Acute pancreatitis due to afferent loop obstruction treated by endoscopic ultrasound-guided transpancreatic afferent limb drainage
Takashi Ito, Tsukasa Ikeura, Ayaka Takaori, Koh Nakamaru, Masataka Masuda, Shinji Nakayama, Makoto Naganuma

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
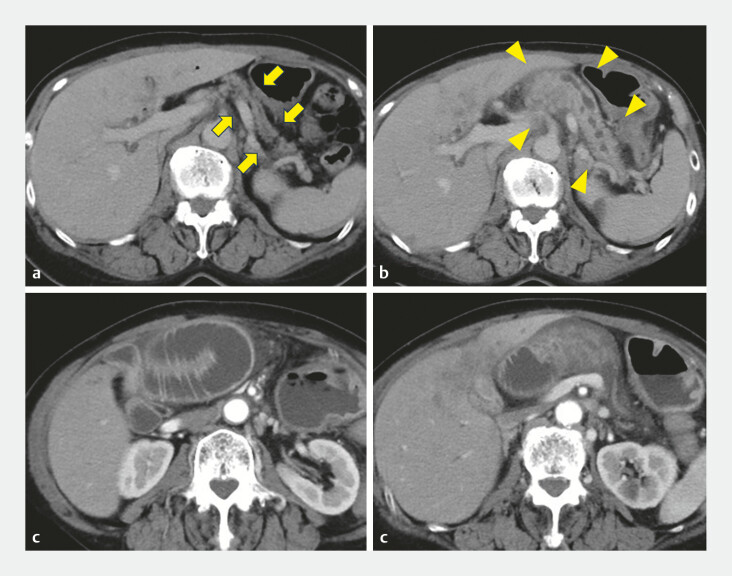 Fig. 1
Fig. 1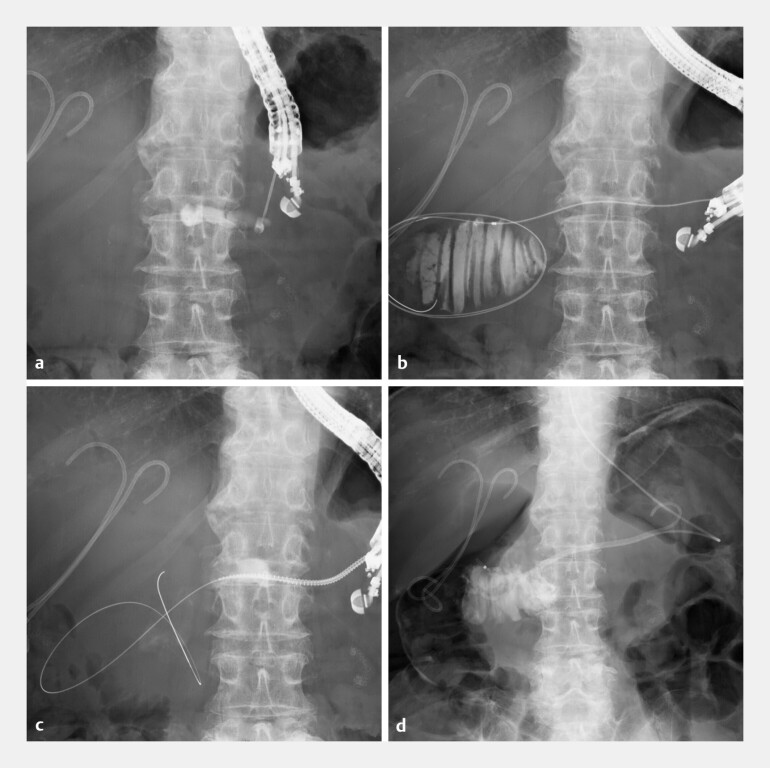 Fig. 2
Fig. 2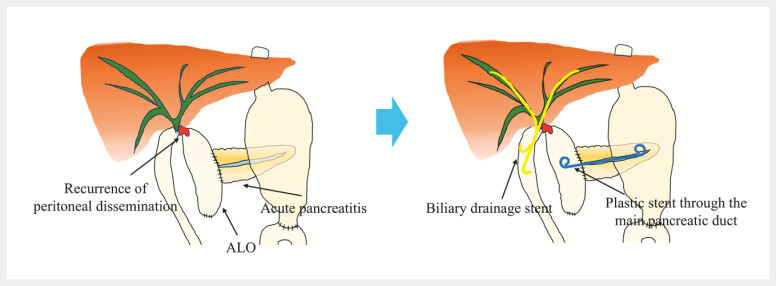 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatitis Pathology and Treatment · Gallbladder and Bile Duct Disorders · Pancreatic and Hepatic Oncology Research
Afferent loop obstruction (ALO) is a rare mechanical complication occurring in 0.3–1.0% of patients after gastrectomy 1 . Elevated intraluminal pressure in the afferent loop can lead to cholangitis or pancreatitis. Recently, endoscopic transluminal stent placement using balloon-assisted endoscopy 2 or endoscopic ultrasound (EUS 3 ) has been reported as an effective treatment. We describe the first successful case of the endoscopic treatment of ALO complicated with acute pancreatitis by an EUS-guided transpancreatic approach ( Video 1 ).
Endoscopic ultrasound-guided transpancreatic afferent limb drainage.Video 1
A 71-year-old woman with a history of gallbladder cancer who had undergone pancreaticoduodenectomy 5 years earlier presented with fever and abdominal pain. Computed tomography revealed dilation of the afferent limb and pancreatic enlargement with dilation of the main pancreatic duct (MPD) to 6 mm, compared with images obtained 3 months earlier ( Fig. 1 ). She was diagnosed with acute pancreatitis secondary to ALO.
Computed tomography performed 3 months before admission and at the time of hospitalization: a pancreatic parenchymal atrophy 3 months before admission (yellow arrow); b swelling of the pancreatic parenchyma and dilated main pancreatic duct (yellow arrowhead); c, d dilation of the afferent loop at the blind end.
A short-type double ballon endoscope (EI-580BT; Fujifilm, Tokyo, Japan) reached the choledochojejunal anastomosis; however, the dilated blind end where the pancreaticojejunal anastomosis was located could not be accessed due to peritoneal dissemination. Histopathological examination of endoscopic biopsy specimens revealed adenocarcinoma. As a result, decompression of the afferent limb was not achieved, and only biliary stents were placed. Consequently, we planned to perform EUS-guided transpancreatic afferent limb drainage. Under EUS guidance, a 19-gauge needle was inserted into the MPD, and a guidewire was advanced across the pancreaticojejunal anastomosis into the blind end. There was no pancreatic duct stricture. The fistula was dilated using a drill dilator. A plastic stent and a nasodrainage tube were placed into the dilated blind end ( Fig. 2 ). Six days after the procedure, the nasodrainage tube was removed because both afferent loop dilation and pancreatitis improved promptly ( Fig. 3 ). No recurrence of pancreatitis was observed without removing the stent until the patientʼs death.
a–d Placement of a plastic stent and a nasodrainage tube into the dilated afferent loop at the blind end via the main pancreatic duct using endoscopic ultrasound-guided transpancreatic afferent limb drainage. a Under EUS guidance (UCT260; Olympus Co., Ltd, Tokyo, Japan), a 19-gauge needle (SonoTip Pro Control; Medico’s Hirata Inc., Osaka, Japan) was inserted into the dilated main pancreatic duct. b A 0.025-inch guidewire (Visiglide2; Olympus) and an MTW catheter (ABIS, Tokyo, Japan) were advanced across the pancreaticojejunal anastomosis into the blind end. c The fistula was dilated using a drill dilator (Tornus ES; Asahi Intecc, Aichi, Japan). d A plastic stent (6-Fr 7-cm, pigtail type, Zimmon; COOK Medical, Bloomington, IN, USA) and a nasodrainage tube (5Fr; Create Medic) were placed into the dilated blind end. EUS, endoscopic ultrasound.
Schematic illustration of EUS-guided afferent limb drainage via the main pancreatic duct. EUS, endoscopic ultrasound.
EUS-guided transpancreatic afferent limb drainage may represent a feasible and effective endoscopic treatment for ALO associated with acute pancreatitis.
Endoscopy_UCTN_Code_CCL_1AC_2AH Endoscopy_UCTN_Code_TTT_1AS_2AK Endoscopy_UCTN_Code_TTT_1AS_2AI
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aoki M Saka M Morita S Afferent loop obstruction after distal gastrectomy with Roux-en-Y reconstruction World J Surg 2010342389239220458583 10.1007/s 00268-010-0602-5 · doi ↗ · pubmed ↗
- 2Ito T Shimatani M Masuda M Efficacy and safety of endoscopic stent placement for afferent loop obstruction using a short double-balloon endoscopy DEN Open 202222 E 15410.1002/deo 2.154PMC 930774635898829 · doi ↗ · pubmed ↗
- 3Yamamoto K Tsuchiya T Tanaka R Afferent loop syndrome treated by endoscopic ultrasound-guided gastrojejunostomy, using a lumen-apposing metal stent with an electrocautery-enhanced delivery system Endoscopy 201749 E 270E 27228799148 10.1055/s-0043-115893 · doi ↗ · pubmed ↗