Critical level of food insecurity and nonadherence to antiretroviral therapy among adults living with HIV
N.L. Mbiki, M.S. Dimfumu, B.E. Disuemi, G.M. Ngombua, S.B. Bindamba, K.T. Totokani, G.D. Nahimana, B.P. Mutombo

TL;DR
Severe food insecurity strongly predicts nonadherence to HIV treatment, highlighting the need for nutritional support in HIV care.
Contribution
Identifies a critical threshold of food insecurity that significantly impacts ART adherence among HIV patients.
Findings
Severe food insecurity was strongly associated with nonadherence (aOR = 5.98).
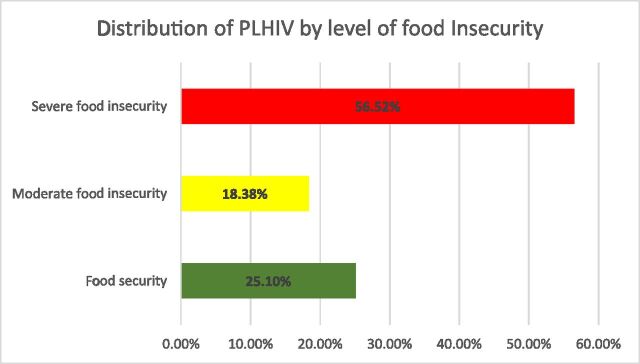
74.9% of participants were food insecure, with 56.5% experiencing severe food insecurity.
ART refill intervals of 3–6 months were protective against nonadherence (aOR = 0.42).
Abstract
Adherence to antiretroviral therapy (ART) is crucial for the clinical management of people living with HIV (PLHIV), but food insecurity can compromise it. The threshold at which food insecurity significantly affects adherence remains poorly studied. A cross-sectional study was conducted in health care facilities in Kinshasa among 506 PLHIV receiving outpatient ART. Socio-demographic, clinical, behavioural, and nutritional data were collected through structured interviews and medical record reviews. Chi-square tests and logistic regression analyses were performed using Stata version 17.0 software, with a statistical significance threshold set at P < 0.05. Proportion of ART nonadherence was 51.4%. Overall, 74.9% of participants were food insecure, including 56.5% with severe food insecurity. In multivariate analysis, severe food insecurity was strongly associated with nonadherence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE
FIGURE| Characteristics | Total ( | Adherence to ART | ||
|---|---|---|---|---|
| Yes | No | |||
| Gender | 0.001 | |||
| Men | 279 | 117 (47.6) | 162 (62.3) | |
| Women | 227 | 129 (52.4) | 98 (37.7) | |
| Marital status | 0.004 | |||
| Single | 277 | 133 (54.1) | 144 (55.4) | |
| Married | 133 | 78 (31.7) | 55 (21.2) | |
| Divorced and widowed | 96 | 35 (14.2) | 61 (23.5) | |
| Level of study | 0.016 | |||
| No | 29 | 8 (3.3) | 21 (8.1) | |
| Primary | 16 | 5 (2.0) | 11 (4.2) | |
| Secondary | 301 | 144 (58.5) | 157 (60.4) | |
| Superior | 160 | 89 (36.2) | 71 (27.1) | |
| Respondent’s main activity | <0.001 | |||
| Employee | 127 | 66 (26.8) | 61 (23.5) | |
| Self-employed | 134 | 42 (17.1) | 92 (35.4) | |
| Unemployed | 245 | 138 (56.1) | 107 (41.2) | |
| Household size | 0.025 | |||
| <5 | 162 | 67 (27.2) | 95 (36.5) | |
| ≥5 | 344 | 179 (72.8) | 165 (63.5) | |
| Appointment adherence | 0.004 | |||
| Yes | 448 | 228 (92.7) | 220 (84.6) | |
| No | 58 | 18 (7.3) | 40 (15.4) | |
| ART regimen | 0.009 | |||
| First-line | 196 | 96 (68.6) | 100 (54.4) | |
| Second-line | 128 | 44 (31.4) | 84 (45.6) | |
| Primary caregiver | 0.012 | |||
| Another person | 224 | 123 (54.9) | 101 (45.1) | |
| Self | 282 | 123 (43.6) | 159 (56.4) | |
| Variables | Frequency, | cOR (95% CI) |
|---|---|---|
| Food insecurity | 379 (74.8) | |
| Level of food insecurity | ||
| Food security | 127 (25.1) | r |
| Moderate | 93 (18.38) | 2.35 (1.28–4.32) |
| Severe | 286 (56.52) | 9.65 (5.82–15.99) |
| Characteristics | Total | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|---|
| cOR | 95% CI | aOR | 95% CI | ||
| Gender | |||||
| Men | 279 | r | |||
| Women | 227 | 0.55** | 0.38–0.78 | ||
| Age (years) median (IQR) 38 ± 19 | |||||
| 30–39 | 156 | r | |||
| <30 | 113 | 0.84 | 0.52–1.36 | ||
| 40–49 | 114 | 0.92 | 0.57–1.49 | ||
| 50–59 | 88 | 0.79 | 0.47–1.34 | ||
| ≥60 | 35 | 0.90 | 0.43–1.87 | ||
| Marital status | |||||
| Married | 133 | r | |||
| Single | 277 | 1.53* | 1.01–2.33 | 1.38 | 0.79–2.40 |
| Divorced and widowed | 96 | 2.47** | 1.44–4.24 | 2.18* | 1.10–4.35 |
| Level of study | |||||
| Superior | 160 | r | |||
| No | 29 | 3.29** | 1.38–7.87 | ||
| Primary | 16 | 2.75 | 0.92–8.30 | ||
| Secondary | 301 | 1.37 | 0.93–2.01 | ||
| Main activity | |||||
| Employee | 127 | r | |||
| Self-employed | 134 | 2.37** | 1.43–3.92 | ||
| Unemployed | 245 | 0.83 | 0.55–1.29 | ||
| Duration of ART provided | |||||
| <3 months | 209 | r | |||
| 3–6 months | 210 | 0.43*** | 0.29–063 | 0.42** | 0.25–0.69 |
| >6 months | 87 | 1.05 | 0.63–1.75 | 1.30 | 0.65–2.58 |
| Viral load test done | |||||
| Yes | 230 | r | |||
| No | 276 | 2.58*** | 1.80–3.69 | 1.63* | 1.03–2.58 |
| Alcohol consumption | |||||
| No | 239 | r | |||
| Yes | 267 | 3.45*** | 2.39–4.97 | 1.93* | 1.07–3.47 |
| Drug use | |||||
| No | 325 | r | |||
| Yes | 181 | 2.91*** | 1.98–4.26 | ||
| Travel outside Kinshasa | |||||
| No | 371 | r | |||
| Yes | 135 | 2.83*** | 1.86–4.30 | 3.52*** | 2.03–6.11 |
| Keeping your appointment | |||||
| No | r | ||||
| Yes | 2.30** | 1.28–4.14 | |||
| Support | |||||
| Third party | r | ||||
| Yourself | 1.57* | 1.11–2.24 | |||
| Level of food insecurity | |||||
| Food security | 127 | r | |||
| Moderate | 93 | 2.35** | 1.28–4.32 | 1.64 | 0.83–3.24 |
| Severe | 286 | 9.65*** | 5.82–15.99 | 5.98*** | 3.35–10.69 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · Food Security and Health in Diverse Populations · HIV-related health complications and treatments
HIV infection remains a major global public health concern. In 2023, an estimated 39.9 million people were living with HIV and 630,000 died from opportunistic infections, with sub-Saharan Africa accounting for approximately 3,100 new infections per day.^1^ In the Democratic Republic of the Congo (DRC), HIV prevalence is estimated at 1.0% in the general population and 0.4% in Kinshasa,^2^ representing more than 500,000 people living with HIV (PLHIV) nation-wide.^3^ Progress towards the UNAIDS 95-95-95 targets has been notable: by 2023, 87% of PLHIV knew their status, 98% of those diagnosed were on antiretroviral therapy (ART), and among the 46% who had viral load testing, 89% achieved suppression equivalent to an estimated 75.9% overall viral suppression.^1^ Viral suppression improves clinical outcomes and reduces sexual and perinatal transmission^4^ but relies heavily on sustained ART adherence.^5^ Adherence, defined as the degree to which patients follow prescribed regimens,^6^ is key to therapeutic success; poor adherence contributes to virologic failure, disease progression, and increased morbidity.^5,6^
Food insecurity is a well-established determinant of poor adherence. Defined as limited or uncertain access to sufficient, safe, and nutritious food,^7^ it affects health care access, quality of life,^8^ psychological well-being,^9^ hospitalisation rates, and mortality.^10^ Evidence shows a consistent association between food insecurity and ART nonadherence.^11^ However, most studies treat food insecurity as a binary exposure, neglecting potential gradient effects across mild, moderate, and severe categories.^12^ This simplification limits the ability to determine the severity threshold at which adherence begins to deteriorate. In the DRC, where food insecurity is widespread, PLHIV face heightened vulnerability, yet some maintain adequate adherence despite hardship. This suggests that nonadherence may emerge only beyond a certain severity level, underlining the relevance of exploring a dose–response relationship.^13^
This study therefore investigates the association between graded levels of food insecurity and ART adherence among PLHIV in Kinshasa. The findings aim to inform targeted nutritional and therapeutic interventions and support progress towards the national 95-95-95 goals.
METHODS
This cross-sectional analytical study was conducted from November 2024 to January 2025 among adults living with HIV attending outpatient services in six geographically distributed health care facilities in Kinshasa, Democratic Republic of the Congo. All centres provided free ART and none offered food or nutritional assistance during the study period.
Participants and recruitment
Eligible participants were adults (≥18 years) living with HIV, on ART for at least 6 months, and receiving routine follow-up in the selected facilities. Patients who were hospitalised or presented severe psychiatric or cognitive impairment were excluded. Consecutive recruitment was performed during routine visits after confirming eligibility and obtaining written informed consent.
Sampling and sample size justification
The sample size was calculated at 385 using a 95% confidence level and 5% margin of error, assuming 50% nonadherence. Accounting for a 10% nonresponse rate, the final target was 511 participants. A three-stage sampling strategy was employed: first, six high-volume facilities were selected; then, adults on ART for at least 6 months were identified; and finally, consecutive enrolment occurred.
Data collection tools and procedures
Data were collected through a structured questionnaire administered in French or Lingala and complemented by medical record review. The questionnaire, programmed in KoboCollect, included socio-demographic characteristics, food insecurity assessed using the Food Insecurity Experience Scale (FIES), adherence to ART using a composite indicator (Morisky Medication Adherence Scale [MMAS-8], AACTG, pharmacy refill, and clinical follow-up), and clinical variables (CD4 count, viral load, regimen, weight, appointment attendance).
The primary outcome
ART nonadherence was defined as nonadherence identified through any of three sources: pharmacy refill delays (≥1 day), missed doses reported during clinical follow-up, low self-reported adherence using the AACTG^14^ and the Morisky Medication Adherence Scale (MMAS-8).^15^
The main exposure
Food insecurity was categorised into food secure, mildly, moderately, or severely insecure based on the FIES.^16^ Covariates included socio-demographic characteristics, treatment duration, treatment line, reasons for missed doses, and appointment adherence.
Data quality control and management
Investigators were trained for 3 days, and the tool was pretested on 10% of the expected sample in non-study sites. Daily supervision ensured completeness and accuracy. Data were entered in EpiData 3.1 and analysed in Stata 17.
Statistical analysis
Descriptive statistics summarised participant characteristics. Chi-square tests explored factors associated with food insecurity. Variables with P < 0.05 in bivariate analyses were included in multivariate logistic regression. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were reported; significance was set at P < 0.05.
Ethical statement
Ethical approval was granted by the Ethics Committee of the School of Public Health, University of Kinshasa. Written informed consent was obtained from all participants.
RESULTS
In total, 506 of the 511 adult PLHIV screened met the inclusion criteria, and they were selected for this study. Participants had a median age of 38 years (interquartile range: 18–57), were mostly male (55.1%), single (54.7%), and had at least secondary education (91.1%). Most were unemployed (74.9%) and lived in households of five or more members (68.0%). Among the 272 participants with CD4 measurements, 24.6% had counts >500 cells/mm^3^ (Table 1).
Proportion and level of food insecurity associated with nonadherence to ART among PLHIV adults, 2024
Overall, 51.4% of participants were nonadherent to ART. Food insecurity was highly prevalent (74.9%), with 56.5% experiencing severe and 18.4% moderate insecurity; only 25.1% were food secure (Figure; Table 2). Both moderate (odds ratio [OR] = 2.35; 95% CI: 1.28–4.32) and severe food insecurity (OR = 9.65; 95% CI: 5.82–15.99) were significantly associated with increased odds of nonadherence.
Level of food insecurity associated with nonadherence to antiretroviral therapy.
Factors associated with nonadherence to ART among PLHIV
In univariate analysis, nonadherence was associated with several socio-demographic, behavioural, and treatment-related characteristics (Table 3). Lower odds of nonadherence were observed among women (OR = 0.55; 95% CI: 0.38–0.78) and among participants on ART for 3–6 months (OR = 0.43; 95% CI: 0.29–0.63). Higher odds were observed among single participants (OR = 1.53; 95% CI: 1.01–2.33) or divorced participants (OR = 2.47; 95% CI: 1.44–4.24), those without formal education (OR = 3.29; 95% CI: 1.38–7.87), self-employed individuals (OR = 2.37; 95% CI: 1.43–3.92), alcohol users (OR = 3.45; 95% CI: 2.39–4.97), drug users (OR = 2.91; 95% CI: 1.98–4.26), or those missing clinic appointments (OR = 2.30; 95% CI: 1.28–4.14), practicing self-management of ART (OR = 1.57; 95% CI: 1.11–2.24), or travelling outside Kinshasa (OR = 2.83; 95% CI: 1.86–4.30). Moderate and severe food insecurity were among the strongest predictors.
In multivariate analysis, severe food insecurity remained the strongest independent predictor of nonadherence (aOR = 5.98; 95% CI: 3.35–10.69; P < 0.001). Additional independent predictors included travel outside Kinshasa (aOR = 3.52; P < 0.001), widowed/divorced status (aOR = 2.18; P = 0.025), alcohol consumption (aOR = 1.93; P = 0.028), and absence of viral load monitoring (aOR = 1.63; P = 0.035). ART duration of 3–6 months remained protective (aOR = 0.42; P = 0.001).
DISCUSSION
This study examined the association between food insecurity and ART adherence and identified the severity level at which food insecurity significantly reduces adherence among PLHIV. More than half of the participants (51.38%) were nonadherent, a level that threatens progress towards the UNAIDS 95-95-95 targets, as poor adherence increases the risk of drug resistance and virologic failure.^5,17,18^ This prevalence is higher than that previously reported in the DRC (25%–30%),^19^ possibly due to differences in adherence measurement or the recent deterioration of socio-economic conditions in Kinshasa.
Food insecurity was highly prevalent (74.9%), with 56.52% experiencing severe food insecurity. This burden adversely affects immunity, mental health, and overall disease management, and is consistently linked to poor adherence in sub-Saharan Africa.^20^ Our findings therefore align with existing evidence showing that poverty and unstable access to food undermine HIV outcomes. After adjustment, severe food insecurity remained the strongest predictor of nonadherence. This gradient-based analysis represents a methodological improvement compared with binary classifications used in previous studies. Several mechanisms may explain this association: from biological, some ART regimens cause gastrointestinal or neurological side effects when taken without food,^21,22^ and nutritional recommendations supporting ART effectiveness may be unattainable in food-insecure settings.^23^ From psychosocial, chronic hunger increases stress, anxiety, and depression, which impair treatment consistency.^24^ From economic, limited financial resources may force patients to prioritise food over transport or medical costs, reducing continuity of care.^25^
In the DRC, where armed conflict, political instability, and food price inflation persist, PLHIV remain especially vulnerable.^26^ The magnitude of the association observed in our study exceeds that described in other regions, where severe food insecurity generally doubled the risk of nonadherence.^27^ This difference may reflect heightened economic vulnerability in Kinshasa or contextual barriers to stable access to care. Other determinants of nonadherence were also identified. Lack of viral load monitoring may signal irregular follow-up, depriving patients of reinforcing feedback when viral suppression is achieved. Alcohol consumption, a known barrier to adherence due to forgetfulness and reduced judgement,^28^ may additionally reflect underlying mental health concerns. Travel outside Kinshasa was associated with missed doses and disrupted follow-up, underscoring the need for extended refills and interprovincial ART coordination.^27^ Treatment duration between 3 and 6 months was protective, while refills exceeding 6 months increased nonadherence, possibly due to treatment fatigue or perceived recovery.^29,30^ Widowhood and divorce also emerged as vulnerability factors, consistent with findings from southern Africa.
This study provides the first quantification in the DRC of the critical food insecurity threshold affecting ART adherence. Strengths include methodological rigour, a validated FIES scale, a composite adherence metric, adjustment for key confounders, and a large multisite sample from both public and private facilities. However, generalisability may be limited outside Kinshasa. Limitations include its cross-sectional design, which limits causal inference, and self-reported adherence may be biased. Bias was mitigated through triangulation with clinic appointments and biological monitoring, trained interviewers, and a composite adherence measure combining subjective and objective indicators.
CONCLUSION
Severe food insecurity is strongly associated with ART nonadherence among PLHIV in Kinshasa. Identifying a critical threshold at which adherence declines highlights food access as a major barrier to HIV therapeutic success. These findings support Sustainable Development Goals 2 (Zero Hunger) and 3 (Good Health and Well-Being) and underscore the need for multisectoral strategies integrating nutritional support into HIV care, while informing future research aimed at comprehensive and patient-centred HIV management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1UNAIDS. Global HIV & AIDS statistics - 2024 fact sheet. Geneva, Switzerland: UNAIDS, 2024. https://www.unaids.org/en/resources/fact-sheet.
- 2Ministry of Planning and Monitoring of the Implementation of the Revolution of Modernity, Ministry of Public Health (MSP), ICF International. Demographic and health survey in the Democratic Republic of Congo 2023-2024. Rockville, MD, USA: MPSMRM, MSP, and ICF International, 2024.
- 3Ministry of Public Health National AIDS Control Program. Annual report of the national AIDS control program 2022. Kinshasa, Democratic Republic of the Congo: PNLS, 2022.
- 4World Health Organization. HIV/AIDS fact sheet. Geneva: WHO, 2024.
- 5Bangsberg DR, Kroetz DL, Deeks SG. Adherence-resistance relationships to combination HIV antiretroviral therapy. Curr HIV/AIDS Rep. 2007;4(2):65-72.17547827 10.1007/s 11904-007-0010-0 · doi ↗ · pubmed ↗
- 6World Health Organization. HIV drug resistance report 2017. Geneva: WHO, 2017.
- 7Food and Agriculture Organization of the United Nations, International Fund for Agricultural Development, UNICEF, World Food Programme, World Health Organization. The state of food security and nutrition in the world 2023. Rome, Italy: FAO, 2023.
- 8Singer AW, Weiser SD, Mc Coy SI. Does food insecurity undermine adherence to antiretroviral therapy? A systematic review. AIDS Behav. 2015;19(8):1510-1526.25096896 10.1007/s 10461-014-0873-1 · doi ↗ · pubmed ↗