Lumen-apposing metal stent gastrojejunostomy for biliary drainage of an obstructive biliodigestive anastomosis: an endoscopic resolution avoiding surgery
Ottavia De Simoni, Irma Albergati, Carola Cenzi, Pierluigi Pilati, Mario Gruppo, Alberto Fantin

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
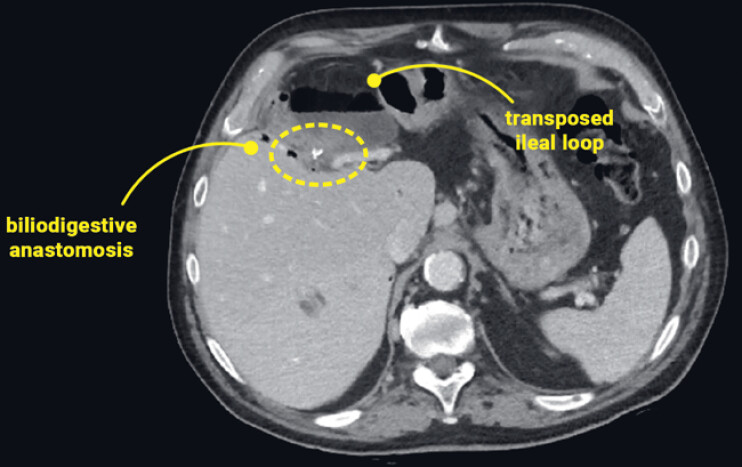 Fig. 1
Fig. 1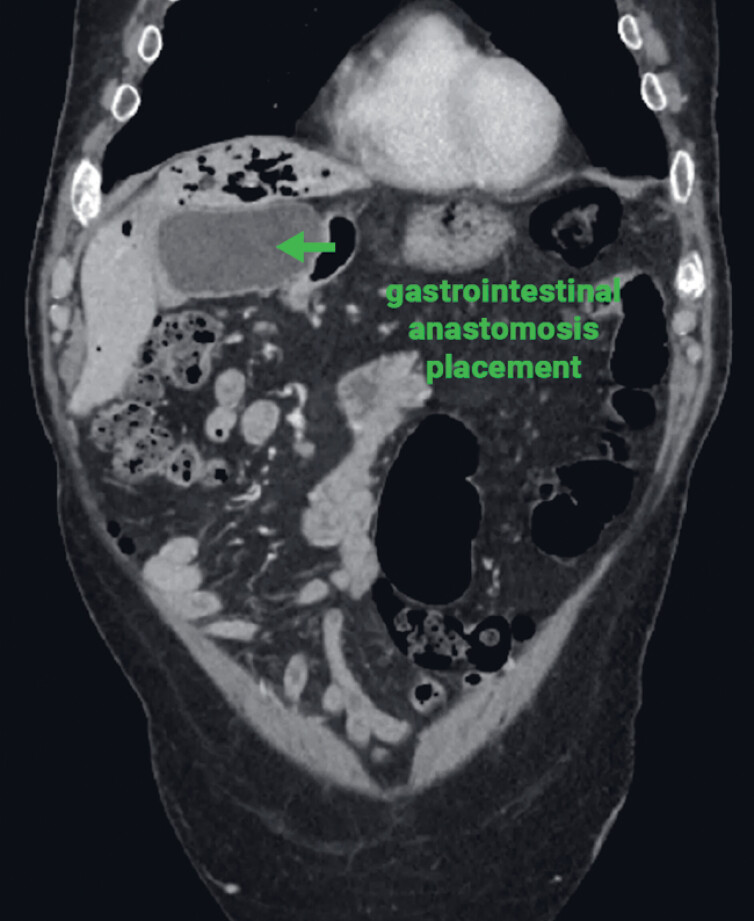 Fig. 2
Fig. 2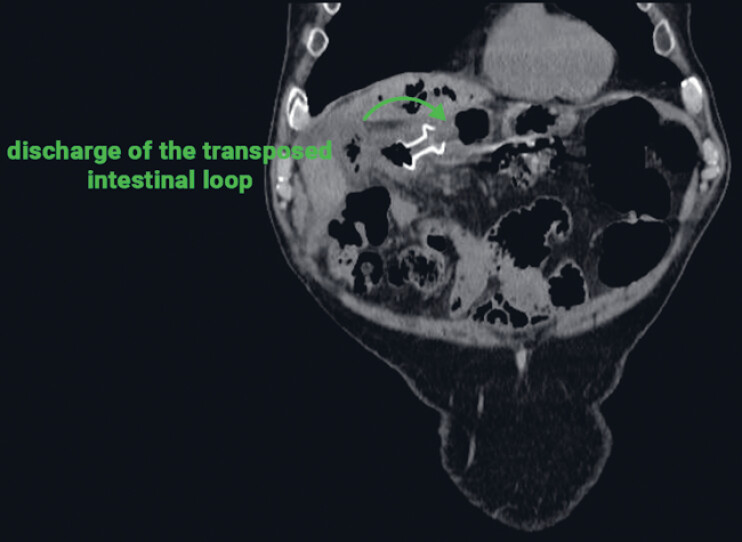 Fig. 3
Fig. 3- —Ricerca Corrente
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Biliary and Gastrointestinal Fistulas
A 76-year-old man with a long-standing history of recurrent cholangitis was referred to our department. Twenty years earlier, he had undergone surgery to remove a large hepatic cyst in segments S5–S6. The postoperative course was complicated by multiple reoperations for choleperitoneum, ultimately requiring the creation of a biductal hepatico-jejunostomy anastomosis.
An abdominal computed tomography (CT) scan revealed the dilation of the afferent tract of the transposed jejunal loop, suggesting impaired drainage through the biliodigestive anastomosis ( Fig. 1 ). Although surgical revision was deemed technically feasible, it was associated with considerable operative complexity and high perioperative risk. Haase et al. described a case of an obstructed biliodigestive anastomosis in a patient with a progressive pancreatic cancer, in which the transgastric endoscopic ultrasound-guided placement of a lumen-apposing metal stent (LAMS) into the afferent jejunal was performed with good results 1 .
A preoperative abdominal CT scan showing the dilation of the afferent tract of the transposed loop with suspected impaired biliodigestive anastomosis discharge. CT, computed tomography.
For this reason, an endoscopic approach was considered ( Fig. 2 ). The patient subsequently underwent the transgastric endoscopic ultrasound-guided placement of a lumen-apposing metal stent (LAMS) into the afferent jejunal loop ( Fig. 3 ), as shown in Video 1 .
A preoperative CT scan showing the feasibility of the endoscopic ultrasound-guided placement of a LAMS between the gastric antrum and the afferent jejunal loop. CT, computed tomography; LAMS, lumen-apposing metal stent.
The final position of the stent between the prepyloric region and the afferent loop, demonstrating effective bile drainage into the stomach.
Lumen-apposing metal stent gastrojejunostomy is performed for biliary drainage of an obstructive biductal hepatico-jejunostomy anastomosis.Video 1
A CT scan performed 1 month after the procedure confirmed correct stent positioning, adequate biliary drainage through the anastomosis, and a marked reduction in intrahepatic bile duct dilation.
Approximately 1 year later, he reported two brief, self-limited episodes of fever. Endoscopic ultrasound showed the partial obstruction of the LAMS at the prepyloric site due to food debris. The material was removed, restoring unobstructed bile flow through the stent. Follow-up remained uneventful, and the patient remained asymptomatic.
This case highlights the feasibility, safety, and efficacy of LAMS placement as a minimally invasive alternative for managing impaired bile drainage following complex biliary surgery. In this patient, the endoscopic approach successfully resolved recurrent cholangitis, improved the quality of life, and, most importantly, avoided a highly complex surgical procedure with a considerable perioperative risk.
Endoscopy_UCTN_Code_TTT_1AS_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.