High levels of unfavourable treatment outcomes in children with drug-sensitive TB in Sierra Leone
N. Sesay, I.F. Kamara, A.M.V. Kumar, P. Thekkur, A.A. Alwani, B.D. Fofanah, A.R.Y. Kamara, A. Bah, L. Farma-Grant, M.A. Sesay, W.K. Lahai, J.A. Koroma, S.M. Tengbe, F. Kanu, G. Ameh, S.M. Kanneh, R. Zachariah, M. Mahmoud

TL;DR
This study finds that most children with drug-sensitive TB in Sierra Leone have poor treatment outcomes despite following guidelines.
Contribution
The study is the first from Sierra Leone to evaluate treatment outcomes in children with drug-sensitive TB.
Findings
Only 32% of children achieved favorable treatment outcomes for drug-sensitive TB.
HIV co-infection and extra-pulmonary TB were significantly associated with unfavourable outcomes.
Children treated in 2023 and 2024 had better outcomes compared to those treated in 2022.
Abstract
Ola During Children’s Hospital, a tertiary-level paediatric facility affiliated with a university and located in Freetown, Sierra Leone. No published studies from Sierra Leone have evaluated treatment outcomes in children (<15 years) with drug-sensitive TB (DS-TB). To assess compliance with national TB treatment guidelines and evaluate treatment outcomes among children with DS-TB. A non-concurrent cohort study, utilising routinely collected secondary patient data from TB treatment master cards. Poisson regression was done to calculate adjusted relative risks (aRR). Of 689 children, 95% received treatment regimens compliant with national guidelines. However, only 32% achieved favourable outcomes, while 68% had unfavourable outcomes (7% death, 30% loss to follow-up, 31% not evaluated). HIV co-infection (aRR = 1.2) and HIV-unknown status (aRR = 1.5), residence outside urban areas (aRR =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE
FIGURE| Characteristics | n (%) |
|---|---|
| Age (in years) | |
| 0–4 | 548 (79.5) |
| 5–9 | 95 (13.8) |
| 10–14 | 46 (6.7) |
| Gender | |
| Men | 372 (54.0) |
| Women | 317 (46.0) |
| Year of treatment initiation | |
| 2022 | 311 (45.1) |
| 2023 | 277 (40.2) |
| 2024 | 101 (14.7) |
| Residence | |
| Western Area Urban | 440 (63.9) |
| Western Area Rural | 221 (32.1) |
| Other provinces | 28 (4.0) |
| TB type | |
| Pulmonary TB | 559 (81.1) |
| Extra-pulmonary TB | 79 (11.5) |
| Not recorded | 51 (7.4) |
| Site of EPTB ( | |
| Lymph node | 34 (43.0) |
| Abdomen | 1 (1.3) |
| Meningitis | 37 (46.8) |
| Osteoarticular | 6 (7.6) |
| Pericardial | 1 (1.3) |
| Type of TB diagnosed | |
| Bacteriologically confirmed | 190 (27.6) |
| Clinically diagnosed | 483 (70.1) |
| Not recorded | 16 (2.3) |
| Patient type | |
| New | 565 (82.0) |
| Previously treated | 32 (4.6) |
| Not recorded | 92 (13.4) |
| HIV status | |
| Positive | 206 (29.9) |
| Negative | 447 (64.9) |
| Unknown | 1 (0.1) |
| Not recorded | 35 (5.1) |
| ART status ( | |
| On ART | 47 (22.8) |
| Not on ART | 2 (1.0) |
| Not recorded | 157 (76.2) |
| Treatment guideline | |
| Compliant | 652 (94.6) |
| Non-compliant | 37 (5.4) |
| Treatment outcome | |
| Treatment completed | 213 (30.9) |
| Cured | 9 (1.3) |
| Death | 48 (7.0) |
| Lost to follow-up | 206 (29.9) |
| Not evaluated | 213 (30.9) |
| Outcome | Number | Proportion (including ‘not evaluated’) | Proportion (excluding ‘not evaluated’) |
|---|---|---|---|
| Total | 689 | ||
| Treatment success | 222 | 32.2 | 46.6 |
| Cured | 9 | 1.3 | 1.9 |
| Treatment completed | 213 | 30.9 | 44.7 |
| Unfavourable outcomes | 467 | 67.8 | 53.4 |
| Death | 48 | 7.0 | 10.1 |
| Loss to follow-up | 206 | 29.9 | 43.3 |
| Not evaluated | 213 | 30.9 | NA |
| Characteristics | Total | Unsuccessful outcomes | RR (95% CI) | aRR (95% CI) |
|---|---|---|---|---|
| Total, | 689 | 467 (67.8) | ||
| Age (in years) | ||||
| 0–4 | 548 | 379 (69.2) | Ref | Ref |
| 5–9 | 95 | 53 (65.4) | 0.9 (0.8–1.1) | 1.0 (0.8–1.1) |
| 10–14 | 46 | 35 (58.3) | 0.9 (0.7–1.1) | 1.0 (0.8–1.2) |
| Gender | ||||
| Men | 372 | 248 (66.7) | Ref | Ref |
| Women | 317 | 219 (69.1) | 1.0 (0.9–1.1) | 1.0 (0.9–1.1) |
| Year of treatment initiation | ||||
| 2022 | 311 | 262 (82.2) | Ref | Ref |
| 2023 | 277 | 157 (56.7) | 0.7 (0.6–0.8) | 0.7 (0.6–0.7) |
| 2024 | 101 | 48 (47.5) | 0.6 (0.5–0.7) | 0.6 (0.5–0.7) |
| Residence | ||||
| Western Area Urban | 440 | 281 (63.9) | Ref | Ref |
| Western Area Rural | 221 | 160 (72.4) | 1.1 (1.0–1.3) | 1.1 (1.0–1.2) |
| Other | 28 | 26 (92.9) | 1.5 (1.3–1.6) | 1.3 (1.1–1.5) |
| Site of TB infection | ||||
| Pulmonary TB | 559 | 372 (66.5) | Ref | Ref |
| Extra-pulmonary TB | 79 | 61 (77.2) | 1.2 (1.0–1.3) | 1.2 (1.0–1.3) |
| Not recorded | 51 | 34 (66.7) | 1.0 (0.8–1.2) | 1.0 (0.9–1.3) |
| Type of TB diagnosed | ||||
| Bacteriologically confirmed | 190 | 131 (68.9) | Ref | Ref |
| Clinically diagnosed | 483 | 324 (67.1) | 1.0 (0.9–1.1) | 1.0 (0.9–1.1) |
| Not recorded | 16 | 12 (75.0) | 1.1 (0.8–1.5) | 0.9 (0.7–1.2) |
| Patient type | ||||
| New | 565 | 378 (66.9) | Ref | Ref |
| Previously treated | 32 | 22 (64.8) | 1.1 (0.3–4.6) | 1.2 (0.3–4.7) |
| Not recorded | 92 | 67 (72.8) | 0.8 (0.3–2.2) | 0.7 (5–2.9) |
| HIV status | ||||
| Positive | 206 | 151 (73.3) | 1.2 (1.0–1.3) | 1.2 (1.0–1.3) |
| Negative | 447 | 280 (62.6) | Ref | Ref |
| Unknown | 36 | 36 (100.0) | 1.6 (1.5–1.7) | 1.5 (1.4–1.7) |
| Compliance to IP prescription | ||||
| Yes | 635 | 434 (68.3) | Ref | Ref |
| No | 54 | 33 (61.0) | 0.9 (0.7–1.1) | 0.9 (0.7–1.1) |
- —Structured Operational Research and Training Initiative (SORT IT)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Pneumocystis jirovecii pneumonia detection and treatment · Infectious Diseases and Tuberculosis
TB is a preventable and curable disease; yet, it is the world’s leading cause of death from a single infectious agent.^1^ In children, especially those under the age of 5 years, TB is often underdiagnosed due to atypical presentations of the disease, placing them at higher risk of severe disease and unfavourable treatment outcomes.^2,3^ In low- and middle-income countries, additional drivers of the TB epidemic in children include poverty, malnutrition, HIV co-infection, and a high prevalence of TB among adults.^2,4,5^ Sub-Saharan Africa (SSA) carries a disproportionate TB burden, with an estimated 800,000 children affected annually.^6,7^ In Sierra Leone, an estimated 24,000 people contract TB yearly, and it is the sixth leading cause of death, with an estimated 1,770 annual fatalities – a case fatality ratio of 7.4%. Approximately 1,536 children under 15 years with TB are reported annually, accounting for 7% of all cases notified in 2023.^1^ However, this figure is likely to be an underestimate due to diagnostic challenges and weaknesses in the monitoring and evaluation system in health facilities.^8,9^
The most recent WHO TB report revealed a global treatment success of 88% for new drug-sensitive TB (DS-TB) cases treated with first-line drugs.^1^ However, this figure is lower in SSA with 79% treatment success.^7^ More alarming is that treatment success among children is lowest in Africa at 70%.^7,10^ Sierra Leone’s National Tuberculosis Control Program aims to increase the early detection of paediatric TB and increase the treatment success.^9^ However, there has been no formal analysis of treatment outcomes in children under 15 years of age. Ensuring high TB treatment success in children requires high compliance with recommended treatment regimens and addressing factors linked to unsuccessful outcomes. Achieving this goal necessitates surveillance and operational research.^11–13^ A review of existing literature revealed that studies focused on treatment outcomes in adults and in those with drug-resistant TB.^9,14–16^ However, there is a lack of studies focused on children. To bridge this gap, we assessed i) compliance with national TB treatment guidelines and ii) treatment outcomes in a cohort of children with DS-TB initiated on treatment from January 2022 to June 2024 at one of the largest paediatric referral centres in Sierra Leone.
Insights from this study can inform improvements in clinical practice, strengthen health system capacity, and guide strategies aimed at addressing unfavourable outcomes, such as mortality, treatment failure, and loss to follow-up.^16,17^
METHODS
This was a non-concurrent cohort study utilising routinely collected, secondary data in TB treatment cards.
Study setting
Sierra Leone, a low-income country located on the Atlantic coast of West Africa between Guinea and Liberia, has a population of over 8 million people, with children (<15 years) accounting for 41% of the total.^17^ The capital, Freetown, hosts the majority of the country’s tertiary and specialised health care facilities, including paediatric care. The study was conducted at Ola During Children’s Hospital (ODCH), Sierra Leone’s oldest paediatric facility and part of the University of Sierra Leone Teaching Hospital complex. It provides free comprehensive paediatric, HIV, and DS-TB care, serving predominantly the Western Area while referring drug-resistant TB cases to specialised centres.
TB programme framework at ODCH
TB diagnosis involves a combination of clinical assessment based on medical history and physical examination, chest radiography, and laboratory tests such as sputum smear microscopy for acid-fast bacilli, Xpert MTB/RIF/ultra, and culture. Clinically diagnosed TB includes both cases confirmed through clinical assessment alone and those supported by radiological evaluation. Chest X-ray findings were extracted when available; however, they were not consistently recorded for all patients. Children diagnosed with DS-TB receive a 2-month intensive phase (IP) treatment. Severely ill patients are admitted for directly observed therapy, followed by a caregiver-administered continuation phase (CT) at home under caregiver supervision, with periodic hospital visits for medication collection.
HIV and antiretroviral therapy (ART) status were extracted retrospectively from routine TB treatment records, specifically the patient TB treatment cards, which served as the sole data source. Missing or undocumented ART information was classified as ‘not recorded’ and analysed as not on ART.
Standardised TB treatment regimens for children are tailored by disease site and weight band.^18^ Children under 15 years and weighing under 25 kg with pulmonary or extra-pulmonary TB (EPTB) (excluding TB meningitis, miliary TB, and osteoarticular TB) receive a 2-month IP of rifampicin/isoniazid/pyrazinamide/ethambutol (RHZE – 75/50/150/100 mg), followed by a 4-month CP of rifampicin/isoniazid (RH – 75/50 mg). For children with TB meningitis, miliary TB, or osteoarticular TB, the CP extends to 10 months. The number of fixed-dose combination (FDC) tablets administered daily ranges from one to four, depending on the child’s weight (4–7, 8–11, 12–15, 16–24 kg). Children less than 4 kg receive half a tablet. Children weighing 25 kg and above receive adult dosing: those between 25 and 39 kg receive two tablets and those between 40 and 54 kg receive three tablets of RHZE (150/75/400/275 mg) in the IP and rifampicin/isoniazid (150/75 mg) in the CP, respectively.
Study population
Children (<15 years) with DS-TB, who were initiated on first-line treatment at ODCH between 1 January 2022 and 30 June 2024, were included.
Data collection
Data were collected by trained health care professionals experienced in patient chart review. To ensure uniformity, all data collectors underwent standardised training on the data collection tool, the use of Epicollect5, and how to collect the data from treatment cards. The data were collected from 1 March to 30 April 2025. The principal investigator provided overall supervision and conducted routine cross-checks to ensure data accuracy, without disrupting clinical services.
Statistical analysis
Data from Epicollect5 were exported and analysed using Stata 16.1 (StataCorp LLC, College Station, TX, USA). Demographic and clinical characteristics of the study participants, non-compliance with treatment regimens, and treatment outcomes were summarised using frequencies and proportions. Patients were classified into favourable (cured and treatment completed) and unfavourable outcome (treatment failure, death, loss to follow-up, and not evaluated) groups following national and WHO guidelines.^18,19^ Compliance with the three recommended paediatric regimens for DS-TB was assessed by evaluating whether the prescribed regimen and duration matched with the TB type and whether the dosage (based on tablet count) was appropriate for the child’s weight. To identify factors associated with unfavourable treatment outcomes, both unadjusted and adjusted generalised linear models (Poisson regression) were employed. Adjusted relative risks (aRRs) with 95% confidence intervals (CIs) were calculated to quantify the associations.
Ethical statement
Ethics approval was granted by the Sierra Leone Ethics and Scientific Review Committee (SLESRC – 026/02/2025). Hospital management authorised data access, and informed consent was waived as the study involved only secondary data review.
RESULTS
There were 689 children with DS-TB during the study period (Table 1). The majority (548, 79.5%) were under the age of five. More than half (372, 54%) were males. Most children (440, 63.9%) lived in urban areas. Pulmonary TB was predominant (81%), while EPTB accounted for 11.5% of children. Among EPTB cases (n = 79), TB meningitis (37, 46.7%) and TB lymphadenitis (34, 43%) were most common. Nearly one third (206, 29.9%) of the children were HIV-positive, and among them, only 22.8% were on ART.
Treatment guidelines compliance
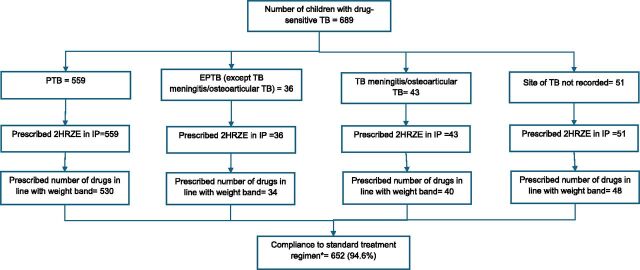
Compliance with treatment guidelines was high, with 652 (94.6%) compliant with intensive-phase prescriptions (Figure). Non-compliance was primarily due to prescription of incorrect doses – 5 children had underdosing (one FDC tablet less than that recommended per day) and 32 children had overdosing (one FDC tablet more than that recommended per day).
*Compliance to treatment guidelines among children with drug-sensitive TB initiated on treatment at Ola During Children’s Hospital, Sierra Leone, from January 2022 to June 2024. PTB and EPTB patients prescribed 2HRZE in the intensive phase with the number of drugs per day in line with the weight bands. HRZE = isoniazid/rifampicin/pyrazinamide/ethambutol; IP = intensive phase; PTB = pulmonary TB; EPTB = extra-pulmonary TB.
Treatment outcomes and factors associated with unfavourable outcomes
Of the 689 children, 222 (32.2%) had favourable outcomes (cured 1.3%; treatment completed 30.9%) and 467 (67.8%) had unfavourable outcomes (death 7%; loss to follow-up 29.9%; and not evaluated 30.9%) (Table 1). Treatment success was 46.6% after excluding patients classified as ‘not evaluated’ (Table 2). Mortality was notably high in children with TB meningitis (15/37, 40.5%). Children treated in 2023 (aRR = 0.7, 95% CI: 0.6–0.7) and 2024 (aRR = 0.6, 95% CI: 0.5–0.7) had a significantly lower risk of unfavourable treatment outcomes compared to those treated in 2022 (Table 3). Children residing in provincial areas had a significantly higher likelihood of unfavourable outcomes compared with those from Western Area Urban (aRR = 1.3, 95% CI: 1.1–1.5). HIV-positive children had a higher risk of unfavourable outcomes compared to HIV-negative children (aRR = 1.2, 95% CI: 1.0–1.3). Children with an unknown HIV status had the highest risk, with all cases (100%) classified as having unfavourable outcomes (aRR = 1.5, 95% CI: 1.4–1.7). EPTB was associated with higher risk (aRR = 1.2, 95% CI: 1.0–1.3) compared to pulmonary TB.
DISCUSSION
This is the first study from Sierra Leone presenting a comprehensive analysis of treatment outcomes among children with DS-TB over a 30-month period. We found a high proportion of unfavourable outcomes (67.8%), which are among the highest reported globally, despite high compliance with national treatment guidelines. Excluding ‘not evaluated’ cases, treatment success was only 46.6%. The outcomes were worse in certain subgroups, such as children with HIV co-infection, those with EPTB, and those residing outside the urban areas. This highlights critical gaps in paediatric TB care and health system performance.
One of the most striking findings is the disconnect between high compliance with treatment guidelines (94.6%) and unfavourable treatment outcomes. This suggests that adherence to standardised regimens alone is insufficient to ensure successful treatment in paediatric populations. While correct dosing and regimen selection are foundational, they must be complemented by robust systems for follow-up, treatment support, and management of comorbidities such as HIV. The high loss to follow-up (29.9%) and not evaluated cases (30.9%) point to systemic weaknesses in continuity of care, particularly during the CT when treatment is administered by the caregiver at home. This also reflects a lack of capacity and resources at ODCH for active follow-up of children and weaknesses in systematic transfer out of children to referral centres and related documentation. In contrast, in a large study from Ethiopia of children with DS-TB, the treatment success rate was 92.2% and death was 2.8%; loss to follow-up was only about 1.1%, and about 0.4% of all children were not evaluated.^20^ This may be due to differences in geographical coverage, patient characteristics, socio-economic conditions, and programme capacities.
HIV co-infection was a significant predictor of unfavourable outcomes, with only 22.8% of HIV-positive children documented as receiving ART despite national guidelines recommendation. Incomplete HIV/ART documentation reflects weak TB-HIV integration, leading to missed opportunities for universal testing, timely ART initiation, and coordinated care. The 100% unfavourable outcomes among children with unknown HIV status underscore the critical importance of universal HIV testing and accurate documentation. These findings align with previous studies that have demonstrated the detrimental impact of HIV on TB treatment outcomes.^21–23^
Extra-pulmonary TB, particularly TB meningitis, was associated with the highest mortality and poorest outcomes, consistent with global evidence that severe paediatric TB forms have substantially lower treatment success than pulmonary TB. A study in Mozambique showed EPTB was associated with worse outcomes, and HIV-positive status further worsened the outcome.^24^ The fact that ODCH is a referral centre seeing more severe TB cases may explain the disproportionate representation of TB meningitis and EPTB, as well as the elevated mortality outcomes.
Children residing outside Western Area Urban had significantly higher risks of unfavourable outcomes. This disparity likely reflects inequities in access to health care, transportation barriers, and socio-economic challenges faced by families in rural and remote areas. While ODCH serves as a national referral centre, the burden of travel and follow-up may be prohibitive for families from distant regions.
Encouragingly, treatment outcomes improved over time, with children treated in 2023 and 2024 showing significantly lower risks of unfavourable outcomes compared to those treated in 2022. These improved treatment outcomes may reflect strengthened programmatic practices, including staff training on documentation by the TB programme, introduction of a more user-friendly treatment register, and enhanced monitoring and evaluation. Although the exact cause is uncertain, these improvements likely supported better data completeness, guideline adherence, and patient management. Another commendable finding is the high compliance with treatment guidelines, with nearly all children being treatment compliant at the start of treatment. A limitation of this assessment, however, is that we could not assess the compliance as the treatment progressed, as changes in weight and doses were not documented in the treatment cards.
Our study has several strengths. It is one of the first to systematically assess paediatric DS-TB treatment outcomes in Sierra Leone, addressing a critical gap in the literature. The large sample size and use of standardised data collection tools enhanced the reliability of findings. The use of adjusted Poisson regression models provided robust estimates of associations between clinical and demographic factors and treatment outcomes. We reported the study findings in line with STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.^25^ There were also some limitations. First, we relied on routinely collected secondary data, which may be subject to documentation errors and missing information. The high proportion of ‘not evaluated’ outcomes and unrecorded variables (e.g., ART status) reflects these challenges. Second, the study was conducted at a single tertiary hospital, which may limit generalisability nation-wide. Third, we did not collect data on nutritional status and other comorbidities, which may influence outcomes. Finally, the absence of a qualitative component limited the exploration of underlying reasons for the unfavourable treatment outcomes.
Despite these limitations, the findings of this study highlight several areas for targeted intervention:
- i)Strengthening the monitoring of the CT of treatment: Potential strategies include systematically documenting transfer-outs, recording caregiver contact information, conducting follow-up calls after 15 days, and allocating dedicated staff for patient follow-up.
- ii)Integration of TB-HIV services: Ensuring that all patients with TB are tested for HIV, and if HIV-positive, children are promptly initiated on ART and monitored closely. Co-location of TB and HIV services, joint training of staff, and shared data systems could facilitate integration.
- iii)Decentralisation and outreach: Expanding paediatric TB services to peripheral health facilities and enhancing outreach to primary care units and sharing patient information with peripheral facilities can improve care continuity and reduce geographic disparities in outcomes. Implementing a web-based or online TB register accessible to receiving facilities would facilitate real-time tracking, reduce loss to follow-up, and ensure timely monitoring.
- iv)Strengthening data recording: The high proportion of cases classified as ‘not evaluated’ points to weaknesses in data capture and reporting. Training staff in documentation and routine data audits could improve accountability and programme performance.
CONCLUSION
The study reveals alarmingly unfavourable outcomes among children with DS-TB in Sierra Leone, despite high compliance with national treatment guidelines. HIV co-infection, residence outside urban areas, and EPTB were significant predictors of unfavourable outcomes. These findings call for urgent programmatic action to strengthen follow-up systems, integrate TB-HIV care, decentralise services, and improve data quality. Addressing these gaps is essential to achieving the national goal of improved paediatric TB outcomes and contributing to the global End TB strategy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Global tuberculosis report 2024. Geneva: WHO, 2024.
- 2Glaziou P, Global epidemiology of tuberculosis. Semin Respir Crit Care Med. 2013;34(1):3-16.23460002 10.1055/s-0032-1333467 · doi ↗ · pubmed ↗
- 3Aketi L, Childhood tuberculosis in a Sub-Saharan tertiary facility: epidemiology and factors associated with treatment outcome. Mokrousov I. P Lo S One. 2016;11(4):e 0153914.27101146 10.1371/journal.pone.0153914 PMC 4839557 · doi ↗ · pubmed ↗
- 4Tilahun G, Gebre-Selassie S. Treatment outcomes of childhood tuberculosis in Addis Ababa: a five-year retrospective analysis. BMC Public Health. 2016;16(1):612.27443308 10.1186/s 12889-016-3193-8PMC 4957362 · doi ↗ · pubmed ↗
- 5Engelbrecht MC, Unsuccessful TB treatment outcomes with a focus on HIV co-infected cases: a cross-sectional retrospective record review in a high-burdened province of South Africa. BMC Health Serv Res. 2017;17(1):470.28693508 10.1186/s 12913-017-2406-x PMC 5504727 · doi ↗ · pubmed ↗
- 6Campbell SM, Meyer JC, Godman B. Why compliance to national prescribing guidelines is important especially across sub-Saharan Africa and suggestions for the future. J Biomed Pharm Sci. 2021;4:316.
- 7Bagcchi S. WHO’s global tuberculosis report 2022. Lancet Microbe. 2023;4(1):e 20.36521512 10.1016/S 2666-5247(22)00359-7 · doi ↗ · pubmed ↗
- 8Government of Sierra Leone. National leprosy and tuberculosis-strategic plan (2016-2020) core plan. Freetown, Sierra Leone: Ministry of Health, Government of Sierra Leone, 2016. https://portal.mohs.gov.sl/wp-content/uploads/2021/04/national-leprosy-and-tb-strategic-plan-2016-2020-final-draft.pdf.