Endometriosis-Associated Intestinal Tumor: A Case Report and Literature Review with Comprehensive Proteomic Data
Naoyuki Toyota, Yuki Yoshimatsu, Chihiro Kamozawa, Ryo Nakanishi, Shin Fujita, Makoto Abe, Ryo Konno, Yusuke Kawashima, Tadashi Kondo

TL;DR
This case report describes a rare intestinal tumor linked to endometriosis and highlights the challenges in diagnosis and treatment.
Contribution
The paper provides comprehensive proteomic data from an endometriosis-associated intestinal tumor, offering insights for future research.
Findings
The patient was diagnosed with endometriosis-associated endometrioid adenocarcinoma after inconclusive initial tests.
Proteomic profiling of the tumor may aid in understanding its biology and guide future translational research.
The patient remained disease-free for 3.5 years following surgery and chemotherapy.
Abstract
Endometriosis-associated intestinal tumors (EAITs) are rare malignancies that arise from ectopic endometrial tissue, and their clinical and molecular characteristics remain poorly defined. We report a 53-year-old woman who presented with rectal bleeding. Imaging revealed a rectal mass invading the uterus. An initial endoscopic biopsy was inconclusive; however, a subsequent CT-guided biopsy confirmed adenocarcinoma. Immunohistochemical analysis suggested a gynecological origin. The patient underwent posterior total pelvic exenteration with bilateral lymphadenectomy. Histopathological evaluation confirmed endometriosis-associated endometrioid adenocarcinoma with ovarian metastasis. Postoperative chemotherapy was administered, and the patient has remained disease-free for 3.5 years. This case highlights the diagnostic challenges and clinical complexity of EAITs. Tumor proteomic profiling…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
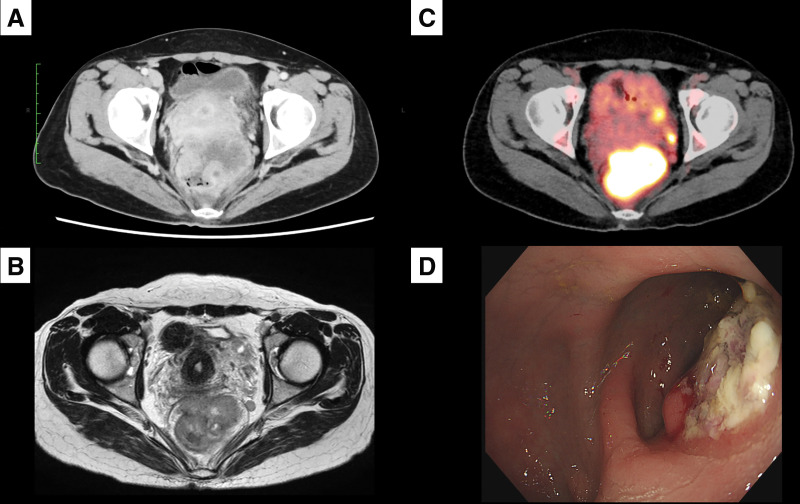 Fig. 1
Fig. 1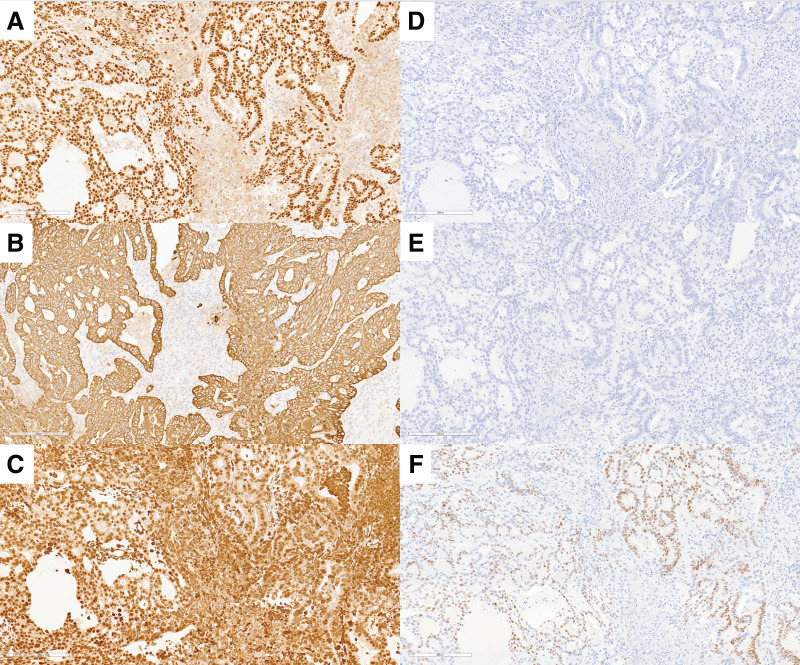 Fig. 2
Fig. 2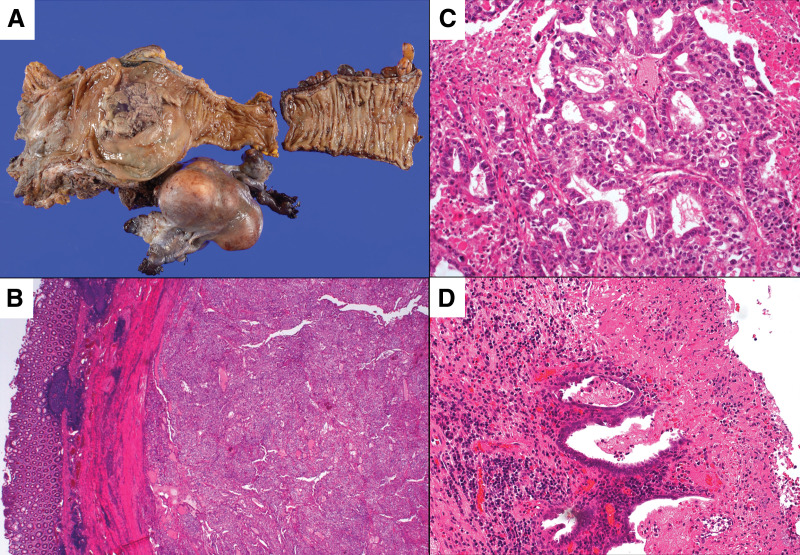 Fig. 3
Fig. 3| Case no. | Author | Year | Age | Site | Prodromal symptoms | Diagnosis | Treatment | Lymph nodes metastasis | Postoperative therapy | Outcome | Follow-up (month) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Nylander | 1938 | 36 | Rectum | Abdominal pain | Spindle cell sarcoma | Surgery | (Not available) | None | AWOD | (Not available) |
| 2 | Marx | 1949 | 48 | Sigmoid | Lower abdominal pain | Squamous cell carcinoma | Surgery | (Not available) | None | (Not available) | (Not available) |
| 3 | Ferraro | 1956 | 44 | Ileum | Abdominal pain, LLQ mass, Melena | Endometrial sarcoma | Sigmoidectomy with R2 resection | (Not available) | Radiation | DOD | 4 |
| 4 | Weinrod | 1956 | 59 | Sigmoid | Abdominal discomfort, Melena | Adenocanthoma | Small bowel resection | Negative | None | (Not available) | (Not available) |
| 5 | Scully | 1966 | 64 | Sigmoid | Frequent bowel movements, Melena | Endometrial stromal sarcoma | Sigmoidectomy | (Not available) | None | DOC | 216 |
| 6 | Reintoft | 1974 | 36 | Rectum | Not given | Endometrioid carcinoma | Hysterectomy, left salpingo-oophorectomy, and rectal resection | Positive | Radiation | DOD | 4 |
| 7 | Weisz-Carrington | 1977 | 77 | Cecum | Melena, Distension | Carcinosarcoma | Ileocolectomy | Positive | None | DOD | 1 |
| 8 | Lott | 1978 | 52 | Rectum | Hematochezia | Endometrioid carcinoma | Anterior resection | (Not available) | None | AWOD | (Not available) |
| 9 | Grimes | 1980 | 44 | Cecum and terminal ileum | Abdominal pain | Adenosquamous carcinoma | Right colectomy | Positive (9/20) | None | DOD | 10 |
| 10 | Amano | 1981 | 44 | Sigmoid | Abdominal distress, Melena | Endometrioid carcinoma | Sigmoidectomy | Negative | None | AWOD | (Not available) |
| 11 | Lankerani | 1982 | 49 | Sigmoid | Abdominal discomfort | Mixed germ cell tumor | Hysterectomy, Bilateral salpingo-oophorectomy, and rectal resection | (Not available) | None | DOD | 12 |
| 12 | Chumas | 1986 | 67 | Rectosigmoid | Frequent bowel movements, Melena | Carcinosarcoma | Hartmann procedure with distal right ureter resection | Positive (1/20) | Chemotherapy | DOD | 24 |
| 13 | Baiocchi | 1990 | 38 | Terminal ileum | Abdominal pain | Endometrial stromal sarcoma | Partial ileal resection; transverse and ascending colectomy with R2 resection | (Not available) | Chemotherapy | AWOD | (Not available) |
| 14 | Hitti | 1990 | 39 | Ascending colon | Lower abdominal pain | Clear cell carcinoma | Sigmoid colectomy with total hysterectomy and bilateral salpingo-oophorectomy | Negative | Chemotherapy, Radiation | AWOD | 9 |
| 15 | Yasui | 1992 | 44 | Sigmoid | Ileus | Endometrioid carcinoma | Low anterior resection | (Not available) | None | (Not available) | (Not available) |
| 16 | Duun | 1993 | 62 | Rectum | Pelvic mass | Endometrioid carcinoma | Anterior resection of the rectosigmoid colon | (Not available) | Radiation | DOD | 12 |
| 17 | Jiang | 1993 | 42 | Sigmoid | Abdominal mass | Endometrioid carcinoma | Surgery | (Not available) | Chemotherapy | AWOD | 6 |
| 18 | Slavin | 2000 | 62 | Rectum | Perirectal mass | Endometrioid carcinoma | Segmental rectal resection with peritoneal mass excision, sigmoid colectomy, and TAH-BSO | Negative | None | AWOD | 24 |
| 19 | Slavin | 2000 | 38 | Rectum | Abdominal pain, Hematochezia | Endometrioid carcinoma | Sigmoidectomy, TAH + BSO, and omentectomy | Negative | None | AWOD | 24 |
| 20 | Slavin | 2000 | 54 | Sigmoid | Vaginal bleeding | Endometrioid carcinoma | Extirpation of pelvic mass with partial vaginectomy and additional sigmoid colectomy | Negative | None | AWOD | 12 |
| 21 | Slavin | 2000 | 49 | Sigmoid | Abdominal pain in LLQ | Adenofibroma | Sigmoidectomy | Negative | None | AWOD | 36 |
| 22 | Slavin | 2000 | 47 | Sigmoid | Small bowel obstruction | Adenosarcoma | Segmental distal ileal resection with right anterior pelvic sidewall resection | Negative | Chemotherapy (adriamycin, ifosfamide, etoposide) | AWOD | 72 |
| 23 | Slavin | 2000 | 50 | Sigmoid | Melena, pelvic mass | Carcinosarcoma | Sigmoidectomy with right pelvic sidewall resection | Positive | Chemotherapy (cisplatin, megestrol acetate) | DOD | 5 |
| 24 | Yantiss | 2000 | 52 | Sigmoid | Obstruction | Endometrioid carcinoma | Segmental colectomy | Negative | None | AWOD | 1 |
| 25 | Yantiss | 2000 | 66 | Rectum (rectovaginal septum) | Pelvic mass, pelvic pain | Endometrioid carcinoma | Segmental colectomy with R2 resection | Negative | Radiation | AWOD | 38 |
| 26 | Yantiss | 2000 | 74 | Sigmoid | Obstruction | Endometrioid carcinoma | Segmental colectomy | Positive | None | DOD | 12 |
| 27 | Yantiss | 2000 | 47 | Rectum (rectovaginal septum) | Pelvic pain, pelvic mass | Endometrioid carcinoma | Segmental colectomy | Negative | Radiation | AWOD | 9 |
| 28 | Yantiss | 2000 | 67 | Rectum (rectovaginal septum) | Vaginal bleeding | Endometrioid carcinoma | Segmental colectomy | Negative | None | AWOD | 156 |
| 29 | Yantiss | 2000 | 48 | Rectum (rectovaginal septum) | Acute abdomen, Fecal peritonitis | Endometrioid carcinoma | Segmental colectomy | (Not available) | (Not available) | (Not available) | (Not available) |
| 30 | Yantiss | 2000 | 60 | Colon | (Not available) | Endometrioid carcinoma | Segmental colectomy | Positive | Chemotherapy | AWD | 24 |
| 31 | Yantiss | 2000 | 62 | Sigmoid | (Not available) | Endometrioid carcinoma | Segmental colectomy | (Not available) | (Not available) | (Not available) | (Not available) |
| 32 | Yantiss | 2000 | 65 | Small bowel | Chronic abdominal pain, Hypermenorrhea | Endometrioid adenofibroma, adenocarcinoma | Segmental small bowel resection | Negative | None | AWOD | 3 |
| 33 | Yantiss | 2000 | 36 | Sigmoid | Abdominal pain | Endometrioid carcinoma | Segmental colectomy | Negative | None | AWOD | 36 |
| 34 | Yantiss | 2000 | 50 | Colon | (Not available) | Mullerian adenosarcoma | Segmental colectomy | (Not available) | (Not available) | AWOD | 24 |
| 35 | Yantiss | 2000 | 83 | Small bowel | Abdominal mass, Obstruction | Mullerian adenosarcoma | Segmental small bowel resection | (Not available) | (Not available) | (Not available) | (Not available) |
| 36 | Yantiss | 2000 | 43 | Small bowel | (Not available) | Mullerian adenosarcoma | Segmental colectomy with R2 resection | (Not available) | (Not available) | (Not available) | (Not available) |
| 37 | Yantiss | 2000 | 63 | Rectum | (Not available) | Endometrioid stromal sarcoma | Segmental colectomy | Negative | Radiotherapy | AWD | 36 |
| 38 | Yantiss | 2000 | 57 | Sigmoid | Obstruction, BRBPR | Mild atypical hyperplasia | Segmental colectomy | Negative | None | AWOD | 1 |
| 39 | Yantiss | 2000 | 63 | Rectum | Progressive change bowel habits | Moderate atypical hyperplasia, endometriosis | Segmental colectomy | (Not available) | (Not available) | AWOD | 60 |
| 40 | Yantiss | 2000 | 59 | Sigmoid | Obstruction | Adenocarcinoma in situ | Segmental colectomy | Negative | None | AWOD | 192 |
| 41 | Magtibay | 2001 | 76 | Rectum | Diarrhea, rectal bleeding | Endometrioid adenocarcinoma | Low anterior resection with colonic J-pouch anal anastomosis and diverting right transverse colostomy | Negative | Radiation | AWOD | 21 |
| 42 | Jones | 2002 | 52 | Sigmoid | Rectal bleeding | Endometrioid adenocarcinoma | Anterior resection of the rectosigmoid colon | Negative | None | AWOD | 9 |
| 43 | Chen | 2002 | 80 | Rectum | Constipation, Hematochezia | Endometrioid adenocarcinoma | Rectosigmoid segmental resection | Positive (5/10) | (Not available) | (Not available) | (Not available) |
| 44 | Petersen | 2002 | 61 | Sigmoid | Diarrhea | Endometrioid adenocarcinoma | Anterior resection with formation of a loop ileostomy | Negative | (Not available) | (Not available) | (Not available) |
| 45 | Petersen | 2002 | 47 | Rectum | Large bowel obstruction | Endometrioid adenocarcinoma | Sigmoidectomy, TAH + BSO | Positive (3/18) | (Not available) | (Not available) | (Not available) |
| 46 | Petersen | 2002 | 57 | Rectum | Lower abdominal pain and mass lesion | Endometrioid adenocarcinoma | Anterior resection | Negative | (Not available) | (Not available) | (Not available) |
| 47 | Debus | 2001 | 50 | Rectum | Abdominal mass | Endometrioid adenocarcinoma | Rectosigmoid colectomy with diverting ileostomy, omentectomy, and appendectomy | Negative | Chemotherapy (TC, 6 cycles) | AWOD | (Not available) |
| 48 | Hoang | 2005 | 60 | Rectum | Hematochezia | Endometrioid adenocarcinoma | En bloc resection of the upper rectum and distal ureter | Negative | (Not available) | (Not available) | (Not available) |
| 49 | Kawate | 2005 | 62 | Sigmoid | Abdominal tumor | Endometrioid adenocarcinoma | Sigmoidectomy with lymph node dissection | Positive (5/10) | Chemotherapy (Cyclophosphamide, Pirarubicin, Hydrochloride, Carboplatin) | AWOD | 28 |
| 50 | Efethymou | 2009 | 59 | Rectum | Constipation, Weight loss | Endometrioid adenocarcinoma | Anterior resection with diverting loop ileostomy | Negative | (Not available) | AWOD | (Not available) |
| 51 | Kobayashi | 2010 | 45 | Rectum | Periodic hematochezia with lower abdominal pain during her menstrual period | Endometrioid adenocarcinoma | Anterior resection | Positive (6/8) | Chemotherapy (TC) | AWOD | (Not available) |
| 52 | Palla | 2017 | 75 | Sigmoid | Abdominal pain, Enterorrhagia | Endometrioid adenocarcinoma | Sigmoidectomy | (Not available) | None | (Not available) | (Not available) |
| 53 | Hemedez | 2018 | 58 | Rectum | Recto-vaginal pain, Severe constipation | Endometrioid adenocarcinoma | Low Anterior resection | Negative | Chemotherapy | AWOD | (Not available) |
| 54 | Li | 2018 | 55 | Rectum | Abdominal pain, Enterorrhagia | Endometrioid adenocarcinoma | Anterior resection, hysterectomy and bilateral salpingo-oophorectomy | Positive (8/30) | Chemotherapy (TC, 8 cycles) | AWD | 23 |
| 55 | Yang | 2019 | 57 | Rectum | Left lower abdominal pain | Endometrioid adenocarcinoma | Radical hysterectomy; bilateral adnexectomy; pelvic peritonectomy; pelvic lymphadenectomy; omentectomy; partial rectal resection with diverting ileostomy; appendectomy | (Not available) | Chemotherapy | AWOD | 12 |
| 56 | Current case | 2025 | 53 | Rectum | Lower abdominal pain | Endometrioid adenocarcinoma | Low anterior resection, total hysterectomy, bilateral salpingo-oophorectomy, vaginal cuff resection, and bilateral lateral pelvic lymph node dissection | Negative | Chemotherapy (TC, 6 cycles) | AWOD | 36 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometriosis Research and Treatment · Echinoderm biology and ecology · Coagulation, Bradykinin, Polyphosphates, and Angioedema
Abbreviations
EAIT endometriosis-associated intestinal tumors ^18^F-FDG-PET fluorine-18 fluorodeoxyglucose-PET
INTRODUCTION
Endometriosis is a benign, non-neoplastic condition characterized by the ectopic proliferation of endometrial tissue. Approximately 80% of cases involve the ovaries, whereas about 12% affect the intestines, with the rectum and sigmoid colon being the most frequently involved sites.^1)^ Malignant transformation of intestinal endometriosis is exceedingly rare. The first case of endometriosis-associated adenocarcinoma was reported by Sampson in 1925.^2)^ Since then, only a few comprehensive reports have been published, including a notable series of 23 cases by Slavin et al. in 2000.^3)^
Despite these efforts, the clinicopathological and molecular features of EAITs remain poorly understood. In this report, we describe a rare case of rectal EAIT and provide an integrated clinicopathological analysis in the context of previously published cases, including 15 reported in the past literature. Additionally, we conducted a comprehensive proteomic analysis of the tumor tissue using mass spectrometry (Supplementary Table 1). The resulting global protein expression profile was deposited in the publicly accessible Japan ProteOme STandard (jPOST) repository, providing a reference resource that may support future comparative analyses as more cases are accumulated.
CASE PRESENTATION
A 53-year-old woman presented with rectal bleeding and was referred to a secondary hospital for further evaluation.
History of present illness
She reported persistent dull pain in the lower abdomen but denied other gastrointestinal symptoms such as weight loss, vomiting, nausea, or diarrhea.
Past medical and family history
The patient had no notable past medical history except for a prior anal fistula, and no relevant family history.
Physical examination
The patient appeared well, with a body mass index of 21.8 kg/m^2^. Abdominal examination revealed no tenderness or palpable masses, and there was no enlargement of the spleen, liver, or lymph nodes. However, gynecological examination revealed a palpable mass in the pouch of Douglas with mild tenderness. Digital rectal examination identified a solid mass on the anterior wall of the rectum.
Laboratory findings
Routine hematological and biochemical tests were within normal limits, including liver and renal function tests. Tumor markers, including carcinoembryonic antigen and carbohydrate antigen 19-9, were within normal ranges. However, CA125 was elevated at 148.0 U/mL (normal range: 0–35 U/mL), suggesting a potential gynecologic malignancy.
Imaging studies
Initial colonoscopy at the referring hospital revealed an 8-cm segmental stenosis in the rectum (Rb–Rs), suspected to result from extramural compression. Endoscopic biopsy was inconclusive, prompting referral for further investigation.
Contrast-enhanced CT demonstrated a poorly defined 7-cm mass on the anterior rectal wall, with suspected extensive invasion into the uterus and prominent pelvic and lateral lymphadenopathy (Fig. 1A). Pelvic MRI showed circumferential wall thickening of the rectum with heterogeneous enhancement, raising suspicion for invasion into the uterovaginal junction (Fig. 1B). PET with ^18^F-FDG-PET revealed significant tracer uptake in the rectal lesion and bilateral lateral pelvic lymph nodes (Fig. 1C).
Preoperative multimodal imaging studies. (A) Contrast-enhanced abdominal CT demonstrating a highly invasive, bulky tumor occupying more than half of the pelvic cavity and involving both the rectum and the uterus. (B) Pelvic MRI showing circumferential rectal wall thickening with heterogeneous enhancement, suggestive of invasion into the uterovaginal junction. (C) Fluorine-18 fluorodeoxyglucose-PET revealing marked tracer uptake in the rectal tumor as well as in the bilateral lateral pelvic lymph nodes. (D) Repeat colonoscopy identifying the lower tumor margin approximately 6 cm from the anal verge. Extramural compression was again observed, accompanied by partial mucosal ulceration with a villous tumor-like appearance.
A second colonoscopy identified the tumor’s lower edge approximately 6 cm from the anal verge. Extramural compression was again observed, with partial mucosal ulceration resembling a villous tumor (Fig. 1D). However, biopsy specimens demonstrated only necrotic tissue and no evidence of malignancy.
To establish a definitive diagnosis, a CT-guided needle biopsy was performed. Histopathological analysis confirmed adenocarcinoma. Immunohistochemical stains showed the tumor cells to be positive for PAX8, CK7, estrogen receptor (ER), and vimentin, and negative for CK20 and CDX2, findings consistent with a gynecologic origin (Fig. 2A–2F).
Immunohistochemical (IHC) staining of tumor cells for six markers (original magnification ×200). (A) PAX8 (positive). (B) CK7 (positive). (C) Vimentin (positive). (D) CK20 (negative). (E) CDX2 (negative). (F) Estrogen receptor (ER) (positive).
Final diagnosis
Based on the clinicopathological findings, the diagnosis of EAIT was established.
Treatment
Given the aggressive clinical presentation and precedent from previous case reports, the patient underwent posterior pelvic exenteration. The procedure included low anterior resection, total hysterectomy, bilateral salpingo-oophorectomy, vaginal cuff resection, and bilateral lateral pelvic lymph node dissection, in collaboration with the gynecology team. No macroscopic intraperitoneal metastasis was identified intraoperatively. Owing to bilateral tumor extension, resection of both pelvic plexus nerves was performed.
Pathological findings
Gross examination revealed a 70 × 67 × 48 mm tumor extending from the rectosigmoid junction to the upper rectum, located predominantly on the anterior rectal wall with mucosal ulceration (Fig. 3A), and invading the uterine cervix. Microscopically, the lesion displayed glandular and solid architecture, composed of columnar cells with eosinophilic and clear cytoplasm, mimicking endometrial-type glands (Fig. 3B and 3C). Foci of adjacent endometriosis were identified (Fig. 3D). Based on these findings, the tumor was diagnosed as endometriosis-associated endometrioid adenocarcinoma. Surgical margins were negative. No lymph node metastasis was identified, but ovarian metastasis was confirmed.
Histopathological features of the resected specimen. (A) Macroscopic examination of the resected specimen showing a tumor located predominantly on the anterior rectal wall with mucosal ulceration. (B) Low-power magnification (original magnification ×40) showing tumor invasion into the rectal muscularis propria. (C) High-power magnification (original magnification ×200) demonstrating neoplastic glands composed of columnar cells with clear to eosinophilic cytoplasm, consistent with endometrioid carcinoma. (D) Foci of endometriosis identified on the rectal serosa adjacent to the tumor (original magnification ×200).
Postoperative course and follow-up
The postoperative course was uneventful, except for the development of a neurogenic bladder. Because of the ovarian metastasis, six cycles of adjuvant chemotherapy with paclitaxel and carboplatin (TC regimen) were administered. The patient has remained disease-free for 3.5 years.
Proteomic analysis
Tumor tissue was obtained from the Tochigi Cancer Biobank. Samples were collected intraoperatively under the supervision of a certified pathologist and preserved in vapor-phase liquid nitrogen. Informed consent was obtained from the patient. Ethical approval was granted by the Tochigi Cancer Center Ethics Committee (Approval No. 21-A037). Proteomic profiling was performed using mass spectrometry, as described in the Supplementary Methods. A total of 9294 proteins were identified (Supplementary Table 1), and the data have been deposited in the jPOST database (Accession Nos.: JPST004032 and PXD067723). The dataset is publicly available through the ProteomeXchange Consortium via the jPOST partner repository.
DISCUSSION
Endometriosis is characterized by the presence of endometrial glands and stroma outside the uterine cavity. Although its etiology remains unclear, Sampson’s theory of retrograde menstruation is the most widely accepted hypothesis. According to this theory, endometrial fragments reflux through the fallopian tubes into the peritoneal cavity during menstruation, where they adhere to and infiltrate the pelvic organs. Endometriosis affects approximately 10%–15% of women of reproductive age. Based on anatomical distribution, it is classified into common sites (e.g., ovaries, uterosacral ligaments, pouch of Douglas, peritoneum), less common sites (e.g., intestines, ureters, bladder), and rare sites (e.g., lungs, pleura, soft tissues).^4)^
Among these, intestinal endometriosis represents the most frequent form of extrapelvic disease, occurring in 12%–37% of all endometriosis cases. The rectum and sigmoid colon are the most commonly involved intestinal sites (84%), followed by the colon (7%), cecum (5%), and appendix (3%).^5)^ While intestinal endometriosis is often managed conservatively, its malignant transformation—referred to as EAITs—is of major clinical concern. Approximately 0.7%–1.0% of all endometriosis cases undergo malignant transformation, with 78.7% of these occurring in the ovaries and the remaining 21.3% in extragonadal sites.^6)^ In a Japanese nationwide survey by Mandai et al., 7 out of 11 cases of malignant transformation in rare-site endometriosis involved the intestines.^4)^
EAITs are exceedingly rare, and no consensus exists regarding their optimal management. This study provides two main contributions. First, it represents the first attempt to investigate EAITs using proteomic analysis. Second, given that fewer than ten cases of EAIT have been reported in the Japanese population, presenting a Japanese EAIT case with proteomic analysis results is particularly noteworthy. In this study, proteomic analysis was prioritized over genomic or transcriptomic approaches to address the specific clinical and pathological questions raised by this rare case. While genomic and transcriptomic profiling are powerful tools for identifying recurrent molecular alterations across cohorts, their interpretability is inherently limited in single-case studies, particularly when the goal is to understand functional tumor biology. Proteomics captures the integrated downstream consequences of genetic, epigenetic, and transcriptional regulation, thereby providing a more direct representation of the tumor’s active molecular state. This feature makes proteomic profiling especially suitable for exploratory analyses aimed at linking molecular signatures with histopathological features and clinical behavior in rare or atypical presentations.
To date, we have identified 56 previously reported cases published in the English literature, which are summarized in Table 1.^3,7–37)^ The median age of onset ranged from 36 to 83 years, with a peak incidence in the 60s, followed by the 50s and 40s. About half of the patients presented with abdominal pain or gastrointestinal symptoms such as rectal bleeding, melaena, or hematochezia. Acute presentations, including bowel obstruction or peritonitis, were rare. Consistent with previous studies, the rectum was the most frequent site of EAITs.
Histologically, endometrioid adenocarcinoma was the predominant tumor type (n = 34), followed by carcinosarcoma (n = 3), Müllerian adenosarcoma (n = 3), endometrial stromal sarcoma (n = 2), spindle cell carcinoma (n = 1), squamous cell carcinoma (n = 1), adenoacanthoma (n = 1), adenosquamous carcinoma (n = 1), and clear cell carcinoma (n = 1). This histological diversity underscores the heterogeneous nature of EAITs.
Preoperative diagnosis remains challenging, largely owing to the submucosal or extrinsic growth pattern of these tumors. Conventional diagnostic modalities such as ultrasound, CT, and MRI have shown limited accuracy, with correct preoperative diagnosis reported in only 9%–22% of cases.^38,39)^ More recently, endoscopic ultrasound with fine-needle aspiration has emerged as a valuable tool for tissue diagnosis and should be considered early in the diagnostic work-up.^40,41)^
Immunohistochemistry also plays a critical role in differentiating EAITs from primary colorectal adenocarcinomas. While CK20 is commonly expressed in intestinal-type and Merkel cell carcinomas, CK7 positivity (in the absence of CK20) is typically seen in gynecological, breast, and lung adenocarcinomas.^42)^ Additionally, PAX8 and CDX2 staining provide further diagnostic guidance. PAX8 is a marker for Müllerian, renal, and thyroid tumors,^43)^ whereas CDX2 is a highly sensitive and specific marker for intestinal differentiation, particularly colorectal origin. Furthermore, vimentin and ER positivity supports an endometrioid phenotype. Therefore, the use of a panel of immunomarkers is recommended to distinguish EAITs from primary colorectal malignancies.
Surgical resection remains the mainstay of treatment. Most reported cases have undergone en bloc resection with concurrent or non-concurrent hysterectomy and oophorectomy, although no formal guidelines recommend this approach. Given the common dissemination pattern of endometriosis through the uterus and adnexa, combined gynecological resection is generally favored.^42)^
According to Table 1, 51 of 55 cases achieved R0/1 resection, and 94% of patients who survived for more than 1 year had undergone R0/1 surgery. In addition, lymph node metastasis appears to have a substantial impact on prognosis. Lymph node metastasis was identified in 12 of 38 cases for which lymph node status was available; recurrence occurred in 8 of these 12 patients in the lymph node-positive group, compared with 1 of 26 patients in the lymph node-negative group, indicating a markedly higher recurrence rate.
This finding is consistent with the report by Tanaka et al., who analyzed Japanese case reports and demonstrated that the 5-year overall survival rate was 90.9% in the lymph node-negative group and 41.7% in the lymph node-positive group.^44)^ Taken together, these findings suggest that achieving complete resection is a key determinant of favorable outcomes, whereas lymph node metastasis is associated with poor prognosis and a high risk of recurrence.
On this basis, we elected to perform posterior pelvic exenteration with bilateral pelvic lymph node dissection, including lateral pelvic nodes, with the aim of maximizing oncological clearance. Although this approach entails substantial surgical invasiveness, the patient was deemed fit for radical surgery. Furthermore, preoperative imaging demonstrated significant enlargement of the lateral pelvic lymph nodes, supporting the need for aggressive surgical clearance. In this context, the potential oncological benefit of complete tumor eradication was considered to outweigh the risks associated with the extensive procedure.
The role of adjuvant chemotherapy or radiation therapy in EAIT remains unclear. Among patients with lymph node-positive disease listed in Table 1, 7 of 12 received additional treatment, such as chemotherapy or radiation therapy. In most reported cases, chemotherapy regimens based on ovarian cancer protocols—most commonly paclitaxel and carboplatin—have been used empirically. Kawate et al. reported a favorable outcome using a regimen comprising cyclophosphamide, pirarubicin, and carboplatin in a patient with lymph node-positive disease;^31)^ however, the evidence remains anecdotal. Similarly, the role of radiation therapy is poorly defined, with no established evidence regarding optimal dose or irradiation field. Therefore, further investigation is warranted to establish optimal adjuvant treatment strategies and standardized protocols through collaborative efforts.
Finally, we conducted proteomic analysis of the tumor using mass spectrometry. We acknowledge the inherent limitations of single-case studies, including the inability to draw generalized conclusions or establish causality. Accordingly, the present analysis should be regarded as exploratory in nature. Rather than serving as definitive evidence, the proteomic dataset generated in this study is intended to function as a reference molecular profile for this rare disease context. By providing a detailed protein-level characterization, this work offers a foundation for future comparative analyses, enabling subsequent studies to assess reproducibility, identify shared molecular features, and refine biological hypotheses as additional cases become available. Integrating such datasets across multiple cases may enable the identification of diagnostic biomarkers or novel therapeutic targets in EAIT.
CONCLUSIONS
We presented an extremely rare case of an EAIT. Although EAITs generally have a poor prognosis, our case suggests that aggressive surgical resection, including lymphadenectomy, followed by adjuvant chemotherapy may improve clinical outcomes. Further research is required to determine the optimal surgical approach, define the role of adjuvant therapies, and identify reliable prognostic indicators. Moreover, the proteomic data generated from this case, which are publicly available through a proteomic repository, provide a valuable resource for future comparative studies when integrated with additional cases.
SUPPLEMENTARY MATERIALS
Supplementary Table 1. Results of comprehensive proteomic analysis of the tumor tissue using mass spectrometry.
Supplementary MethodsDetailed methods are described in the Supplementary Appendix.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Orbuch IK, Reich H, Orbuch M, et al. Laparoscopic treatment of recurrent small bowel obstruction secondary to ileal endometriosis. J Minim Invasive Gynecol 2007; 14: 113–5.17218241 10.1016/j.jmig.2006.07.009 · doi ↗ · pubmed ↗
- 2Sampson JA. Endometrial carcinoma of the ovary, arising in endometrial tissue in that organ. Arch Surg 1925; 10: 1–72.
- 3Slavin RE, Krum R, Van Dinh T. Endometriosis-associated intestinal tumors: a clinical and pathological study of 6 cases with a review of the literature. Hum Pathol 2000; 31: 456–63.10821493 10.1053/hp.2000.6712 · doi ↗ · pubmed ↗
- 4Mandai M, Osuga Y, Hirata T, et al. Cancers associated with extraovarian endometriosis at less common/rare sites: a nationwide survey in Japan. J Obstet Gynaecol Res 2020; 46: 917–23.32212420 10.1111/jog.14244 · doi ↗ · pubmed ↗
- 5Longo LD. Classic pages in obstetrics and gynecology. Aberrant portions of the Müllerian duct found in an ovary [William Wood Russell, Johns Hopkins Hospital bulletin, vol.10, pp.8-10, 1899]. Am J Obstet Gynecol 1979;134:225–6.377966 · pubmed ↗
- 6Heaps JM, Nieberg RK, Berek JS. Malignant neoplasms arising in endometriosis. Obstet Gynecol 1990; 75: 1023–8.2188180 · pubmed ↗
- 7Nylander PEA. Zur Frage des Rektumsarkoms. Zentralbl Chir 1938; 65: 74–8.
- 8Marx H. Ein Beitrag zur Frage der bosartige Entartung der Endometriose. Chirurgie 1949; 20: 441–3.