Cognitive changes associated with chemotherapy in breast cancer: an assessment of social cognition and executive functions in Peruvian patients
Sandro Casavilca-Zambrano, Nilton Custodio, Ruddy Liendo-Picoaga, Juan José Contreras Mancilla, Jenny Katherine Bonifacio Mundaca, Rosa Montesinos, Laura Fejerman, Valentina Zavala, Stéphane Bertani, Jorge Honles, Tatiana Vidaurre

TL;DR
This study examines cognitive changes in Peruvian breast cancer patients undergoing chemotherapy, finding that a subset experiences measurable cognitive decline.
Contribution
The study provides evidence of chemotherapy-related cognitive impairment in a Peruvian population with high Amerindian ancestry.
Findings
21% of patients showed cognitive impairment based on the Facial Emotion Recognition test after chemotherapy.
Higher educational attainment was associated with better cognitive performance across all domains.
Culturally adaptable tools like the FER test are promising for cognitive screening in resource-limited oncology settings.
Abstract
Cognitive impairment related to chemotherapy—commonly referred to as “chemo brain”—is a well-documented phenomenon among breast cancer patients. These impairments affect memory, attention, executive function, and social cognition, yet remain understudied in low- and middle-income countries. In Peru, where populations present a high proportion of Amerindian ancestry and distinct sociocultural factors, evidence is scarce. We conducted a longitudinal study of 143 Peruvian women aged 28-64 years, newly diagnosed with early-stage breast cancer and naïve to chemotherapy, treated at the National Institute of Neoplastic Diseases (INEN) in Lima. Cognitive function was assessed using the Addenbrooke’s Cognitive Examination (ACE), the INECO Frontal Screening Test (IFS), and a Facial Emotion Recognition (FER) task to evaluate social cognition. Baseline tests were performed before the start of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
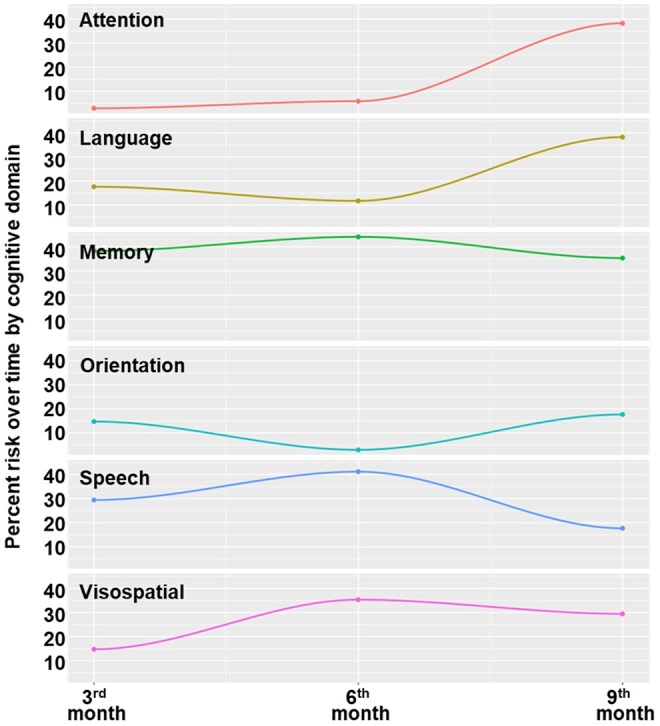 Figure 1
Figure 1| Means (SD) | |
|---|---|
|
| |
|
| 48.3 (8.9) |
|
| 13.0 (1.7) |
|
| 46.5 (4.9) |
|
| 11.4 (3.3) |
|
| |
|
| |
|
| 72 (58.1) |
|
| 52 (41.9) |
|
| |
|
| 91 (73.4) |
|
| 33 (26.6) |
|
| |
|
| 31 (25.0) |
|
| 42 (33.9) |
|
| 50 (40.3) |
|
| 1 (0.8) |
|
| |
|
| 5 (4.0) |
|
| 54 (43.5) |
|
| 19 (15.3) |
|
| 46 (37.1) |
|
| |
|
| 16 (12.9) |
|
| 15 (12.1) |
|
| 26 (21.0) |
|
| 67 (54.0) |
|
| |
|
| 72 (58.1) |
|
| 33 (26.6) |
|
| 16 (12.9) |
|
| 2 (1.6) |
|
| 1 (0.8) |
| Test | Evaluations | ||||
|---|---|---|---|---|---|
| E0 | E1 | E2 | E3 | ||
|
| 25 | 30 | 27 | 21 | |
| 27 | 29 | 26 | 17 | ||
| 15 | 26 | 22 | 17 | ||
| 24 | 31 | 30 | 29 | ||
| 25 | 31 | 28 | 25 | ||
| 26 | 30 | 28 | 25 | ||
| 26 | 33 | 32 | 12 | ||
| 23.38 ± 4.1 | 29.75 ± 2.2 | 27.25 ± 3.2 | 20.75 ± 5.9 | ||
|
| 21% IC 95% (7.3-34.7) | ||||
|
| 18 | 25 | 22 | 19 | |
| 14 | 20 | 19 | 16 | ||
| 25 | 25 | 24 | 20 | ||
| 14 | 26 | 23 | 18 | ||
| 17.75 ± 5.2 | 24 ± 2.7 | 22 ± 2.2 | 18.25 ± 1.7 | ||
|
| 12% IC 95% (1.1-22.9) | ||||
|
| 90 | 92 | 91 | 89 | |
| 83 | 94 | 93 | 92 | ||
| 89 | 95 | 94 | 90 | ||
| 86 | 95 | 92 | 91 | ||
| 97 | 97 | 96 | 76 | ||
| 90 ± 5.2 | 94.6 ± 1.8 | 9.2 ± 1.9 | 87.6 ± 6.6 | ||
|
| 15% IC 95% (3-27) | ||||
| Evaluations ( | ||||
|---|---|---|---|---|
| E0 | E1 | E2 | E3 | |
|
| 1.84 ± 1.28 | 2.15 ± 1.28 | 2.46 ± 1.28 | 2 ± 1.55 |
|
| 3.28 ± 1.48 | 3.58 ± 1.4 | 3.77 ± 1.24 | 3.29 ± 1.32 |
|
| 3.48 ± 1.09 | 3.95 ± 0.93 | 4.25 ± 0.85 | 3.34 ± 1.39 |
|
| 3.74 ± 1.14 | 4.10 ± 0.97 | 4.27 ± 0.93 | 4.09 ± 1.12 |
|
| 3.89 ± 1.49 | 4.28 ± 1.14 | 4.26 ± 1.19 | 4.06 ± 1.61 |
|
| 4.11 ± 1.17 | 4.64 ± 0.64 | 4.35 ± 1.09 | 4.37 ± 1.19 |
|
| 4.9 ± 0.36 | 4.99 ± 0.09 | 4.99 ± 0.11 | 4.94 ± 0.34 |
|
| 25.23 ± 4.29 | 27.68 ± 3.23 | 28.34 ± 3.83 | 26.09 ± 5.3 |
| Domain | Third month (%) | Sixth month (%) | Ninth month (%) |
|---|---|---|---|
|
| 14.71 | 2.94 | 17.64 |
|
| 2.94 | 5.88 | 38.23 |
|
| 38.24 | 44.12 | 35.29 |
|
| 29.41 | 41.18 | 17.65 |
|
| 17.65 | 11.76 | 38.24 |
|
| 14.71 | 35.29 | 29.41 |
- —Tecnología e Innovación Tecnológica (CONCYTEC)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer-related cognitive impairment studies · Brain Metastases and Treatment · Advanced Breast Cancer Therapies
Introduction
Cognitive ability, shaped by evolution, allows us to perceive, process, and interpret information from our environment. It is not learned but a function of our sensory and central nervous systems, making the brain a predictive machine that reduces uncertainty by interpreting stimuli.1–3 Cognitive changes, often manifesting as difficulties in attention, memory, concentration, and executive functioning, have been reported in 16% to 75% of women undergoing chemotherapy for breast cancer.4–8
In Peru, breast cancer is the most prevalent malignancy among women and the second leading cause of cancer-related mortality.9^,^10 The Peruvian population is characterized by high Amerindian ancestry, which has been linked to unique epidemiological patterns in disease susceptibility and outcomes.11–19 According to GLOBOCAN, an estimated 7,797 new breast cancer cases were projected for Peru by 2022, making it the most common cancer among women, predominantly affecting the economically active population. The mean age of onset is 49 years, a decade earlier than that observed in Europe and the United States, with a higher incidence of triple-negative breast cancer, which often necessitates more aggressive chemotherapy.14–16^,^20–22
With the aging population, both degenerative diseases such as dementia and breast cancer are on the rise, highlighting the need for studies that explore the prevalence of cognitive impairment in women diagnosed with breast cancer and assess its impact on this population.23^,^24 Our study aimed to determine the prevalence of cognitive impairment using brief psychological tests, including the Addenbrooke’s Cognitive Examination (ACE) and the INECO Frontal Screening (IFS) test, to evaluate general cognition and executive functions. Additionally, we sought to assess Facial Emotion Recognition (FER) as an objective, accessible tool for evaluating social cognition.25–33 The INECO Frontal Screening (IFS), Addenbrooke’s Cognitive Examination (ACE), and Facial Emotion Recognition (FER) tests instead of the tools recommended by the International Cognition and Cancer Task Force (ICCTF) because they offered broader, more integrative insights into the cognitive and emotional status of our participants. Specifically, we worked with Peruvian women diagnosed with breast cancer, most of whom had incomplete formal education. While the ICCTF tools (such as the Trail Making Test, COWAT, and HVLT-R) are widely validated for assessing isolated cognitive domains, they often assume a level of education or cultural familiarity that may limit their applicability in lower-education settings. In contrast, the IFS allowed us to explore executive functions in a more comprehensive and accessible way, the ACE provided a global cognitive screening tailored to Spanish-speaking populations, and the FER test added a valuable dimension by addressing social and emotional processing—an area not covered by the ICCTF battery. Additionally, unlike many ICCTF-based studies that rely on comparisons with a control group, our study did not include a control group, making it even more important to use screening tools capable of capturing a broad and meaningful cognitive profile within the patient group alone. Together, these instruments helped ensure that our cognitive assessments were not only scientifically robust but also culturally and contextually appropriate, capturing the realities and needs of the women we aimed to study.
Materials and methods
Patients’ sampling and study design
This longitudinal study, conducted at the National Institute of Neoplastic Diseases (INEN) in Lima, Peru, focuses on women with early-stage breast cancer. It included 143 female patients aged 28-64 years, diagnosed with breast cancer who had not received prior chemotherapy. To ensure eligibility, participants underwent a Beck Depression Inventory-II test; those with a score below 14 or symptoms of depression were excluded. Blood tests for B12, TSH, T3, and T4 were also performed, and patients with results outside the normal range were excluded.
The COVID-19 pandemic limited the recruitment of new patients to complete the number of patients scheduled for the study. The patients involved had to meet inclusion criteria such as women older than 18 years diagnosed with breast cancer, not having received chemotherapy, having at least 4 years of elementary education; and exclusion criteria such as: presence of metastasis, some type of neurological disorder (Alzheimer’s disease, vascular dementia, frontotemporal dementia, epilepsy, febrile seizures, Parkinson’s disease, and others), any type of autoimmune disease, pregnant patients, if receiving additional treatment, patients with vascular cognitive disorder based on assessment of vascular risk factors (hypertension, diabetes mellitus, hyperlipidemia, obesity, and others), and modified Hachinski index; and elimination criteria such as: insufficient biological material, incomplete cognitive function assessment.
All participants provided informed consent, and the study was approved by the INEN Ethics Committee. Clinical and sociodemographic information was compiled into a database. Blood samples were collected by INEN-trained personnel. The study involved baseline cognitive and psychological assessments, with follow-up cognitive testing conducted quarterly at 3, 6, and 9 months after the initiation of chemotherapy. The type of chemotherapy received by each patient was also recorded.
Psychological brief cognitive tests
The psychological assessment, conducted by a psychologist, included the IFS test, the Facial Emotion Recognition (FER) test, and the ACE test. These tests were used to evaluate executive functions, social cognition, and general cognition, respectively and were administered in their validated Peruvian versions.25–28
ACE assessed 6 cognitive domains with a maximum score of 100 points: orientation (10 points), attention (8 points), memory (35 points), verbal fluency (14 points), language (28 points), and visual-spatial skills (5 points). Additionally, ACE included components of the Mini-Mental State Examination (MMSE), contributing 30 points to the overall score. While the MMSE allocated 3/30 points to memory function, ACE assigned 35/100 points. The Peruvian study identified a cut-off score of 86 out of 100 as most effective for detecting dementia, demonstrating high sensitivity and specificity. This cut-off point also ensures that dementia classification is consistent regardless of sex, age, or years of education.26
IFS is a concise cognitive assessment tool used to evaluate executive functions, consisting of 8 subtests. These include motor programming (3 points), conflicting instructions (3 points), inhibitory motor control (3 points), digit counting in reverse order (6 points), verbal working memory (2 points), spatial working memory (4 points), capacity for abstraction (3 points), and verbal inhibitory control (6 points). With a maximum total score of 30 points, IFS can be administered and scored in approximately 10 minutes. A score of 23 or below indicated executive and social impairment. The Peruvian version of IFS has demonstrated high efficacy, with a sensitivity of 94.12% and a specificity of 94.2%, surpassing the Frontal Assessment Battery in its ability to detect cognitive impairments.29
FER involved identifying facial expressions that convey basic emotions such as fear, happiness, and disgust. Basic human emotions are categorized into 6 types: anger, disgust, fear, happiness, sadness, and surprise, in addition to neutral expressions.30–35 In our evaluation, 7 facial expressions were assessed: happiness, surprise, neutral, sadness, fear, disgust, and anger. These expressions are presented in a set of 35 images used for the test.
Chemotherapy schemes
All patients received the same chemotherapy regimen, which included hormonotherapy, anthracyclines, and taxanes, with some variations based on the pathological diagnosis and immunohistochemistry approach related to the type of breast cancer. The standard chemotherapy regimen consisted of doxorubicin hydrochloride (Adriamycin) and cyclophosphamide, followed by paclitaxel (Taxol), specifically administered as Adriamycin + Cyclophosphamide (AC) followed by Paclitaxel (Table S1).
Genotyping and quality control (QC)
Genotyped data were obtained with the Affymetrix Precision Medicine Research Array (PMRA) Chip, and quality control of the whole genome genotype was performed in PLINK v1.933. Markers from sex chromosomes were excluded; SNPs with more than 2% absence in the data, Hardy–Weinberg equilibrium at a P-value of <5 × 10^−5^ and alleles with a minor allele frequency (MAF) below 5% were excluded. Individuals with more than 5% loss of genotyped information were excluded. The search for genetically related individuals was performed using KING v2.2.5 to be removed from the study (no related participants >12.5% were found). After performing the QC, palindromic variants were eliminated.
Genetic ancestry and principal component analysis (PCA)
Individual global genetic ancestry was estimated using ADMIXTURE, ADMIXTURE continental ancestry estimates obtained in unsupervised analysis, assuming K = 4. Genotyped data were pruned using PLINK v1.933 and merged with data from the 1000 Genomes Project with admixed Americans, Europeans, east Asians, and African populations. PCA was performed in unrelated individuals to estimate the genetic structure of the Peruvian population under study (135 participants).
Identification of genetic polymorphisms for APOE and TREM2 genes
R Studio and PLINK v1.933 were used to select the polymorphisms that were studied in the APOE and TREM2 genes from the genotyped data (without QC, simply MAF). The genetic information that was discovered for each person in the study was combined with their phenotype (as measured by the ACE, IFS, and FER psychological tests) and their ancestry values for each continental group. Data on sociodemographic characteristics were listed among the covariates.
Statistical analysis
To evaluate changes in cognitive performance over time and in accordance with the study design, a multivariate analysis was performed; a linear mixed model of repeated measures was chosen. 4 cut-off points were established for each evaluation (E0, E1, E2, and E3); as follows: E0—for Baseline scores (prior to the start of chemotherapy), E1—for Evaluation 1 (3 months after starting treatment), E2—for Evaluation 2 (6 months after starting treatment) and E3—for Evaluation 3 (9 months started treatment). To fit the model, fixed and random effects were considered. The fixed effect variables were evaluation 0 (Baseline), age, level of education, number of normal pregnancies, number of abortions, and menopause. Each patient was considered as a random variable and as a dependent variable, the scores of each evaluation in the sections (Assessment 1, 2, and 3); corresponding to 3, 6, and 9 months of starting the treatment to find the minimum clinically important difference, the patients who presented sustained alterations in the E2 and E3 controls of the study were evaluated.36^,^37 Chemotherapy regimens were included as a time interaction covariate. In addition, the Toeplitz structure matrix and an autoregressive structure model (AR1) were used. The Akaike Information Criterion was used as a reference for estimating variance parameters for each analysis. A P-value <.05 was considered for a statistically significant difference or relationship. The PostgreSQL 12, SPSS 27, and R Studio 1.3.1093 packages were used.
Results
Sociodemographic and clinical characteristics
The mean age at diagnosis of invasive breast cancer was 48.3 years (SD = 8.98). The average age at menarche was 13 ± 1.7 years, and the mean age at menopause was 46.5 ± 4.9 years. Among the participants, 63 women (50.8%) were premenopausal. The majority, 72 patients (58.1%), resided in the Lima region, while 52 (41.9%) lived in other regions of the country.
Regarding educational level, 91 women (73.4%) had completed secondary education, whereas 33 (26.6%) had not; the average number of years of schooling was 11.4. Marital status distribution showed that 31 women (25.0%) were cohabitants, 42 (33.9%) were married, 50 (40.3%) were single (including separated, divorced, or widowed), and one participant (0.8%) did not report this information. Employment status indicated that 5 women (4%) were employed, 54 (43.5%) were not working (including those previously employed), 19 (15.3%) were self-employed, and 46 (37.1%) were unemployed.
In terms of reproductive history, 16 women (12.9%) had never been pregnant, 15 (12.1%) reported one pregnancy, 26 (21%) had 2 pregnancies, and 67 women (54%) had more than 2 pregnancies (Table 1).
Cognitive performance
Patients received an average of 10.8 chemotherapy cycles. The most commonly administered regimen was Adriamycin combined with cyclophosphamide followed by paclitaxel (AC + Paclitaxel), received by 71 patients (57.3%). Those with triple-negative breast cancer received adjuvant capecitabine.
Cognitive function was assessed using 3 instruments: the IFS for executive function, ACE for global cognition, and the FER for social cognition. According to these assessments, the FER test identified impairments in 21% of patients, the IFS test in 12%, and the ACE test in 15% (Table 2).
The emotion “fear” was the most difficult to recognize, whereas “happiness,” “surprise,” and “neutral” were recognized more accurately. Lower FER scores were observed in patients with poorer executive and cognitive performance, both before and after chemotherapy (Table 3). Higher IFS and ACE scores were associated with better emotion recognition performance. Additionally, patients with at least secondary education showed better cognitive outcomes across domains including facial recognition, orientation, attention, concentration, memory, and language.
Notably, attention and language domains showed greater risk of impairment by the sixth month of chemotherapy. Visuospatial ability, already affected at 6 months, declined further by the ninth month of treatment (Figure 1, Table 4).
Chemotherapy-related cognitive changes over time based on risk behavior by domain.
Genetic and ancestry findings
Ancestry analysis was conducted in 135 individuals. Amerindian ancestry was predominant, representing 77.8% of the cohort, followed by European ancestry (15.7%) and African ancestry (mean 5.8%). The average African genetic ancestry observed was higher than that reported in previous studies of Peruvian patients with breast cancer.15 The detailed distribution of ancestry components by individual is available in the Supplementary Material (Table S2).
Discussion
Chemotherapy treatment has been associated with alterations in cognitive performance, particularly affecting executive functions and emotion recognition, thus revealing impairments in social cognition processes. In our study, executive functions were evaluated using the FER, ACE, and IFS tests. The FER test identified decreased cognitive performance in 21% of patients, while the ACE and IFS tests showed declines in 15% and 12% of cases, respectively. These findings are consistent with previous reports indicating a measurable impact of chemotherapy on executive function domains, such as attention, working memory, and verbal fluency.1^,^38
Notably, better emotion recognition performance was associated with higher ACE and IFS scores, supporting the close interaction between cognitive and emotional processing. Fear—an emotion strongly associated with the temporal lobes and amygdala (Theory of Mind)—was the most difficult emotion for patients undergoing chemotherapy to recognize.1^,^38 This aligns with existing literature highlighting the amygdala’s crucial role in emotion and social behavior. Studies in individuals with amygdala lesions have demonstrated impaired recognition of emotional facial expressions, particularly fear, reinforcing its importance in emotional processing.39^,^40
Research using animal models and neuroimaging has shown that chemotherapy can directly affect cognitive function, especially in frontal regions responsible for executive and memory-related tasks. Emotion recognition via facial expression, a universal phenomenon widely studied in psychology, has been explored since Darwin’s evolutionary theory of 1868, which proposed that such expressions serve an adaptive role in communication and survival.41 According to this theory, facial expressions are biologically encoded and evolved through natural selection to facilitate social interaction and understanding.
In our analysis, emotion recognition scores were consistently lower among patients with executive and cognitive impairments, across all evaluations (E0, E1, E2, and E3) (Table 2). Moreover, patients with a high school education or higher exhibited better performance in cognitive domains such as facial recognition, orientation, attention, memory, and language (Table 4). These findings suggest the influence of cognitive reserve, consistent with prior observations that lower education levels are associated with higher vulnerability to cognitive dysfunction and increased mortality.42
Specifically, IFS testing revealed that 12% of patients exhibited executive function impairments, affecting abilities such as inhibitory control, attention regulation, and flexible thinking.43–46 In our study, attention and language domains were particularly affected at the sixth-month chemotherapy follow-up (Table 4). A decrease in visuospatial ability was observed at this time point as well, dropping from 35.29 to 29.41 by the ninth-month follow-up.
The identification of predictive factors for cognitive performance in breast cancer patients remains challenging. There is a clear need for brief, user-friendly diagnostic tools to assess executive functions and social cognition.47^,^48 An ideal screening instrument would be concise, require minimal materials, be easy to score, and demonstrate high sensitivity and specificity for detecting cognitive impairment.49
Interestingly, several studies have reported that cognitive deficits may be present even before the start of chemotherapy, suggesting a possible baseline vulnerability. These deficits may be influenced by cancer-related biological changes or shared risk factors for both cancer and cognitive decline.50^,^51 Longitudinal studies have shown that 20%-30% of patients exhibit cognitive impairments prior to treatment initiation.52 In line with this, Jansen et al. (2011) found that 23% of 71 breast cancer patients had cognitive dysfunction before starting chemotherapy.53
The most frequently used chemotherapy protocol in our cohort was a combination of doxorubicin hydrochloride (Adriamycin) and cyclophosphamide followed by paclitaxel (Taxol), administered to 71 patients (57.3%). This regimen (AC + Paclitaxel) has previously been associated with neurotoxic effects. Moreover, when taxanes are combined with hormonal therapy, cognitive decline appears to intensify, although the duration of these effects remains unclear.53
The mechanisms underlying chemotherapy-induced cognitive impairment are not yet fully understood, though changes in the central nervous system are known to be heterogeneous. Several hypotheses have been proposed, including toxicity to non-tumor cells, microvascular damage, hormonal disruption, and immune activation via cytokines such as TNF-α.54^,^55 Additionally, genetic factors such as TREM2 and APOE may modulate microglial activity and influence cognitive outcomes. The involvement of these genes in “chemo brain” and their interaction with ancestry-specific polymorphisms remains an area of active investigation.56^,^57
It remains unclear how genetic polymorphisms influence the risk of cognitive decline in breast cancer patients.58–69 Given Peru’s diverse genetic makeup, the prevalence and impact of such polymorphisms may differ significantly compared to other populations.13^,^24^,^70–73 Ancestry plays a key role in the frequency of risk alleles. For example, the APOE ε4 allele has a lower frequency in Peruvians (4.6%) compared to Caucasian populations, and TREM2 variants have not been studied in cognitively impaired Peruvian individuals. Marca et al. identified the APOE ε4 allele in 4.6% of cognitively normal Peruvians.25^,^73 Genetic studies in Peruvians have shown a predominant Quechua ancestral component in central regions, with Andean-Piedmont subcomponents in the north and a smaller Aymara influence in the south.74^,^75
In our sample, Amerindian ancestry comprised 77.8%, and the proportion of African ancestry (5.8%) was higher than in other Peruvian studies of breast cancer patients.15 This population structure presents a unique opportunity to evaluate how Amerindian ancestry and related genetic polymorphisms may contribute to cognitive decline and dementia risk.14^,^16^,^20 Accurate assessment of cognitive impairment and the implementation of tailored clinical protocols will be essential for understanding the underlying biological mechanisms and identifying potential molecular markers associated with cognitive deterioration.76
Conclusions
The implementation of brief, accessible, and objective cognitive tests that provides independent evaluation of educational levels is essential for assessing patients undergoing chemotherapy in standard-of-care settings. The FER test is a promising tool for this purpose, as it is easy to implement and does not require specialized personnel for administration.
Additionally, studying cognitive impairment caused by cancer chemotherapy is crucial to identify genes and polymorphisms associated with this condition in the Peruvian population, which has a high Amerindian ancestry and has been underrepresented in cancer research. Such research will enhance our understanding of risk factors and enable the development of tailored treatment options.
Supplementary Material
oyag058_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tirapu-Ustárroz J , Pérez-Sayes G, Erekatxo-Bilbao M. Pelegrín-valero C. ¿Qué es la teoría de la mente? Rev Neurol. 2007;44:479-489.17455162 · pubmed ↗
- 2Bubic A , Yves von Cramon D, Schubotz RI. Prediction, cognition and the brain. Vol. 4, Frontiers in Human Neuroscience. Frontiers Media S. A.; 2010.10.3389/fnhum.2010.00025 PMC 290405320631856 · doi ↗ · pubmed ↗
- 3De Ridder D , Verplaetse J, Vanneste S. The predictive brain and the “free will” illusion. Front Psychol. 2013;4:10.3389/fpsyg.2013.00131 PMC 363940323641219 · doi ↗ · pubmed ↗
- 4Argyriou AA , Assimakopoulos K, Iconomou G, Giannakopoulou F, Kalofonos HP. Either called “chemobrain” or “chemofog,” the long-term chemotherapy-Induced cognitive decline in cancer survivors is real. J Pain Symptom Manage. 2011;41:126-139.20832978 10.1016/j.jpainsymman.2010.04.021 · doi ↗ · pubmed ↗
- 5Ibrahim EY , Domenicano I, Nyhan K, et al Cognitive effects and depression associated with taxane-based chemotherapy in breast cancer survivors: a meta-analysis. Front Oncol. 2021;11:642382.33996556 10.3389/fonc.2021.642382 PMC 8121254 · doi ↗ · pubmed ↗
- 6Vardy J , Rourke S, Tannock IF. Evaluation of cognitive function associated with chemotherapy: a review of published studies and recommendations for future research. J Clin Oncol. 2007;25:2455-2463.17485710 10.1200/JCO.2006.08.1604 · doi ↗ · pubmed ↗
- 7Breckenridge LM , Bruns GL, Todd BL, Feuerstein M. Cognitive limitations associated with tamoxifen and aromatase inhibitors in employed breast cancer survivors. Psychooncology. 2012;21:43-53.20967847 10.1002/pon.1860 · doi ↗ · pubmed ↗
- 8Hermelink K. Chemotherapy and cognitive function in breast cancer patients: the so-called chemo brain. J Natl Cancer Inst Monogr. 2015;2015:67-69.26063891 10.1093/jncimonographs/lgv 009 · doi ↗ · pubmed ↗