Assessing the Acceptance of and Compliance With Centchroman Usage, a Non-hormonal Contraceptive Pill, Among Postpartum Women: A Cross-Sectional Study at a Tertiary Care Centre in North India
Pooja Yadav, K Aparna Sharma, Pragati Singh, Nidhi Bhatt, Vidushi Kulshrestha, Priya Karna, Neena Malhotra, Ashish Bhatt

TL;DR
This study evaluates how well postpartum women in India accept and use Centchroman, a non-hormonal contraceptive pill, finding it to be well-accepted with low failure rates.
Contribution
The study provides new empirical evidence on the real-world usage, satisfaction, and effectiveness of Centchroman among postpartum women in India.
Findings
Centchroman had a 58% continuation rate for 12 months or more among postpartum users.
The Pearl Index was 0.42 per hundred woman-years, indicating a low failure rate.
93% of users reported satisfaction with Centchroman, and 88% would recommend it.
Abstract
Introduction: Centchroman is a non-hormonal oral contraceptive available in India through the national family planning program under the brand name "Chhaya." As the first non-hormonal oral contraceptive, it inhibits implantation without affecting ovulation or the hormonal axis, making it particularly safe for breastfeeding women. Despite these advantages, its uptake remains limited. This study aimed to assess the acceptance, satisfaction, compliance, continuation, side effects, and failure rate among centchroman users who adopted it as a contraceptive method. Materials and methods: A cross-sectional descriptive study was conducted through telephonic follow-up of postpartum centchroman users over two years (January 2023 to December 2024) at the Family Planning Clinic, Department of Obstetrics and Gynaecology, AIIMS, New Delhi. A total of 241 women were included. Data on demographics,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
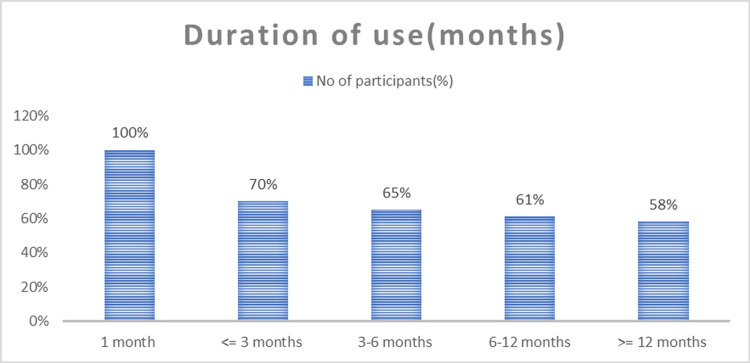 Figure 1
Figure 1| Age distribution | Centchroman users | Percentage (%) |
| Under 19 years | 2 | 0.8 |
| 19-24 years | 39 | 16.2 |
| 24-29 years | 94 | 39 |
| 29-34 years | 86 | 35.7 |
| 35-39 years | 17 | 7.1 |
| >39 years | 3 | 1.2 |
| Parity | Centchroman users | Percentage (%) |
| Nulliparous | 21 | 8.7 |
| 1 | 162 | 67.3 |
| 2 | 50 | 20.7 |
| 3 or >3 | 8 | 3.3 |
| Time of start | Centchroman users | Percentage (%) |
| Postpartum | 174 | 72.2 |
| Interval | 62 | 25.7 |
| Post-abortal | 5 | 2.1 |
| Side effect | Frequency | Percentage |
| No side effects | 198 | 82.2% |
| Delayed menses | 26 | 10.7% |
| Headache | 5 | 2.1% |
| Nausea | 5 | 2.1% |
| Abdominal discomfort | 4 | 1.65% |
| Breast tenderness | 2 | 0.83% |
| Weight gain | 1 | 0.42% |
| Reasons for discontinuation | Frequency | Percentage |
| Distance from the facility and difficulty obtaining the drug | 29 | 12% |
| Adoption of alternative contraception (permanent method, LARC, DMPA) | 29 | 12% |
| Temporarily staying away from their partner because of local cultural beliefs | 18 | 7.5% |
| Non-compliance | 5 | 2.1% |
| Desire for conception | 5 | 2.1% |
| Failure of contraception | 2 | 0.8% |
| Side effects | 6 | 2.5% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Health and Contraception · Pharmaceutical Quality and Counterfeiting · COVID-19 Impact on Reproduction
Introduction
India was the first country in the world to launch a National Programme for Family Planning in 1952 and has undergone several transformations over time [1]. The focus of family planning in India has shifted from population control to promoting maternal, child, and newborn health. Despite the strides made in this area, the unmet need for contraception is 9.4% and 3.6% for spacing methods, respectively, according to the recent National Family Health Survey (NFHS-5) [2]. The immediate postpartum period provides a vital opportunity to promote uptake of contraception and to ensure that the woman has the opportunity to start contraception before her first ovulation. However, the choices during this period are limited and must be considered carefully [1].
Oral contraception is a reliable, convenient, and widely used method for limiting unintended pregnancies. Both combined oral contraceptive pills (estrogen-progestin) and progestin-only pills (minipills) are effective methods of contraception; however, progestin-only pills are considered safer in the postpartum period [3]. In 1967, the Central Drug Research Institute (CDRI), Lucknow, India, synthesized a non-steroidal, once-a-week, oral contraceptive pill, centchroman (ormeloxifene). The drug was approved for marketing in 1991. In April 2016, the Ministry of Health and Family Welfare, India, introduced the drug, free of cost, in the National Family Planning Programme with the name “Chhaya” [4]. It is non-hormonal, taken once a week, and acts as a selective estrogen modulator (SERM) and has weak estrogenic and potent anti-estrogenic properties. It has an anti-estrogenic effect on reproductive organs and an estrogenic effect on bones. It prevents pregnancy by inhibiting implantation with no interference with ovulation and the hypothalamic-pituitary-ovarian axis [4,5]. It is free from steroidal side effects, including carbohydrate metabolism, lipid metabolism, blood pressure, and coagulation factors, and hence a safe option for women who cannot take steroidal pills [6]. It is safe during breastfeeding and is not associated with the side effects commonly seen with hormonal contraceptive pills [7,8].
Despite these benefits, its uptake and recognition beyond India have remained low, with limited studies on its acceptance and continuation during the postpartum period [4-8]. The goal of the present study is to evaluate and assess the acceptability, compliance, safety, and effectiveness of centchroman among postpartum women at a tertiary care facility in North India. This study adds longitudinal, real-world evidence on centchroman use using structured telephonic follow-up. It identifies access-related barriers, rather than side effects, as the primary cause of discontinuation, highlighting key programmatic gaps in postpartum family planning services.
Materials and methods
Study design
This was a hybrid observational study comprising a cross-sectional component to assess acceptability and satisfaction, and a longitudinal follow-up component to evaluate compliance, continuation, side effects, and failure rates among centchroman users, conducted over a period of two years, from January 2023 to December 2024.
Study setting
The study was carried out at the Family Planning Clinic, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences (AIIMS), New Delhi, a tertiary care center in North India. Institutional Ethics Committee approval was obtained.
Study objectives
The objective of this study was to assess the acceptability and compliance of centchroman among postpartum women at a tertiary care center in North India. Secondary objectives included evaluating continuation rates, side-effect profile, user satisfaction, willingness to recommend the method, reasons for discontinuation, and failure rate.
Study population
Using consecutive sampling, women aged 18-40 years who delivered at or beyond 20 weeks of gestation and accepted centchroman as a postpartum contraceptive method were included. Initiation occurred during the immediate postpartum period (prior to discharge, mostly within one week), and only women who consented and were available for telephonic follow-up between January 2023 and December 2024 were enrolled.
Women aged more than 40 years and those with a history of recent jaundice, chronic infections (including tuberculosis), polycystic ovarian disease, chronic liver disease, chronic kidney disease, hepatitis B or C infection, malignancy, or severe allergic conditions were excluded. Women who could not be contacted due to incorrect contact details or were unable to comply with follow-up because of residence in remote areas were also excluded.
Data collection and follow-up
Of the 900 postpartum women screened, 352 were excluded. Among the 548 eligible women, 307 did not participate further because they either declined centchroman, chose no contraception or an alternative method, or were unreachable by telephone. All eligible women received standardized counseling regarding centchroman, including its dosing schedule, mechanism of action, benefits, and possible side effects. A one-month supply of the drug was provided at the time of discharge, and participants were instructed to initiate the medication immediately as per the recommended regimen.
Follow-up was conducted telephonically using a structured questionnaire. Data collected included sociodemographic characteristics, obstetric and contraceptive history, knowledge and usage patterns of centchroman, compliance, continuation, side effects, and overall satisfaction with the method.
Outcome measures
The outcomes assessed were acceptance, patient satisfaction, compliance, continuation rate, side effects, and failure rate. Failure was defined as the occurrence of pregnancy during centchroman use.
Statistical analysis
Data were entered into Microsoft Excel (Microsoft Corp., Redmond, WA) and analyzed using the Statistical Package for the Social Sciences (SPSS) version 21.0 (IBM Corp., Armonk, NY). Categorical variables were summarized as frequencies and percentages, while continuous variables were expressed as means.
Results
The mean age of users was 28.2 years (range: 18 to 39 years), with the majority aged between 24 years and 34 years (Table 1). Most users were primiparous (67%) (Table 2). In around 72% of women, centchroman was initiated in the postpartum period, 26% during the interval period, and 2% post-abortion (Table 3).
Around 80% (191 women) were not using any contraception before centchroman; their stated reason was to achieve conception or the use of natural contraceptives. Out of 20% (N=50) women who had ever used contraception before using centchroman, the majority were using barrier contraception (70%), followed by intrauterine devices and combined hormonal pills.
All centchroman acceptors used it for at least one month, 70% up to three months, and 58% for 12 months or more. The discontinuation rate was highest within the first three months of usage (73%), as shown in Figure 1. Most side effects were also reported in the first three months. Nearly all users (99.6%) received pills from the hospital; a few (2.5%) accessed nearby dispensaries.
Duration of centchroman use among acceptors
No serious side effects were reported. Around 44 centchroman users (18%) reported minor side effects, as shown in Table 4. Most of the side effects occurred within three months of usage.
Around 93% of users were satisfied (gave a score of excellent or good), and 88% would recommend it to others. About 96% understood the dosing schedule, and 85% used alarms for adherence.
Out of 241 women studied, two became pregnant due to user failure, where they missed the pills; the Pearl Index was 0.42 HWY.
Around 61% women (N=147) reported current use of centchroman, and 94 women discontinued the drug. The common reasons for discontinuation were access issues and alternate methods (12% each), followed by staying away from their partner (7.5%), side effects (2.5%), and desire for conception (2.1%), as shown in Table 5.
Around 29% (n=29) of the women who stopped the pill at one month reported that they had used up the strip given at the time of discharge and were unable to follow up due to the distance from the medical facility.
Discussion
This study shows centchroman’s good acceptability among postpartum women. The majority were young, lactating mothers who are an ideal group for centchroman due to its safety during breastfeeding. Delayed menses was the most common side effect, consistent with prior studies (8-26%) [6-7,9-15]. The Pearl Index of 0.42 HWY aligns with published efficacy (0.2-2.0), and the low failure rate suggests high effectiveness when used correctly [3,7,9-11,14-15].
In the present study, the mean age of centchroman users was 28.2 years (range 18-39 years), with the majority of women in the age group of 24-34 years, comparable with other Indian studies [6,9-11]. Women over the age of 40 were excluded from the study. The majority of our acceptors were lactating, and there were no side effects observed in the newborn, as validated by Gupta et al. [12] and Paliwal et al. [8]. The fact that a very small amount of centchroman gets secreted in the breast milk makes centchroman a promising candidate for contraception during lactation [8,12]. The satisfaction rate (93%) mirrors findings from other studies [7,11]. Most users could manage the weekly regimen with digital reminders. However, discontinuation due to access issues, especially after using up the discharge pack, highlights the need for improved drug availability and counseling.
The drug is both safe and effective and is included in the National Family Planning Programme [3]. Around 82% of users had no side effects. Menstrual complaints, especially delayed menses, were the most common side effects among centchroman acceptors, similar to what was reported in the literature. Delayed menstrual cycles were reported in around 10.7% users, which supports the existing literature, ranging from 8-26% [6-7, 9, 11-15]. Systemic side effects were very few and were comparable to the incidence in the general population [3]. The Indian national guidelines mention menstrual delay among 8% of centchroman users [3] and do not mention any other side effects.
The present study shows the efficacy of 99.5%, with two pregnancies due to user failure (Pearl index: 0.42 HWY). This is similar to the National Manual of Oral Contraceptive Pills (efficacy rate of 98-99%) [3], and Miuli et al. [7] having a Pearl index of 0.8 and a low failure rate, compared to Nair et al. [10], Doke et al. [9], and Sarmalkar et al. with a Pearl index of 1.8, 2.0, and 1.0, respectively [14]. In another study by Radhika et al., centchroman had a Pearl index of 0.2 [15], and Gupta et al. reported no failure rate [11].
In our study, around 225 (93%) out of 241 centchroman users were satisfied, and 85% of users were able to take the pill regularly. We could only find two studies in the literature on the satisfaction rate among centchroman users. A study by Gupta et al. showed a satisfaction rate of 95% among centchroman users, and the satisfaction rate and continuation rate were similar to postpartum intra-uterine contraceptive devices (PPIUCD) at six months [11]. Another study by Miuli et al. had a satisfaction rate of 94%, which was higher than that of combined oral contraceptives among post-abortal patients. All acceptors used the drug for one month, and 70% for three months. The rate of discontinuation was maximum in the first three months of usage, with major reasons being side effects and accessibility issues. The major reason was the inability to follow up from remote areas (12%), which was even higher in users who discontinued after a month, where they finished the strip provided at discharge and were unable to procure another. Other reasons were temporarily staying away from partner (7.4%) and adoption of alternative contraception (12%). Around 2% users discontinued due to non-compliance, 2% due to side effects, and 2% due to the desire for conception. The high satisfaction rate, coupled with a low side-effect profile, suggests centchroman is well-received when users are properly counselled and have consistent access [7].
The most cited reason for discontinuation, non-availability, highlights the need for bridging accessibility gaps. Low prior contraceptive use among participants points to centchroman’s unique acceptability as a first method. However, gaps in compliance and inconsistent access remain key barriers. Addressing these through improved counselling, follow-up, and supply chain mechanisms could enhance continuation and overall satisfaction. These results support integrating centchroman into postpartum contraceptive counseling. Strategies like antenatal counseling, referral linkages for resupply, and mHealth reminders could reduce discontinuation and enhance continuity.
However, the study highlights critical challenges, particularly related to continuity and accessibility. A significant proportion of discontinuations occurred due to logistical hurdles, such as the inability to obtain refills from remote areas or a lack of structured follow-up. This points to the urgent need to integrate centchroman more robustly within the supply chain, including through primary health centres and community outreach.
Digital health tools such as SMS-based reminders and follow-up calls, along with routine antenatal counseling, can significantly enhance compliance and reduce early discontinuation. Training health workers in centchroman counseling, including information on side effects and proper intake schedule, will further support users. Additionally, the high proportion of first-time contraceptive users in this cohort suggests that centchroman could serve as an effective entry point into family planning programs, particularly among women hesitant to use hormonal methods.
Therefore, patient education in the form of contraceptive counselling during antenatal visits, labor ward admission, and immediate postpartum should be strengthened. Counselling the users to follow up at their nearby healthcare facility for drug procurement will improve the continuation rate. Mobile applications like voice messages for follow-up dates or reminders will help the patient and the healthcare facility keep track.
The study has certain limitations. Being a single-center study conducted at a tertiary care referral hospital managing predominantly high-risk pregnancies, the findings may not be fully generalizable to the general postpartum population or to primary and secondary healthcare settings. The cross-sectional design limits assessment of long-term continuation rates, effectiveness, and delayed adverse effects. Outcomes such as compliance, satisfaction, and side effects were self-reported during telephonic follow-up and are therefore subject to recall and social desirability bias. Additionally, the absence of a comparison group using other contraceptive methods limits direct comparative evaluation of acceptability and continuation. Finally, logistical barriers affecting drug availability may have influenced discontinuation rates and user experiences.
Conclusions
Centchroman is a safe, effective, and acceptable non-hormonal contraceptive with strong potential for postpartum family planning programs in India. Its once-a-week dosing, minimal side effects, and suitability for breastfeeding women make it particularly advantageous. To fully realize its potential, programmatic efforts should focus on expanding access through consistent supply at peripheral health facilities, improving user education through targeted counseling, and leveraging mobile health technologies to support adherence. Incorporating centchroman into the broader contraceptive method mix with sustained investment in training, monitoring, and community-based promotion can significantly enhance contraceptive choice and autonomy for women in India. Further large-scale, prospective studies are needed to comprehensively evaluate long-term safety, side effects, adherence, and continuation of centchroman under routine programmatic conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ministry of Health and Family Welfare, Government of India. National Family Planning Programme: National Health Mission. 1 2026 2025 https://nhm.gov.in/index 1.php?lang=1&level=2&sublinkid=821&lid=222
- 2Ministry of Health and Family Welfare, Government of India. Family Planning Division: India’s Vision FP 2020 1 2026 2014 https://advancefamilyplanning.org/sites/default/files/resources/FP 2020-Vision-Document%20India.pdf
- 3Family Planning Division, Ministry of Health and Family Welfare, Government of India. Reference Manual for Oral Contraceptive Pills 1 2026 2015 https://nhm.gov.in/images/pdf/programmes/family-planing/guidelines/Reference_Manual_Oral_Pills.pdf
- 4Scoping review to map evidence on mechanism of action, pharmacokinetics, effectiveness and side effects of centchroman as a contraceptive pill BMJ Open Kabra R Allagh KP Ali M Jayathilaka CA Mwinga K Kiarie J 092019 http://10.1136/bmjopen-2019-03037310.1136/bmjopen-2019-030373 PMC 679740231594884 · doi ↗ · pubmed ↗
- 5Centchroman: A safe reversible postcoital contraceptive with curative and prophylactic activity in many disorders Front Biosci (Elite Ed) Kamboj VP Ray S Anand N 114102018 http://10.2741/e 8072893060310.2741/e 807 · doi ↗ · pubmed ↗
- 6Centchroman, a selective estrogen receptor modulator, as a contraceptive and for the management of hormone-related clinical disorders Med Res Rev Singh MM 3023472120011141093310.1002/med.1011 · doi ↗ · pubmed ↗
- 7A study to compare acceptability, safety and continuation rates of combined hormonal pill and centchroman as post abortion contraceptives Int J Reprod Contracept Obstet Gynecol Miuli I Dewan R Agarwal K 33503359232020
- 8Excretion of centchroman in breast milk Br J Clin Pharmacol Paliwal JK Grover PK Asthana OP Nityanand S Gupta RC 485486381994789359410.1111/j.1365-2125.1994.tb 04388.x PMC 1364886 · doi ↗ · pubmed ↗