Evaluation of Pain and Oral Health-Related Quality of Life Associated With Fixed Orthodontic Treatment in Adults: A Systematic Review and Meta-Analysis
Omar A Rasol, Mohammad Y. Hajeer, Ahmad S. Burhan, Huda Abutayyem, Samer T. Jaber, Alaa Oudah Ali Almusawi

TL;DR
This study reviews how pain and quality of life change in adults during orthodontic treatment, finding that pain peaks early but decreases over time.
Contribution
The study provides a systematic review and meta-analysis focusing specifically on pain and quality of life in adult orthodontic patients.
Findings
Pain intensity peaks 24 hours after treatment activation and decreases significantly within a week.
Oral health-related quality of life initially declines but improves measurably within a month.
The certainty of evidence for these outcomes is rated as very low to low.
Abstract
Fixed orthodontic treatment is commonly associated with pain and discomfort, particularly during the initial stages, which may influence patient adherence and satisfaction; however, a comprehensive synthesis of evidence, specifically focused on the adult population, remains limited. This systematic review aimed to evaluate pain and oral health-related quality of life (OHRQoL) in adult patients undergoing fixed orthodontic treatment. Electronic searches were conducted up to August 2025 across multiple databases, including PubMed®, Web of Science™, Scopus®, Google™ Scholar, PsycINFO®, EMBASE®, and the Cochrane Library, with no restrictions on publication date or language. Observational studies, randomized controlled trials (RCTs), and controlled clinical trials (CCTs) involving patients aged 18 years or older, treated with conventional fixed appliances, were included. Two reviewers…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
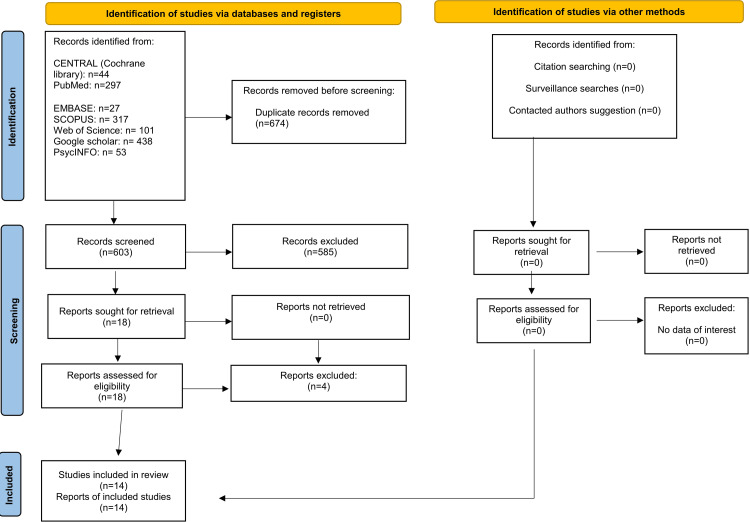 Figure 1
Figure 1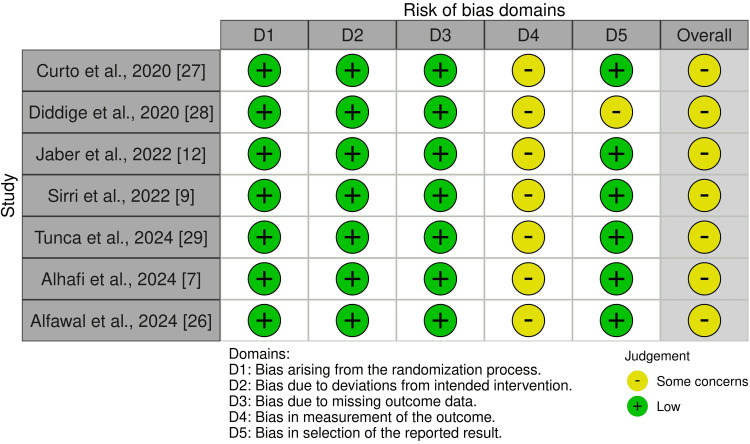 Figure 2
Figure 2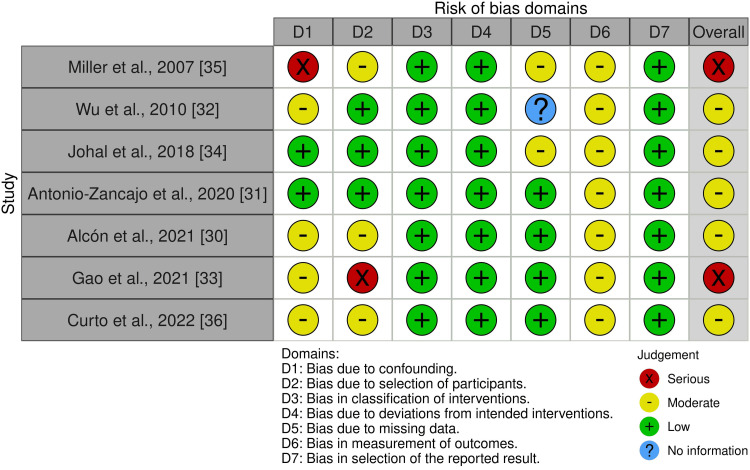 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5| Aspects of the search strategy | Keywords |
| Type of malocclusion | Permanent dentition, permanent occlusion, malocclusion, class I malocclusion, class II malocclusion, class III malocclusion, dental malocclusion, crowding, spacing, overjet, overbite, cross bite, adults, adult patients. |
| Type of orthodontic tooth movement or orthodontic appliance | Leveling, alignment, extraction, retraction, canine retraction, anterior segment retraction, intrusion, extrusion, expansion, distalization, fixed orthodontic treatment, fixed metallic appliance, conventional metallic appliance, fixed appliance, clear aligners, Invisalign, self-ligating braces, lingual orthodontic treatment, lingual orthodontic appliance, lingual appliance, removable, removable appliance. |
| Outcomes | Pain, swelling, tension, pressure, soreness, pain perception, pain intensity, pain assessment, discomfort, pressure sensation, pain threshold, pain duration, VAS, visual analog scale, numerical rating scale, NRS, Likert, self-reported pain, oral health-related quality of life, OHRQoL, quality of life, patient-reported outcomes, oral health impact profile, OHIP, OHIP-14, psychosocial impact, functional limitations, daily life interference, self-esteem, patient experience. |
| Authors | Study design | Number of patients/mean age | Intervention | Outcomes | Follow-up |
| Miller et al. (2007) [ | Prospective cohort | 60 patients FAT: 27 (6m, 21f) 28.6 ± 8.7, CAT: 33 (11m, 22f) 38 ± 12.4 | Fixed appliance treatment vs clear aligner therapy | Oral health-related quality of life (OHRQoL) (GOHAI) | Every day in the first week of treatment |
| Wu et al. (2010) [ | CCT | 60 patients: FAT: 30 (12m, 18f) 20.33 ± 4.205, LFA: 30 (8m, 22f) 21.63 ± 2.23 | Fixed appliance treatment vs lingual fixed appliance | Pain assessed via VAS | 1 week after appliance placement, 1 month, 3 months |
| Johal et al. (2018) [ | Prospective cohort | 58 patients (26m, 32f), 34.7 ± 12.1 | Fixed appliance treatment | Pain assessed via VAS | 4 h, 24 h, 3 days, and 7 days after each of 3 appointments (T0: bond-up, T1: first adjustment, T2: second adjustment) |
| Antonio-Zancajo et al. (2020) [ | CCT | 120 patients: FAT: 30 (13m, 17f), 24.7 ± 4.1; LFB: 30 (12m, 18f), 28 ± 9.7; LFA: 30 (13m, 17f), 33.8 ± 8.2; CAT: 30 (16m, 14f), 33.4 ± 5.1 | Fixed appliance treatment vs low-friction brackets vs lingual fixed appliance vs clear aligner therapy | 1. Pain assessed via VAS, 2. Oral health-related quality of life (OHRQoL) (OHIP-14) | Pain assessment: 4 h (T4h), 8 h (T8h), 24 h (T1), 2 days (T2), 3 days (T3), 4 days (T4), 5 days (T5), 6 days (T6), 7 days (T7) OHRQoL assessment: after one month of treatment |
| Diddige et al. (2020) [ | RCT | 36 patients (18-30 years): FAT: 12 (6m, 6f), SLBs: 12 (6m, 6f), CAT: 12 (6m, 6f) | Fixed appliance treatment vs self-ligating Damon brackets vs clear aligner therapy | Pain assessed via VAS | 4 hours (T1), 24 hours (T2), Day 3 (T4), and Day 7 (T5) |
| Curto et al. (2020) [ | RCT | 90 patients: FAT: 30 (9m, 21f) 23.5 ± 12.6, LFBs: 30 (13m, 17f) 18.87 ± 3.6, LFBO: 30 (13m, 17f) 22.6 ± 9.5 | Fixed appliance treatment vs low-friction brackets vs low-friction brackets + Orthospeed® gel | 1. Pain assessed via VAS, 2. Oral health-related quality of life (OHRQoL) (OHIP-14) | Pain assessment: 4 hours (T1), 8 hours (T2), 24 hours (T3), 2 days (T4), 3 days (T5), 4 days (T6), 5 days (T7), 6 days (T8), and 7 days (T9) after the start of the treatment. OHRQoL assessment: after one month of treatment |
| Alcón et al. (2021) [ | CCT | 140 patients: FAT: 70 (35m, 25f) 26.97 ± 7.23, CAT: 70 (33m, 37f) 31.74 ± 11.39 | Fixed appliance treatment vs clear aligner therapy | Pain assessed via VAS | Every month after the patient's monthly follow-up visit at 4 h (T1), 8 h (T2), 24 h (T3), 2 days (T4), 3 days (T5), 4 days (T6), 5 days (T7), 6 days (T8), and 7 days (T9), during the twelve-month study |
| Gao et al. (2021) [ | Prospective cohort | 110 patients: FAT: 55 (13m, 42f) 24.6 ± 5.2, CAT: 55 (13m, 42f) 26.0 ± 5.47 | Fixed appliance treatment vs clear aligner therapy | 1. Pain assessed via VAS, 2. Oral health-related quality of life (OHRQoL) (OHIP-14) | Pain assessment: every day from day 1 to day 14, OHRQoL assessment: day 1, day 7, day 14 |
| Curto et al. (2022) [ | Cross-sectional | 120 patients (52m, 68f), 19-45 years | Conventional fixed appliance | Oral health-related quality of life (OHRQoL) (OHIP-14) | One month after the start of the treatment |
| Jaber et al. (2022) [ | RCT | 36 patients: FAT: 18 (8m, 10f) 20.86 ± 1.98, CAT: 18 (9m, 9f) 21.27 ± 1.87 | Fixed appliance treatment vs clear aligner therapy | Oral health-related quality of life (OHRQoL) (OHIP-14) | Before treatment (T0), 1 week (T1), two weeks (T2), one month (T3), six months (T4), and 12 months (T5) after starting the treatment |
| Sirri et al. (2022) [ | RCT | 52 patients: FAT: 26 (6m, 20f) 21.30 ± 1.49, CORT: 26 (8m, 18f) 21.46 ± 1.76 | Fixed appliance treatment vs Fixed appliance treatment with corticision | Pain assessed via VAS | After one day of the onset of treatment (T0), seven days (T1), and 14 days (T2) |
| Tunca et al. (2024) [ | RCT | 60 patients: FAT: 30 (15m, 15f) 21.3 ± 3.37, CAT: 30 (15m, 15f) 23.65 ± 6.58 | Fixed appliance treatment vs clear aligner therapy | 1. Pain assessed via VAS, 2. Oral health-related quality of life (OHRQoL) (OHIP-14) | Pain assessment: at 0, 2, and 6 h after treatment and on days 1, 3, 7, 14, and 21. OHRQoL assessment: after the start of treatment (T1) and after 10 days (T10), and 20 days (T20) of treatment |
| Alhafi et al. (2024) [ | RCT | 36 patients: FAT: 18 (6m, 12f) 20.94 ± 2.38, MAA: 18 (5m, 13f) 21.89 ± 2.63 | Fixed appliance treatment vs modified aligner appliance | Oral health-related quality of life (OHRQoL) (OHIP-14) | Before beginning the treatment (T0), two weeks (T1), one month (T2), two months (T3) after the beginning of the treatment, and at the end of the treatment (T4) |
| Alfawal et al. (2024) [ | RCT | 44 patients: FAT: 22 (3m, 19 f) 24.22 + 2.99, CAT: 22 (5m, 17f) 25.40 ± 2.87 | Fixed appliance treatment vs clear aligner therapy | Oral health-related quality of life (OHRQoL) (OHIP-14) | Before the start of treatment (T0), 1 week (T1), 1 month (T2), 3 months (T3), 6 months (T4), after the initial bonding of the fixed appliance or delivery of the first aligner, and post-treatment (T5) |
| Authors | Pain (VAS 0-100 mm) | Oral health-related quality of life (OHRQoL) | |||||||||
| 1D | 1W | 2W | 1M | 3M | Assessment tool | 1D | 1W | 2W | 1M | 3M | |
| Miller et al. (2007) [ | - | - | - | - | - | GOHAI | 38 ± 23.38 | 59 ± 10.39 | - | - | - |
| Wu et al. (2010) [ | - | 59.2 ± 11 | - | 32.3 ± 8 | 9.7 ± 3.5 | - | - | - | - | - | - |
| Johal et al. (2018) [ | 26.35 ± 25.92 | 16.02 ± 21.75 | - | - | - | - | - | - | - | - | - |
| Antonio-Zancajo et al. (2020) [ | 50 ± 27 | 13 ± 16 | - | - | - | OHIP-14 | - | - | - | 3.8 ± 2.1 | - |
| Diddige et al. (2020) [ | 55.3* | 24.9* | - | - | - | - | - | - | - | - | - |
| Curto et al. (2020) [ | 45 ± 22 | 18 ± 19 | - | - | - | OHIP-14 | - | - | - | 3.0 ± 1.9 | - |
| Alcón et al. (2021) [ | 43.66 ± 19.47 | 16.49 ± 13.87 | - | 21.75 ± 1.984 | 6.42 ± 10.09 | - | - | - | - | - | - |
| Gao et al. (2021) [ | 42 ± 22.25 | 17 ± 13.3 | 9 ± 10.4 | - | - | OHIP-14 | 16 ± 12.6 | 11 ± 10.4 | 8.5 ± 8.9 | - | - |
| Curto et al. (2022) [ | - | - | - | - | - | - | - | - | - | 11.93 ± 2.19 | - |
| Jaber et al. (2022) [ | - | - | - | - | - | OHIP-14 | - | 22.88 ± 9.60 | 16.41 ± 9.27 | 14.12 ± 9.07 | - |
| Sirri et al. (2022) [ | 19.54 ± 7.76 | 2.231 ± 2.61 | 0.07 ± 0.27 | - | - | - | - | - | - | - | - |
| Tunca et al. (2024) [ | 56.7† | 23.7† | 13.3† | - | - | OHIP-14 | 18.73 ± 7.75 | - | 14.53 ± 7.07 | - | - |
| Alhafi et al. (2024) [ | - | - | - | - | - | OHIP-14 | - | 19.94† | - | 16.22† | - |
| Alfawal et al. (2024) [ | - | - | - | - | - | OHIP-14 | - | 25.18 ± 4.15 | - | 15.59 ± 2.91 | 11.46 ± 2.63 |
| Outcome time point | Quality assessment criteria | Number of patients, relative effect, and certainty | Comments | |||||||
| No. of studies | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | No. of patients | Relative (95% CI) | Certainty | ||
| Pain (VAS) - at 24 hours | 8 | Serious | Serious | Not serious | Serious | None | 311 | - | Very Low ⊕⊖⊖⊖a b c | High pain levels are consistently reported |
| Pain (VAS) - Day 1 vs Week 1 | 2 RCTs | Serious | Serious | Not serious | Serious | None | 56 | Relative effect (Cl 95%): MD 20.83 (11.7, 29.97) | Very Low ⊕⊖⊖⊖a b c | - |
| Pain (VAS) - 2 weeks | 3 | Serious | Serious | Not serious | Serious | None | 111 | - | Very Low ⊕⊖⊖⊖a b c | - |
| Pain (VAS) - at 1 month | 3 | Serious | Serious | Not serious | Serious | None | 100 | - | Very Low ⊕⊖⊖⊖a b c | Pain levels show variable patterns |
| Pain (VAS) - at 3 months | 2 | Serious | Serious | Not serious | Serious | None | 100 | - | Very Low ⊕⊖⊖⊖a b c | Low pain levels are consistently reported |
| OHRQoL (OHIP-14) - at 24 hours | 2 | Serious | Serious | Not serious | Serious | None | 85 | - | Very Low ⊕⊖⊖⊖a b c | Indicates initial impairment. Scores ranged from 16 to 18.73 |
| OHRQoL (OHIP-14) - at 1 week | 4 | Serious | Serious | Not serious | Serious | None | 113 | - | Very Low ⊕⊖⊖⊖a b c | - |
| OHRQoL (OHIP-14) - at 2 weeks | 3 | Serious | Serious | Not serious | Serious | None | 103 | - | Very Low ⊕⊖⊖⊖a b c | Shows improvement from baseline. Scores range from 8.5 to 14.53 |
| OHRQoL (OHIP-14) - Week 1 vs Month 1 | 2 RCTs | Serious | Not serious | Not serious | serious | None | 40 | Relative effect (Cl 95%): MD 9.5 (7.5, 11.5) | Low ⊕⊕⊖⊖a c | Meta-analysis shows significant improvement |
| OHRQoL (OHIP-14) - at 3 months | 1 RCT | Serious | Serious | Not serious | Serious | None | 22 | - | Very Low ⊕⊖⊖⊖a b c | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · Dental Anxiety and Anesthesia Techniques · Temporomandibular Joint Disorders
Introduction and background
Fixed orthodontic treatment is a widely employed technique for correcting dental malocclusions and achieving optimal occlusal relationships [1]. Brackets, arch wires, and bands are the key components of a fixed appliance, which are attached to the teeth to exert controlled forces to guide tooth movement, providing precise control over dental positioning [1,2]. Although newer forms of fixed appliances, such as ceramic braces and self-ligating brackets (SLBs), as well as aesthetic alternatives like clear aligners and lingual fixed appliances (LFAs), have emerged, the conventional fixed metallic orthodontic appliance remains the gold standard in orthodontic treatment [2].
Pain, as defined by the International Association for the Study of Pain, is “a negative sensory and emotional reaction linked to actual or possible injury to body tissue” [3]. Pain and discomfort are common symptoms of orthodontic treatment. This may discourage patients from initiating treatment; it may also affect their cooperation and adherence to the treatment plan, and the orthodontist’s instructions, all of which may negatively impact treatment satisfaction [4,5]. In orthodontics, pain is caused by the inflammatory response within the periodontal ligament following the application of force, and may vary in intensity and duration across treatment phases [6]. The assessment of pain intensity associated with orthodontic treatment has become a central focus in current studies [7-9]. The most practical and widely accepted approach involves patient self-reporting, using standardized scales such as the Visual Analog Scale (VAS), Numerical Rating Scale (NRS), and Verbal Rating Scale (VRS) [10].
Oral health-related quality of life (OHRQoL) is a comprehensive concept that describes how oral health influences an individual’s physical comfort, emotional state, and social functioning. It includes factors such as pain, functional limitations, emotional distress, and social interactions resulting from oral conditions or treatment [11]. In orthodontics, OHRQoL has become a common outcome measure, as malocclusions and their correction can significantly influence patients’ self-esteem, daily functioning, and satisfaction with treatment [7,12-14].
Several systematic reviews have been conducted on pain and quality of life associated with orthodontic treatment [2,5,15-17]. The majority of systematic reviews have either failed to isolate adult patients as a distinct population or centered their comparisons on conventional appliances versus clear aligners [2,16,17]. The review by Inauen et al. addressed the topic of the pain profile in patients undergoing leveling and alignment by fixed orthodontic appliances; however, the authors included studies involving patients of mixed age groups [5]. Meanwhile, the review by Cheng et al. has focused on the effect of analgesics in controlling pain during orthodontic treatment, with the use of non-steroidal anti-inflammatory drugs (NSAIDs) being a key inclusion criterion for the selected studies [15]. The recent review by Johal et al. compared labial fixed appliances, palatal fixed appliances, and clear aligners in terms of pain, quality of life, and side effects in adult patients [18]. While their work provides a valuable comparison across multiple orthodontic modalities, a dedicated synthesis focusing exclusively on conventional fixed appliances in the adult population remains warranted. This leaves a significant gap in understanding how treatment with the conventional fixed orthodontic appliance affects adult patients in terms of pain experience and its impact on OHRQoL, as the majority of reviews have either failed to isolate adult patients as a distinct population or have focused on comparisons between several modalities. Adult patients differ physiologically and psychosocially from younger patients, with potentially heightened sensitivity to pain, and differing expectations regarding treatment outcomes [19].
Moreover, current reviews have not examined newer or less conventional alternatives, such as lingual fixed appliances or treatments employing acceleration techniques (physical or surgical), in comparison to conventional fixed appliances. Therefore, the current work aims to answer the following review question: what is the level of pain associated with fixed orthodontic treatment, and how does it affect the quality of life in adult patients?
Review
Materials and methods
Preliminary Search and Protocol Registration
A pilot PubMed search was conducted before drafting the final protocol to verify that no comparable studies were available and to identify relevant literature. The protocol was recorded in PROSPERO during the initial stages of this study (CRD420251231931). This systematic review was carried out in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [20,21] and the checklist and methodology recommendations provided in the Cochrane Handbook for Systematic Reviews of Interventions [22].
Eligibility Criteria
This systematic review explicitly defined its inclusion and exclusion criteria. The PICOS framework (population, intervention, comparison, outcomes, and study design) was used to define individuals, interventions, comparisons, outcomes, and study design. The target population consisted of adult patients aged 18 years or older who had undergone treatment with a conventional fixed metallic appliance. Regarding comparisons, no direct comparison was targeted in this review. However, studies that compare conventional fixed appliances to other orthodontic appliances were included if they reported relevant outcomes. The primary outcome of this review was patient-reported pain at the following time points: one day, one week, two weeks, one month, and three months. The effect on patients’ OHRQoL, measured using different scales at the same previous sequence of time points, was the secondary outcome. Observational studies (cross-sectional and cohort) were primarily targeted. Randomized controlled trials (RCTs) and controlled clinical trials (CCTs) were also included if they provided relevant outcome data. The following studies were excluded: those that did not specify adults as participants and included patients of all ages; those involving pain‑relief medications; studies with fewer than 10 participants in the experimental group; studies lacking sample reporting; case reports; case series; opinion pieces; reviews; and technique-description articles.
Information Sources
The electronic search keywords are presented in Table 1, while the full search strategy is detailed in Appendix 1. The initial search was conducted in August 2025 by two reviewers (OAR and MYH) without time restrictions, using PubMed®, Web of Science™, Scopus®, Google™ Scholar, PsycINFO®, EMBASE®, and the Cochrane Library. In addition, the reviewers manually examined the reference lists of all included studies.
Search Strategy and Study Selection
The study selection process went through two phases. Initially, two reviewers (OAR and MYH) independently screened the titles and abstracts of the articles retrieved from electronic databases, followed by a full-text evaluation of potentially eligible studies. Articles that failed to meet the inclusion criteria were excluded. In case of disagreement, the two reviewers consulted the third author (ASB) in order to reach a solution.
Data Collection Process
Two reviewers (OAR and MYH) extracted data from the included studies and compiled it into tables. The information gathered comprised general details (author and year of publication), study design, mean age, sample size, intervention types, follow-up period, and reported outcomes. Any disagreements between the reviewers were settled through discussion and, when necessary, consultation with the third author (ASB).
Risk of Bias Assessment in Individual Studies
Two reviewers independently assessed the risk of bias in the included studies using the RoB‑2 tool for RCTs [23] and the ROBINS-I tool for non-randomized trials [24]. Their assessments were then compared, and any disagreements were resolved through discussion and consultation with the third author (ASB) until consensus was achieved. For RCTs, bias was evaluated across the following domains and categorized as “low,” “high,” or “some concerns”: randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of reported results. The overall risk of bias of the included studies was evaluated as follows: "low risk of bias" if all fields were at low risk of bias; "some concerns" if at least one domain was evaluated as "some concern" but not at high risk of bias for any domain; "high risk of bias" if at least one or more fields were evaluated at high risk of bias, or if there were some concerns for multiple domains, in a way that notably undermines the reliability of the results.
For non-randomized trials, the following domains were evaluated: bias arising from confounding, participant recruitment methods, categorization of interventions, deviations from intended interventions, missing data, the measurement of outcomes, and bias arising from the selection of the reported outcomes. Overall risk-of-bias assessment of non-randomized included studies was evaluated as follows: low if all domains were low risk; moderate if domains were consistently low or moderate; serious if at least one domain was serious but none critical; critical if any domain was critical; and no information if the study lacked serious or critical ratings but had incomplete data in key domains.
The strength of the evidence was assessed using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) framework, which classified the certainty of outcomes as high, moderate, low, or very low [25].
Data Synthesis
Review Manager (RevMan), Version 5.4 (The Cochrane Collaboration, The Nordic Cochrane Center, Copenhagen, Denmark), was utilized to perform the meta-analysis. Continuous outcomes were analyzed with a random‑effects model, based on the inverse variance method, reporting mean differences and 95% confidence intervals. Heterogeneity was considered significant at p < 0.05, and the I² index was used to quantify its magnitude. Forest plots were generated to present findings graphically. Evidence quality was systematically evaluated using the GRADE approach.
Results
Study Selection
After conducting the electronic and manual searches, 1,275 articles were identified; the number dropped to 603 after duplicates were removed. After reviewing the titles and abstracts of these publications, 18 potential articles remained, and those that did not meet the inclusion criteria were excluded. Upon reviewing the full text of all 18 studies, four were found not to meet the inclusion criteria. The reasons for excluding each study are explained in Appendix 2. Following this selection process, 14 papers were included in the qualitative synthesis of the data. Figure 1 shows the PRISMA flow diagram of the reviewing process.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram illustrating the selection of included studies
Characteristics of the Included Studies
The characteristics of the included studies are summarized in Table 2. Fourteen studies were included in this review, comprising seven RCTs [7,9,12,26-29], three CCTs [30-32], three cohort studies [33-35], and one cross-sectional study [36]. A total of 1,022 patients were included across all studies, among whom 396 received treatment with conventional fixed orthodontic appliances, while the remainder received other orthodontic modalities (such as clear aligners or lingual appliances). Across all included studies, both males and females were represented - with females comprising the majority in most samples (61.25%) - and no study was conducted on a single-gender population. The male-to-female ratio was approximately 2:3. The mean age of participants across the included studies ranged from approximately 18.87 to 38 years, with most samples concentrated in the 20s to early 30s.
Fixed appliance treatment (FAT) was the primary treatment modality in all included studies. Several studies incorporated comparative groups, including clear aligner therapy (CAT) [12,26,28-31,33,35], LFAs [31,32], low-friction brackets (LFBs) [31], and SLBs [28]. Additionally, corticision as an adjunctive acceleratory therapy [9] and hybrid approaches- such as the integration of Orthospeed® gel [27] were also explored; however, two studies assessed the effects of FAT independently [34,36].
Regarding pain assessment, 9 of the 14 included studies measured pain using the VAS [9,27-34]. Seven of the nine studies initiated pain assessment within the first few hours following appliance placement [9,27-31,34], one study began on the following day [33], and one study commenced evaluation one week after appliance placement [32]. Patient follow-up durations varied across the nine studies, ranging from 7 days [27,28,31] to 12 months [30]. Most studies followed patients for short periods (e.g., one to five weeks) [9,27-29,31,33], while others extended follow-up to 3 [32] or 12 months [30]. However, one study reported follow-up based on three appointments [34].
Regarding OHRQoL assessment, 9 of the 14 included studies evaluated OHRQoL using validated instruments at different stages of orthodontic care [7,12,26,27,29,31,33,35,36]. Three out of the nine studies conducted the initial assessment before starting treatment [7,12,26], while three studies conducted the assessment one month after treatment began, and this was the only assessment [27,31,36]. Three studies conducted the initial assessment on the first day of treatment [9,33,35]. Follow-up durations for OHRQoL varied across studies, ranging from 1 week [35] to 12 months [12], and, in some cases, extended until treatment completion [7,26].
Notably, pain and OHRQoL assessments were included in 4 of the 14 studies to provide a more comprehensive evaluation of patient-centered outcomes [27,29,31,33].
Risk of Bias Within Studies
Risk of bias was assessed for seven RCTs using the ROB 2 tool. All were rated as having “some concerns,” most commonly driven by lack of participant blinding and outcome-measurement domain concerns for self-reported pain and OHRQoL [7,9,12,26-29]. For the seven non-randomized studies, the ROBINS-I tool was applied: five were judged to have a moderate risk of bias [30-32,34,36], while two were considered at serious risk [33,35]. The “serious” ratings were principally due to selection bias/confounding from non-random allocation or self-selection of treatment (e.g., socioeconomic differences between aligner and bracket groups) and baseline imbalances not adjusted for in analyses. Figures 2-3 illustrate the overall risk of bias assessments, with the rationale for each judgment detailed in Appendix 3.
Risk of bias of the included randomized controlled trials
Risk of bias of the included non-randomized controlled trials
Effects of Interventions
Table 3 presents a summary of the main findings. A key consideration when interpreting results is the variation in methodological approaches across studies. The included studies employed different summary metrics; the majority presented means [9,12,26-33,35,36] (suitable for normally distributed data) while two studies reported medians (more robust for skewed distributions, potentially reflecting non-normal data or an intent to assess peak pain intensity and the peak impact on quality of life) [7,29]. This methodological difference should be considered when interpreting the results.
Pain evaluation: Regarding pain assessment, 9 of the 14 studies evaluated pain associated with fixed orthodontic treatment using the VAS [9,27-34]. The highest pain levels were consistently observed at the 24-hour mark. High values were reported across multiple studies, including 55.3 [28] and 50 ± 27 [31]. Tunca et al. reported a median pain score of 56.7 [29]. Other studies recorded initial mean values ranging from 26.35 ± 25.92 to 45 ± 22 [27,30,33,34]. Sirri et al. reported the lowest initial pain level, with a mean of 19.54 ± 7.76 [9].
A significant reduction in pain occurred after one week. A meta-analysis of two studies confirmed this observation (since they were the only ones reporting mean VAS scores with standard deviations at both the 24-hour and one-week time points), showing that pain was significantly higher on the first day compared to after one week (MD = 20.83; 95% CI: 11.7, 29.97; p < 0.00001; I² = 67%; Figure 4) [9,27]. It was not feasible to perform a sensitivity or subgroup analysis, since only two studies were included. This trend was supported by other studies, in which pain scores decreased to 13 ± 16 [31], 16.49 ± 13.87 [30], and 17 ± 13.3 [33]. Three studies confirmed a continued decrease at the two-week mark, with values of 13.3 [29], 9 ± 10.4 [33], and a notably low value of 0.07 ± 0.27 in Sirri et al.'s study [9]. Long-term assessment showed variable patterns. Wu et al. reported mean pain values of 32.3 ± 8 at one month, decreasing to 9.7 ± 3.5 by three months [32]. In Alcón et al.'s study, they did not measure pain at a single endpoint for each month; instead, they calculated an overall mean from all measurements taken throughout the first month (21.75 ± 1.98), and similarly for the third month (6.42 ± 10.09) [30].
Forest plot showing the difference in pain intensity between the first day and the first week
OHRQoLevaluation: Regarding assessment of oral health-related quality of life (OHRQoL), 9 of the 14 studies evaluated OHRQoL [7,12,26,27,29,31,33,35,36]. In eight of the nine studies, the Oral Health Impact Profile-14 (OHIP-14) was used [7,12,26,27,29,31,33,36], while one study used the Geriatric Oral Health Assessment Index (GOHAI) [35]. The assessment of OHRQoL across the included studies showed a consistent trend of initial impairment, followed by significant improvement over time.
The timing of the initial assessment influenced the baseline scores. Two studies measuring OHRQoL after one day of treatment reported scores of 16.0 ± 12.6 and 18.73 ± 7.75 [29,33]. In contrast, studies that conducted their first post-treatment evaluation at the one-week mark reported notably higher scores, indicating greater initial impairment, with values of 22.88 ± 9.60 [12] and 25.18 ± 4.15 [26]. It is important to note that these studies [12,26] established a pre-treatment baseline (T0) before reporting these one-week values. Another study also established a pre-treatment baseline, with its first post-treatment assessment conducted at the two-week mark, reporting a median score of 19.94 [7]. By the two-week point, three studies demonstrated substantial improvement, with scores ranging from 8.5 ± 8.9 to 16.41 ± 9.27 [12,29,33].
The conducted meta-analysis of two studies confirmed this pattern of recovery (as they were the only ones that provided mean OHIP-14 scores with standard deviations at both the one-week and one-month assessments), showing that OHRQoL was significantly better at one month than at one week. The pooled estimate showed that quality of life after one month was significantly better by 9.50 compared to one week, and the heterogeneity was low (MD = 9.50; 95% CI: 7.50, 11.50; p ˂ 0.00001; X² = 0.06; p = 0.80; I² = 0%; Figure 5) [12,26]. Given the zero heterogeneity, there was no need for further analyses. Data from four of the nine studies at the one-month mark revealed a notable divergence in scores. Curto et al.'s study reported a mean of 11.93 ± 2.19 [36], Alhafi et al. reported a median of 16.22 [7], while the other two reported markedly lower scores of 3.8 ± 2.1 [31] and 3.0 ± 1.9 [27]. Alfawal et al. reported a three-month OHRQoL score of 11.46 ± 2.63 [26]. The study by Miller et al., which used the GOHAI scale, confirms the same trend, showing an improvement in quality of life during the first week of treatment (59 ± 10.39) compared to the first day (38 ± 23.38) (in this scale, the highest values indicate better quality of life) [35].
Forest plot showing the difference in oral health quality of life between the first week and the first month
Certainty of the Evidence (GRADE)
The overall certainty of the evidence for the primary outcomes was assessed using the GRADE approach (Table 4). For the outcome of pain intensity, the quality of evidence was rated as very low, downgraded due to serious risk of bias, serious inconsistency (substantial heterogeneity across studies), and serious imprecision (small sample sizes and wide confidence intervals). For the outcome of OHRQoL, the quality of evidence was generally rated as low to very low. The comparison between OHRQoL at one week versus one month had a low certainty level, downgraded for risk of bias and imprecision, but not for inconsistency.
Discussion
This systematic review provides a focused analysis of pain and OHRQoL, specifically in adult patients undergoing fixed orthodontic treatment. While previous reviews have often examined mixed-age populations or compared appliance types [2,5,16,17], our findings offer a distinct perspective by concentrating on the adult demographic, whose pain perception and psychosocial responses may differ notably from those of younger patients.
The results showed a predictable adaptation pattern, characterized by an initial peak in pain at 24 hours, followed by a significant decline within the first week, and a parallel improvement in OHRQoL by the one-month mark. The improvement in OHRQoL reflects a complex interplay beyond pain adaptation. While the meta-analysis confirmed a statistical association between pain reduction and improvement in OHRQoL, the mechanisms underlying this improvement in quality of life extend beyond pain adaptation alone and were not consistently explored in the included studies. The recovery in OHRQoL may be attributed to patients' psychological adaptation to the appliance and their growing acceptance of the treatment process over time.
However, these findings should be interpreted with caution, as substantial heterogeneity was observed in the methodology of the included studies. A primary source of complexity arose from notable differences in the timing of initial outcome assessments across the studies. Notably, the timing of the initial outcome assessment varied considerably between and within the pain and OHRQoL measures. For pain, the first evaluation was conducted at different points after appliance placement: within the first few hours [27-29,31,34], at 24 hours [9,33], or after one week [32]. In contrast, the initial assessment of OHRQoL was even more heterogeneous. While some studies reported the first absolute values after one day [29,33] or one week [35], others established a pre-treatment baseline (T0), making their first post-treatment scores at one week [12,26] or two weeks [7] measures of change.
This fundamental discrepancy in baseline definition and assessment timing complicates the comparison of absolute scores across studies and likely contributed to the observed heterogeneity in reported values. Furthermore, a notable divergence in reported pain levels was observed even at similar time points. It can be attributed not only to assessment timing but also to other clinical and methodological factors. For example, the study by Sirri et al. reported notably lower pain scores across all evaluation periods compared to other studies, which could be influenced by specific patient demographics, the type of adjunctive procedure used (corticision), or inherent differences in pain perception thresholds within the sample [9]. This inter-study variability highlights that, while the overall pattern of pain resolution is consistent, pain magnitude is context-dependent and should not be generalized without considering these modifying factors.
Another point to discuss is the variation in summary metrics across the included studies. The majority presented means and standard deviations, suitable for normally distributed data. However, some studies reported medians [7,29], a practice often indicative of skewed data distributions, which is common for subjective outcomes like pain intensity that may not follow a normal curve. The use of medians in such cases is more robust for representing central tendency, but it poses a challenge for meta-analysis, which typically relies on means and standard deviations to pool data. This inconsistency limited the number of studies that could be included in our quantitative synthesis. The combination of these factors - variable assessment timing, divergent absolute scores, and the use of different or incomplete summary statistics - undoubtedly influenced the overall results of the review, leading to observed heterogeneity and limiting the precision of the pooled estimates.
In terms of the clinical significance of the findings, the statistically significant reduction in pain (a mean difference of over 20 VAS points from day 1 to week 1) and the improvement in OHRQoL (a mean difference of 9.5 OHIP-14 points out of the overall 54 points) are substantial enough to be considered clinically significant, representing a clear transition from high discomfort to a more acceptable state. However, the overall confidence in these findings is tempered by the methodological limitations discussed, which are reflected in the “low” to “very low” GRADE ratings. The risk of bias, particularly concerning self-reported outcomes in often unblinded studies, further underscores the need for cautious interpretation.
Limitations of the current work
This review has several limitations to consider, primarily the high risk of bias in several studies. The limited number of studies included in the meta-analysis was due to variability in assessment timing and statistical reporting. The reliance on self-reported outcomes, combined with the inability to blind participants, raises concerns regarding measurement bias. Furthermore, the inconsistent use of summary metrics limited the robustness and generalizability of the findings. These limitations, alongside generally small sample sizes and unaccounted-for demographic variables, underscore the need for cautious interpretation of the results.
Conclusions
Based on very low- to low-certainty evidence, this review suggests a consistent pattern of pain peaking at 24 hours and subsiding within the first week, alongside the parallel improvements in quality of life in adult patients undergoing conventional fixed orthodontic therapy. Clinicians may use these findings cautiously to reassure adult patients that initial discomfort is normal and temporary. Recommendations should be tempered due to the limited strength of the supporting evidence.
The very low- to low-certainty evidence raises the need for more studies. Future research should prioritize standardized methodology, including consistent timing of outcome assessments and reporting of summary data, to enable more reliable meta-analyses. Investigating long-term outcomes and the impact of specific demographic and clinical factors through well-designed longitudinal studies is essential to generate higher-certainty evidence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Contemporary Orthodontics Proffit W Fields H Sarver D St Louis Mosby 2007 https://books.google.com/books?hl=en&lr=&id=1UJ Mr CGU Ki 0C&oi=fnd&pg=PT 10&dq=Contemporary+Orthodontics&ots=GI 9Li OAYYN&sig=Sz S 48HTJNQA 8bdupjd QL 9Nihl Us#v=onepage&q=Contemporary%20Orthodontics&f=false
- 2Treatment outcome with orthodontic aligners and fixed appliances: a systematic review with meta-analyses Eur J Orthod Papageorgiou SN Koletsi D Iliadi A Peltomaki T Eliades T 3313434220203175819110.1093/ejo/cjz 094 · doi ↗ · pubmed ↗
- 3The Kyoto protocol of IASP basic pain terminology Pain Loeser JD Treede RD 47347713720081858304810.1016/j.pain.2008.04.025 · doi ↗ · pubmed ↗
- 4Satisfaction with orthodontic treatment outcome Angle Orthod Feldmann I 5815878420142442320210.2319/093013-710.1PMC 8650456 · doi ↗ · pubmed ↗
- 5Pain profile during orthodontic levelling and alignment with fixed appliances reported in randomized trials: a systematic review with meta-analyses Clin Oral Investig Inauen DS Papadopoulou AK Eliades T Papageorgiou SN 1851186827202310.1007/s 00784-023-04931-5PMC 1015994936879148 · doi ↗ · pubmed ↗
- 6Evaluation of pain and discomfort associated with orthodontic adjustments J Pharm Bioallied Sci Mohanty B Chekka M Sowmya C Khurana R Manga UM Varma Datla PK Somaraj V 0216202410.4103/jpbs.jpbs_269_24PMC 1142663139346332 · doi ↗ · pubmed ↗
- 7The impact of non-extraction orthodontic treatment on the oral-health-related quality of life between a modified aligner appliance with Ni-Ti springs and the traditional fixed appliances: a randomized controlled clinical trial Medicina (Kaunas) Alhafi ZM Hajeer MY Latifeh Y 11396020243906456810.3390/medicina 60071139 PMC 11279390 · doi ↗ · pubmed ↗
- 8Evaluation of the levels of pain, discomfort, functional impairments and satisfaction with the periodontally accelerated osteogenic orthodontics (PAOO) when leveling and aligning crowded teeth: a prospective cohort study Cureus Alsino HI Hajeer MY Alkhouri I Murad RM Khattab TZ 014202210.7759/cureus.22623 PMC 888193535233336 · doi ↗ · pubmed ↗