-minute resting period in a supine position in a quiet room started. A baseline blood sample was collected at the end of this period.
SECPT (Stress Task): participants, remaining in a supine position, were instructed to immerse their hand in cold water maintained at 4°C for a maximum of 3 minutes. They were informed that they could remove their hand at any time if the perception became intolerable. To induce social evaluation, participants were videotaped and instructed to look into the camera for the entire duration of the immersion, while an experimenter monitored them and took notes. Immediately before the hand immersion, participants rated how stressed they were on a Visual Analogue Scale (VAS) (0 = “not at all” to 100 = “very much”).
Subjective Ratings: immediately after removing their hand from the water, participants rated how unpleasant, stressful, and painful the experience had been on a VAS (0 = “not at all” to 100 = “very much”).
POST10 (Recovery 1): a 10-minute recovery period immediately started after the SECPT. A second blood sample was collected at the end of this phase.
POST40 (Recovery 2): an additional 30-minute recovery period (40 minutes post SECPT) ended with a third blood sample collection. Continuous physiological signals were monitored throughout all phases.
A follow-up phone call was made 72 hours after the session to verify the potential occurrence of HAE-C1INH attacks.
Following the experimental session, patients were categorized into two subgroups based on their SECPT performance. Patients who completed the 3-minute protocol were classified as “Completers”, while those who withdrew before the 3-minute cut-off were classified as “Non-completers”.
Psychological scales
A battery of self-report questionnaires was administered to assess a range of psychological outcomes at baseline. The Hospital Anxiety and Depression Scale (HADS) (18) was administered to measure anxiety and depressive symptoms. Stress perception during the last month was measured with the Perceived Stress Scale (PSS) (19). Pain-related cognitions were investigated using the Pain Catastrophizing Scale (PCS) (20). Then, given the somatic nature of HAE-C1INH, participants’ relationship with their body was also explored through several scales. The Functionality Appreciation Scale (FAS) (21) and the Body Appreciation Scale (BAS) (22) were used to assess appreciation for the body’s capabilities and overall acceptance of one’s body, respectively. The Multidimensional Assessment of Interoceptive Awareness (MAIA) (23) was administered to evaluate multiple dimensions of interoception, such as the ability to notice, listen to, and trust bodily sensations. To assess personality traits relevant to perseverance, the Short Grit Scale (Grit-S) (24) was included; this 8-item questionnaire measures “grit,” defined as the tendency to apply passion and sustained effort toward long-term goals. Lastly, angioedema specific outcomes were quantified using the Angioedema Quality of Life (AE-QoL) (25) questionnaire, a 17-item scale, to measure disease-specific impairment across four domains (Functioning, Fatigue/Mood, Fears/Shame, and Food). It is scored as a percentage on a scale of 0 to 100, with lower scores indicating less impairment and better quality of life. Disease control was assessed by the 4-item Angioedema Control Test (AECT) (26), which provides a score from 0 to 16, with higher scores indicating better disease control.
Physiological measures
As described elsewhere (16), continuous physiological signals were recorded, including a continuous electrocardiogram (ECG, LAB3 device, Marazza, Monza, Italy) and non-invasive AP via a photoplethysmography device (Finometer, Finapres Medical System) positioned on the middle finger of the right hand. ECG was sampled at 1000 Hz, while AP at 250 Hz. From these signals, beat-to-beat time series of RR intervals, systolic arterial pressure (SAP), and diastolic arterial pressure (DAP) were derived for subsequent analysis. RR was defined as the temporal distance between two consecutive R peaks detected on the ECG, while SAP and DAP as the maximum and minimum values of the AP signal inside each RR, respectively.
Biochemical parameters analysis
Six milliliters of blood from each participant were drawn into EDTA-coated tubes at three time points: REST, POST10, and POST40. To obtain plasma, the blood samples were centrifuged for 15 minutes at 2,000 × g within 30 minutes of collection. The plasma fraction was then divided into 500 µL aliquots, quickly frozen and kept at −80 °C until further experiments. Plasma levels of Interleukin-1 beta (IL-1β), Interleukin-6 (IL-6) and Tumor Necrosis Factor-alpha (TNF-α) were measured using high-sensitive enzyme-linked immunosorbent assays (ELISA). The following commercial kits were used: IL-1β (E-HSEL-H0001, ElabScience, USA), IL-6 (950.035.096, Diaclone, France), and TNF-α (EIA-4641, DRG, Germany). Each assay included blanks, calibration standards, quality controls, and plasma samples, all tested in duplicate using 96-well microplates, in accordance with the manufacturers’ protocols. Optical density was measured at 450 nm using an automated ELISA reader. Cytokine concentrations were expressed in picograms per milliliter (pg/mL), and the mean value of the duplicates was used for statistical analysis.
Data processing and statistical analysis
Statistical analyses were performed using Sigmaplot (v.14.0, Systat Software, San Jose, CA, USA). The Shapiro-Wilk test was applied to check the normality of the distribution. Unpaired Student t test, or Mann-Whitney rank sum test in case of not-normal distribution, was applied to compare baseline demographic, clinical, psychological characteristics, subjective ratings of stress, pain, and unpleasantness, psychophysiological profile, cardiovascular and inflammatory response between the Completer and Non-completer groups. Fisher’s exact test was used for categorical variables. A p<0.05 was considered as significant.
Results
Demographic and clinical characteristics
The study cohort comprised 20 adult patients with HAE-C1INH (mean age: 44.7 ± 14.8 years; 11 females). Of these, 15 (75%) managed to complete the SECPT while 5 (25%) withdrew their hand before the 3-minute cut-off. No attacks were reported within the next 72 hours. Demographic data and key clinical variables relevant to the disease (e.g., Attack rate, LTP) and its impact on daily life (e.g., AE-QoL, AECT) are summarized in Table 1. Most patients (18 out of 20) were on LTP regimen at the time of the study. Comparisons between Completers and Non-completers revealed significant differences in AECT and AE-QoL. Specifically, Completers reported better disease control and lower impairment in the “Functioning” and “Fatigue/Mood” domains of the AE-QoL. Conversely, no significant differences were observed regarding other baseline variables.
Psychological response
Figure 2 shows the comparison of stress appraisal prior and immediately after the SECPT phase, while Figure 3 illustrates the comparison of perceived pain and unpleasantness immediately after SECPT. Group comparison revealed distinct profiles. Non-completers exhibited higher baseline stress levels compared to Completers (47.8 ± 38.6 vs. 24.0 ± 24.1; p=0.197) and reported a significantly higher, near-maximal surge in stress immediately after the stress task (91.0 ± 8.9 vs. 50.5 ± 33.7; p=0.05).
Group comparison of stress ratings (VAS stress) prior and immediately after the SECPT. Stress Pre, VAS stress before SECPT; Stress Post, VAS stress after SECPT.
Group comparison of unpleasantness and pain ratings (VAS unpleasantness and VAS pain) immediately after SECPT. Unpleasantness, perceived unpleasantness during SECPT; Pain, perceived pain during SECPT.
Furthermore, the subjective appraisal of the stimulus differed substantially: Non-completers experienced the task as significantly more painful (87.8 ± 12.8 vs. 50.1 ± 31.3; p=0.02) and unpleasant (83.0 ± 19.9 vs. 49.5 ± 30.5; p=0.03).
Cardiovascular response
Cardiovascular reactivity data are presented in Table 2. Non-completers registered significantly lower SAP during SECPT compared to Completers. This difference was also present in the POST40 phase, where Non-completers maintained a lower SAP.
When comparing group trajectories across experimental phases, Non-completers exhibited an attenuated AP response to the stressor compared to Completers (Appendix A). Specifically, the increase in SAP from REST to SECPT was significantly smaller among Non-completers (9.1 ± 7.9 vs 26.2 ± 12.0 mmHg; p<0.01). Similarly, the DAP response was significantly attenuated in Non-completers (6.4 ± 4.5 vs 14.5 ± 5.2 mmHg; p<0.01). From SECPT to POST10 phase, Non-completers demonstrated a significantly smaller DAP reduction compared to the recovery observed in Completers (-3.4 ± 4.0 vs -14.2 ± 7.9 mmHg; p<0.01).
Inflammatory response
Table 3 reports data on inflammatory cytokines. Between groups comparison showed trending differences regarding IL-6 levels at REST, and at POST10 in which Non-completers showed higher concentrations than Completers. This trend reached statistical significance during the POST40 phase, in which the Non-completers exhibited significantly higher levels of IL-6 (2.2 ± 0.7 vs 3.5 ± 1.1 pg/ml; p=0.014). Regarding IL-1β and TNF-α, the analysis did not yield statistically significant differences between the two subgroups at any specific time point.
However, with respect to TNF-α trajectories across the experimental phases, the two groups showed opposite dynamics (Appendix B). Between REST and POST40, Completers showed a decreasing trend while Non-completers exhibited an increasing one (-0.46 ± 0.86 vs. 0.93 ± 0.97 pg/ml; p=0.008) and this difference was also present between POST10 and POST40 phases (-0.26 ± 0.76 vs 0.72 ± 0.75 pg/ml; p=0.024).
Discussion
This pilot study investigated whether behavioral withdrawal during a standardized acute stress task (SECPT non-completion) captures clinically relevant heterogeneity in patients affected by HAE-C1INH. Clinical heterogeneity and persistent burden are widely recognized in HAE-C1INH, including impaired quality of life and disease control despite available therapies (5, 7, 25). In parallel, patients frequently report stress as a trigger, and increased attack rates have been described during major population-level stressors (10, 12). Within this context, we observed that early SECPT withdrawal was associated with higher disease burden, greater subjective distress during the stressor, an attenuated arterial blood pressure response, and distinct inflammatory trajectories during the experimental phases. Together, these converging signals suggest that SECPT performance may offer a pragmatic behavioral index of stress tolerance that complements standard clinical descriptors.
Behavioral withdrawal as a marker of vulnerability
The SECPT is a well-validated laboratory paradigm that robustly activates stress-related systems while providing an objective behavioral endpoint (task completion vs early withdrawal) (13, 14). In our sample, non-completion was not explained solely by greater unpleasantness; rather, Non-completers combined high subjective distress (stress, pain, unpleasantness) with poorer disease control and QoL impairment. Although causality cannot be inferred, the alignment between behavioral avoidance and clinically meaningful burden supports the interpretation of early withdrawal as a candidate marker of vulnerability within HAE-C1INH.
AP response patterns during acute stress
Non-completers showed an attenuated increase in SAP/DAP during the stress phase and a less pronounced recovery pattern relative to Completers. Rather than using the broader label of “blunted reactivity”, our data specifically indicate an attenuated AP response in this experimental context. Reduced cardiovascular reactivity has been linked to altered stress regulation and adverse behavioral/health correlates in other settings (27–29). In HAE-C1INH, where unpredictability and anticipatory worry are common (7, 25), limited pressor mobilization and/or inefficient recovery may contribute to perceived uncontrollability and avoidance behavior. This finding adds granularity to our previous observation that HAE-C1INH exhibit heightened perceived stress despite displaying a cardiovascular reactivity comparable to that of healthy subjects (16).
Another possible interpretation of our results is that stress-induced release of bradykinin, a potent endothelial vasodilator, may functionally oppose the sympathetic vasoconstriction triggered by the SECPT (30). In this scenario, the elevated HR in Non-completers may represent a compensatory but ineffective chronotropic effort, attempting to counteract the bradykinin-mediated vasodilation (31, 32). Notably, this pattern of heightened sympathetic drive failing to stabilize vascular tone mirrors the autonomic dysregulation often hypothesized to occur in the prodromal phase of attacks (33), reinforcing the concept that this hemodynamic inefficiency may mirror the physiological instability that predisposes patients to attacks.
Given the small subgroup size, these physiological findings remain exploratory and should be replicated with more complex autonomic measures in stable conditions (i.e. REST and recovery phases) by HR and AP variability analysis and baroreflex sensitivity assessment.
Inflammatory trajectories
Beyond subjective appraisal and pressor indices, Non-completers displayed distinct inflammatory dynamics, including higher IL-6 during late experimental phase and divergent TNF-α trajectories relative to Completers. Similar findings were found in a recent study on pro-inflammatory cytokine concentrations in the overall HAE-C1INH population. Participants showed significantly higher cytokine concentrations compared to healthy controls (34). Stress-related immune changes are shaped by bidirectional neuro-immune pathways and regulatory loops (35, 36). In HAE-C1INH, inflammatory signaling is also embedded within disease-specific mechanisms such as the contact system and bradykinin-related pathways (30, 32). Accordingly, our cytokine findings should be interpreted as preliminary evidence of differential immune response associated with behavioral stress intolerance, rather than as definitive mechanistic proof.
Integrative interpretation and implications
Taken together, our findings converge on the hypothesis that SECPT non-completion identifies a subgroup with (i) greater subjective threat/pain appraisal, (ii) less efficient AP mobilization, and (iii) a more sustained inflammatory response profile. Predictive processing accounts, including the Embodied Predictive Interoceptive Coding (EPIC) framework (37), offer one plausible interpretative lens: illness burden may act as a negative prior that biases the organism toward conservative, energy-preserving responses when incoming signals are appraised as costly or threatening. In parallel, models emphasizing sickness behavior and effort-based decision-making highlight how inflammatory and interoceptive signals can shift motivation toward withdrawal (38), consistent with energy-conserving strategies described in other physiological domains (39). The observed attenuated AP response and the concomitant inflammatory patterns match the “Type 4” profile of allostatic load described by McEwen (36), defined as an “Inadequate Response”, where the failure of one system to mount a sufficient response leads to the compensatory hyperactivity of another. On one hand, the inadequate cardiovascular engagement may lead to a failure of the vagal anti-inflammatory reflex (35). On the other hand, in line with the EPIC model, inaccurate predictions can lead to a pro-inflammatory state, in our context the specific increase in TNF-α suggests the activation of a stress-reactive kinin-mast cell axis (30). Specifically, we hypothesize that in these vulnerable individuals, acute stress may trigger a low-grade release of bradykinin. This mediator could simultaneously account for our findings by blunting the pressor response through vasodilation and promoting a pro-inflammatory state via mast cell activation, resulting in the observed TNF-α surge. This finding is particularly significant as it may represent the mechanistic bridge between acute stress and attack vulnerability. While TNF-α is a known marker of systemic inflammation, its sustained rise in Non-completers suggests a failure to buffer the stress-induced activation of the contact system. Biologically, the released TNF-α can further sensitize the endothelium and promote mast cell degranulation (40), potentially lowering the threshold for bradykinin-mediated vascular leakage (41). Consequently, a feed-forward loop is established: it is biologically plausible that bradykinin signaling not only blunts the pressor response but also promotes downstream cytokine release from sensitized mast cells or endothelium (30). This may create a self-sustaining vicious cycle where the inability to mount a hemodynamic response translates directly into unbuffered inflammatory signaling.
These frameworks should be presented as hypotheses that generate testable predictions. Clinically, if replicated, behavioral withdrawal during standardized stress exposure could support stratification of patients who may benefit from targeted stress regulation and coping interventions integrated with routine care.
Limitations
This study has several limitations. First, it is a pilot investigation with a small sample, the Non-completer group was particularly small, and most of them were on LTP. This limits statistical power, stability of subgroup estimates and the interpretation of the contribution of prophylaxis on the results. Second, multiple outcomes were examined; therefore, results should be interpreted as exploratory, with emphasis on patterns and effect sizes rather than definitive inference. Third, we did not include neuroendocrine measures (e.g., cortisol). This decision was deliberately taken to avoid the confounding effects of its significant circadian variability. Given that cortisol levels fluctuate heavily depending on the time of day, including this marker would have introduced substantial noise, potentially masking the specific stress-reactivity patterns we aimed to isolate. Fourth, potential confounders of lifestyle factors that may influence physiological and cytokine responses were not investigated. Finally, the cross-sectional design does not allow evaluation of whether this phenotype predicts clinically meaningful endpoints (e.g., future attacks, healthcare use, or longitudinal QoL trajectories).
Strengths
This study also has several strengths. First, it adopts a multimodal approach, combining behavioral performance, subjective appraisal, cardiovascular indices, and inflammatory markers within the same experimental session, enabling convergent interpretation across domains. Second, it leverages a standardized and well-validated acute stress paradigm that provides an objective behavioral endpoint (withdrawal vs completion), which may be particularly informative in conditions characterized by different phenotypes and clinical heterogeneity such as in HAE-C1INH (13, 14). Third, the protocol includes repeated biological sampling, allowing the assessment of stress-related dynamics across the acute phase. Finally, by linking laboratory patterns to clinically meaningful patient-reported outcomes (AECT and AE-QoL), the study enhances translational relevance and supports the feasibility of using behavioral stress tolerance as a candidate marker in future longitudinal works.
Conclusion
In this pilot study of HAE-C1INH, early withdrawal from the SECPT identified a subgroup with higher disease burden, greater subjective distress, attenuated pressor reactivity, and distinct inflammatory responses. While the exploratory nature of this research and the small sample size warrant caution in generalizing these results, the strength of our findings lies in the convergence across psychological, cardiovascular, and immunological domains. These preliminary findings support behavioral stress tolerance as a candidate psychobiological marker that may contribute to stratifying vulnerability in HAE-C1INH and guiding future longitudinal and mechanistic research. Preventive measures in addition to pharmacological prophylaxis may represent a more sustainable and synergistic approach that can contribute to a better management of patients affected by HAE-C1INH.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wu MA Perego F Zanichelli A Cicardi M . Angioedema phenotypes: disease expression and classification. Clin Rev Allergy Immunol. (2016) 51:162–9. doi: 10.1007/s 12016-016-8541-z, PMID: 27113957 · doi ↗ · pubmed ↗
- 2Maurer M Magerl M Betschel S Aberer W Ansotegui IJ Aygören-Pürsün E . The international WAO/EAACI guideline for the management of hereditary angioedema—The 2021 revision and update. Allergy. (2022) 77:1961–90. doi: 10.1111/all.15214, PMID: 35006617 · doi ↗ · pubmed ↗
- 3Longhurst H Bygum A . The humanistic, societal, and pharmaco-economic burden of angioedema. Clin Rev Allergy Immunol. (2016) 51:230–9. doi: 10.1007/s 12016-016-8575-2, PMID: 27388236 · doi ↗ · pubmed ↗
- 4Chong-Neto HJ . A narrative review of recent literature of the quality of life in hereditary angioedema patients. World Allergy Organ J. (2023) 16:100758. doi: 10.1016/j.waojou.2023.100758, PMID: 36994443 PMC 10040818 · doi ↗ · pubmed ↗
- 5Mendivil J Murphy R de la Cruz M Janssen E Boysen HB Jain G . Clinical characteristics and burden of illness in patients with hereditary angioedema: findings from a multinational patient survey. Orphanet J Rare Dis. (2021) 16:94. doi: 10.1186/s 13023-021-01717-4, PMID: 33602292 PMC 7893968 · doi ↗ · pubmed ↗
- 6Bork K Anderson JT Caballero T Craig T Johnston DT Li HH . Assessment and management of disease burden and quality of life in patients with hereditary angioedema: a consensus report. Allergy Asthma Clin Immunol. (2021) 17:40. doi: 10.1186/s 13223-021-00537-2, PMID: 33875020 PMC 8056543 · doi ↗ · pubmed ↗
- 7Banerji A . The burden of illness in patients with hereditary angioedema. Ann Allergy Asthma Immunol. (2013) 111:329–36. doi: 10.1016/j.anai.2013.08.019, PMID: 24125136 · doi ↗ · pubmed ↗
- 8Loli-Ausejo D López-Lera A Drouet C Lluncor M Phillips-Anglés E Pedrosa M . In search of an association between genotype and phenotype in hereditary angioedema due to C 1-INH deficiency. Clin Rev Allergy Immunol. (2021) 61:1–14. doi: 10.1007/s 12016-021-08834-9, PMID: 33469833 · doi ↗ · pubmed ↗