Stroke as the Leading Cause of Death in Rural Ludhiana, India: A Verbal Autopsy From the Population-Based Rural Stroke Registry of Ludhiana
Shavinder Singh, Clarence J Samuel, Deepshikha Kamra, Melkey S Bunyan, Ranjit Injety, Jeyaraj D Pandian

TL;DR
Stroke is the top cause of death in rural Ludhiana, India, with high mortality rates linked to uncontrolled hypertension and poor access to acute care.
Contribution
This study provides a population-based verbal autopsy analysis showing stroke as the leading cause of death in rural Ludhiana, India.
Findings
Stroke accounted for 22.2% of all deaths in rural Ludhiana, with a crude mortality rate of 55.4 per 100,000.
83.6% of stroke deaths occurred within 30 days of symptom onset, and 81.7% of stroke victims had uncontrolled hypertension.
Women had a higher cause-specific mortality fraction (24.7%) compared to men (20.5%) despite lower crude rates.
Abstract
Introduction Stroke is the second leading cause of global mortality, with a disproportionately high burden in low- and middle-income countries (LMICs). In regions with limited medical certification of death, verbal autopsy (VA) serves as a critical tool for determining the cause-of-death distribution. This study aimed to determine the stroke mortality in rural Ludhiana, Punjab, India. Materials and methods A prospective, population-based study was conducted between December 2016 and November 2018 across two rural blocks in Ludhiana (Pakhowal and Sidhwan Bet), covering a total population of 236,266. Frontline health workers identified all-cause mortality, followed by home-based VA. To ensure data integrity and minimize misclassification, two independent neurologists adjudicated stroke deaths using World Health Organization (WHO) standards and Indian Council of Medical Research (ICMR)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1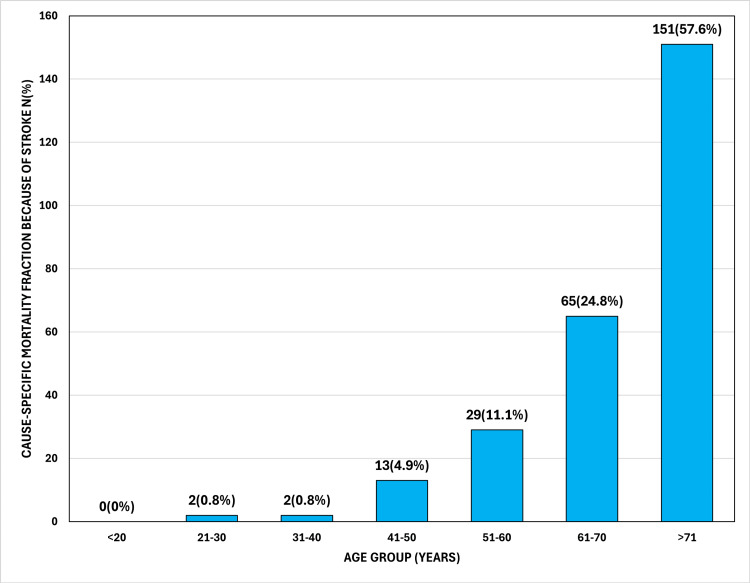 Figure 2
Figure 2| Variables | Male | Female | Total |
| Total deaths (n) | 708 | 474 | 1,182 |
| two-year population person-years | 252,646 | 219,886 | 472,532 |
| Stroke deaths, n (%) | 145 (55.3%) | 117 (44.7%) | 262 (100%) |
| Cause-specific mortality fraction (CSMF), % (95% CI) | 20.5% (17.5-23.5) | 24.7% (20.8-28.6) | 22.2% (19.8-24.5) |
| Mean age of stroke deaths (SD) | 69.0 (15.0) | 73.1 (12.2) | 70.8 (13.9) |
| Crude stroke mortality rate per 100,000 (95% CI) | 57.4 (48.5-67.4) | 53.2 (44.0-63.7) | 55.4 (48.9-62.5) |
| Age Group (Years) | Women Rate | Men Rate | Total Rate (Annualized) |
| <25 | 0.0 | 5.6 | 3.0 |
| 25-29 | 0.0 | 5.5 | 3.0 |
| 30-34 | 0.0 | 5.5 | 3.0 |
| 35-39 | 0.0 | 5.5 | 2.9 |
| 40-44 | 6.4 | 11.0 | 8.8 |
| 45-49 | 19.1 | 38.8 | 29.4 |
| 50-54 | 12.7 | 60.7 | 38.4 |
| 55-59 | 25.4 | 66.2 | 47.2 |
| 60-64 | 82.6 | 82.8 | 82.7 |
| 65-69 | 139.7 | 82.7 | 109.2 |
| 70-74 | 133.5 | 138.0 | 135.9 |
| 75-79 | 82.6 | 71.8 | 76.8 |
| 80-84 | 95.4 | 88.3 | 91.5 |
| ≥85 | 146.1 | 137.9 | 141.7 |
| Total (crude) | 53.2 | 57.4 | 55.4 |
| Risk Factors | Male, n (%) | Female, n (%) | Total, n (%) |
| Hypertension | 115 (79.3%) | 99 (84.6%) | 214 (81.7%) |
| Diabetes mellitus | 44 (30.3%) | 45 (38.5%) | 89 (34.0%) |
| Heart disease | 28 (19.3%) | 17 (14.5%) | 45 (17.2%) |
| Smoking | 22 (15.2%) | 0 (0.0%) | 22 (8.4%) |
| Time to Death From the Onset of Symptoms, n (%) | Women (n=117) | Men (n=145) | Total (n=262) |
| ≤30 days | 92 (78.6%) | 127 (87.6%) | 219 (83.6%) |
| <7 days (subset) | 50 (42.7%) | 76 (52.4%) | 126 (48.1%) |
| >30 days | 12 (10.3%) | 12 (8.3%) | 24 (9.2%) |
| Unclear from the narrative | 13 (11.1%) | 6 (4.1%) | 19 (7.3%) |
| Age Group | Two-Year Deaths | Population | WHO Weight | Weighted Rate |
| <25 | 1 | 116,561 | 0.4284 | 0.18 |
| 25-29 | 1 | 16,910 | 0.0793 | 0.23 |
| 30-34 | 1 | 17,043 | 0.0761 | 0.22 |
| 35-39 | 1 | 17,212 | 0.0715 | 0.21 |
| 40-44 | 3 | 17,015 | 0.0659 | 0.58 |
| 45-49 | 10 | 13,634 | 0.0604 | 2.22 |
| 50-54 | 13 | 11,728 | 0.0537 | 2.98 |
| 55-59 | 16 | 11,664 | 0.0455 | 3.12 |
| 60-64 | 28 | 12,692 | 0.0372 | 4.10 |
| 65-69 | 37 | 11,446 | 0.0296 | 4.78 |
| 70-74 | 46 | 11,043 | 0.0221 | 4.60 |
| 75-79 | 26 | 9,771 | 0.0152 | 2.02 |
| 80-84 | 45 | 8,203 | 0.0091 | 2.50 |
| ≥85 | 34 | 5,294 | 0.0063 | 2.02 |
| Total | 262 | 236,266 | 1.000 | 29.7 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Autopsy Techniques and Outcomes · Global Health and Epidemiology
Introduction
Globally, stroke is the second leading cause of death and the third leading cause of disability. Data from the low- and middle-income countries (LMICs) show a disproportionately high burden, with age-standardized mortality rates (ASMR) and disability-adjusted life years (DALYs) exceeding the global average by a factor of four. One in four adults over 25 will have a stroke in their lifetime [1,2].
The Southeast Asia Region (SEAR) makes up more than 40% of the world's stroke mortality and covers 11 culturally, geographically, and socially varied nations that are transitioning to noncommunicable diseases. Stroke care throughout all stages varies significantly among SEAR nations, despite common issues in healthcare access, awareness, and patient behavior. There is a paucity of high-quality stroke epidemiology data from this region. Although ischemic stroke is common, intracerebral hemorrhage is more common in several SEAR countries than in the rest of the world [3]. A number of factors contribute to this high burden, including an aging population, rising risk factors (diabetes, hypertension, alcohol and tobacco use, and physical inactivity), and environmental issues, including air pollution and extreme weather conditions [4].
According to the Indian Global Burden of Disease (GBD) Study 1990-2019, stroke is the main contributor to neurological-related mortality and the largest contributor to DALYs [5]. Studies across various regions, including Mumbai, Trivandrum, Ludhiana, Kolkata, and rural West Bengal, reveal a high incidence of stroke, with high case fatality and mortality rates. The one-month case fatality was between 18% and 42% [6]. According to the Indian Council of Medical Research (ICMR)-National Centre for Disease Informatics and Research (NCDIR) report, the crude incidence of stroke was 138.1 per 100,000 population. Age-standardized case fatality rates per 100,000 population for the pooled population-based stroke registry (PBSR) per 100,000 were 20.0 for men and 18.8 for women. In Cuttack, Cachar, and Tirunelveli PBSR, the percentage of registered cases from rural regions (ranging from 57.2% to 85.2%) exceeded that from urban areas (ranging from 14.8% to 42.8%), attributable to the substantial rural population [7]. A study on stroke incidence in urban Kolkata, North India, revealed a standardized incidence rate of 145.3 per 100,000 persons per year and a 30-day case fatality rate of 41%, both above estimates from industrialized countries [8]. A study conducted in urban and rural regions of Ludhiana compared stroke profiles and outcomes, where hemorrhagic stroke was seen more in rural regions than in urban regions. Age-standardized incidence rates in the rural area were 218.5/100,000 in 2017 and 197.6/100,000 in 2018, with drug abuse and hypertension being the most common risk factors for stroke [9,10].
According to the National Stroke Registry Programme (NSRP), ICMR-NCDIR shows that among all the registries, Varanasi PBSR reported the highest case fatality rate (CFR) (46.6 per 100,000 population) owing to stroke, followed by Cachar PBSR (39.9) and Cuttack PBSR (31.4). The case fatality proportion varied from 12.2% in Kota PBSR to 41.2% in Cachar PBSR. Kota PBSR had the lowest crude mortality rate (CMR) per 100,000 people (16.2), while the Varanasi registry had the highest (48.9). Among all the registries, Kota PBSR had the lowest age-adjusted case fatality rate per 100,000 people (13.0), whereas Varanasi PBSR had the highest (35.5) [11]. Chronic illnesses were the main cause of death in a study on the causes of death in rural Andhra Pradesh, South India. The majority of deaths were caused by circulatory system diseases (32%), with similar percentages of ischemic heart disease (14%) and cerebrovascular disease (13%) [12]. A study in the Gadchiroli district documented stroke as the leading cause of death, accounting for 14.3% of mortalities [13].
Despite the documented rise of stroke across India, significant disparities persist between urban centers and rural agrarian communities. Current national data often overlook the specific challenges of rural North India, where an aging population and high hypertension prevalence coincide with limited acute care infrastructure. While urban registries provide clinical insights, a critical knowledge gap remains regarding the precise, annualized stroke mortality burden in these underserved regions. Stroke deaths are often underestimated due to misclassification in mortality data documentation. To address this critical issue, a multipronged approach is needed. To overcome these challenges in LMICs with limited resources, verbal autopsy (VA) emerges as a reliable alternative method to assess mortality at a population level [14]. The VA tool records the description of the symptoms and the circumstances leading to death. The data are analyzed manually by a physician who assigns an International Classification of Diseases, Tenth Revision (ICD-10) code for the underlying cause of death based on clinical guidelines [14,15]. Hence, we aimed to determine mortality due to stroke by using verbal autopsy to demonstrate the cause of death as a part of the Ludhiana rural population-based stroke registry.
Materials and methods
This investigation was conducted as part of phase II of the population-based rural stroke registry established in Ludhiana, Punjab. The study was implemented in two designated rural administrative blocks of the Ludhiana district: Pakhowal and Sidhwan Bet. A standardized verbal autopsy procedure was incorporated as a core component of the study protocol to ascertain stroke-related mortality and related epidemiological parameters. Ethical permission was obtained from the Institutional Ethics Committee of Christian Medical College Ludhiana (approval number: MCL-IEC/2013/0171/APPRVL/NEUROLOGY-ICMR), and the project was funded by the Task Force of ICMR.
After receiving training, accredited social health activists (ASHAs) were able to identify stroke victims in the community, who were then assessed by a neurologist [10]. The stroke cases were followed up by two research teams at home or at the hospital where they were admitted. The Ludhiana population-based stroke registry used verbal autopsy (VA) methods to collect data on stroke mortality, especially for deaths occurring at home where medical certification is unavailable. The VA tool (see Appendices) used was developed according to the World Health Organization (WHO) and Indian Council of Medical Research (ICMR) methodologies, and their feasibility was evaluated in a 2015 study [16]. To ensure data integrity, we implemented a multistage quality control process. We cross-referenced the registry and mortality data (hospital and home deaths) with municipal corporation centers to maximize capture rates. Two independent physicians reviewed all verbal autopsy narratives to confirm the cause of death, with a third expert resolving any discrepancies. Additionally, monthly field audits and a random review of interviews ensured data consistency. Individual training sessions and workshops were held in Ludhiana for the research staff and representatives of ICMR on both theoretical and practical aspects during the workshop.
This research was conducted across more than 150 villages in the rural blocks of Pakhowal and Sidhwan Bet, located in the Ludhiana district (Figure 1). According to 2011 census figures, the populations of Pakhowal and Sidhwan Bet were 109,201 and 127,065, respectively. The study's inclusion criteria focused on incident (first-ever) stroke cases and stroke-related fatalities identified during a two-year screening period from December 1, 2016, to November 30, 2018 [17,18].
Map of Block Pakhowal and Sidhwan BetNote: Image sourced from "Multicomponent short-term training of ASHAs for stroke risk factor management in rural India," by Jain M, Pandian J, Samuel C, Singh S, Kamra D, Kate M, 2019, J Neurosci Rural Pract, 10(4), 592-8 [18] under Creative Commons Attribution-NonDerivative-NonCommercial License (https://creativecommons.org/licenses/by-nc-nd/4.0/). No changes were made
Research teams visited deceased patients' homes and additional village households daily (at least five) to collect data using a verbal autopsy questionnaire. Local health workers provided death lists. Collected data was reviewed for errors by investigators and neurologists, who ultimately determined the stroke-related deaths. The study was conducted over a 24-month (two-year) surveillance period. To calculate the mortality rates, the total population at risk (236,266) was multiplied by the duration of the study, resulting in 472,532 person-years. To determine the stroke mortality burden in rural Ludhiana, we calculated the cause-specific mortality fraction (CSMF) as the proportion of stroke deaths relative to all-cause mortality, including 95% confidence intervals (CI). We expressed crude stroke mortality rates (CSMR) per 100,000 person-years. To enable global comparisons, we calculated age-standardized mortality rates (ASMR) using the WHO World Standard Population. We analyzed categorical variables, including sex-stratified risk factor prevalence (hypertension, diabetes, heart disease, and smoking) and time-to-death intervals (<7 days, ≤30 days, and >30 days). Finally, we reported mean ages at death with standard deviations (SD).
Results
The analysis of the data revealed that out of 1,182 total deaths recorded (Table 1), stroke was the leading cause of mortality, accounting for 262 (22.2%) deaths. This represents a cause-specific mortality fraction (CSMF) of 22.2% (95% CI: 19.8-24.5) (Table 1). The annualized crude stroke mortality rate for the combined census population was 55.4 per 100,000 (95% CI: 48.9-62.5) (Table 1). While the crude rate was higher in men (57.4) than in women (53.2), the CSMF was notably higher in women (24.7%) compared to men (20.5%) (Table 1).
The mean age of death due to stroke was 70.8 years, with women dying at a significantly higher mean age (73.1±12.2 years) than men (69.0±15.0 years) (Table 1). Age-specific crude rates showed an exponential increase with age (Table 2), with the highest mortality observed in the ≥85 age group at 141.7 per 100,000 (Table 2). Distribution analysis (Figure 2) showed that 151 (57.6%) of all stroke deaths occurred in individuals aged 71 years and older.
Age-Wise Cause-Specific Mortality Fraction Because of Stroke (N=262)
Hypertension was the most prevalent risk factor among stroke fatalities, present in 214 (81.7%) of cases, followed by diabetes mellitus at 89 (34.0%). It has been observed that the prevalence of hypertension (99, 84.6%) and diabetes (45, 38.5%) is higher in women (Table 3).
Regarding the clinical timeline, the majority of deaths were acute; 219 (83.6%) of deaths occurred within 30 days of symptom onset, with 126 (48.1%) occurring within the first seven days (Table 4).
The annualized age-standardized mortality rate (ASMR) was 29.7 per 100,000 person-years (95% CI: 26.1-33.4) (Table 5).
Discussion
Stroke represents a significant public health burden, often resulting from thrombotic occlusion within the cerebral vasculature [19]. The results of this community-based mortality registry in rural Ludhiana demonstrate that stroke is the preeminent cause of death, accounting for 22.2% of all recorded fatalities. This finding is significantly higher than the results reported by Kalkonde et al. in the Gadchiroli study, which found that stroke was the leading cause of death in rural Maharashtra, accounting for 14.3% of all deaths [13]. While both studies identify stroke as a primary public health threat, the higher cause-specific mortality fraction (CSMF) in Ludhiana (22.2%) suggests an even more advanced epidemiological transition in rural Punjab compared to rural Gadchiroli. This disparity likely reflects regional differences in lifestyle, dietary patterns, and the prevalence of metabolic risk factors [20].
The demographic profile of stroke mortality in our study also shows a distinct pattern. While the annualized crude mortality rate was higher in men (57.4 per 100,000) than in women (53.2 per 100,000), women exhibited a higher CSMF (24.7% versus 20.5%), indicating that stroke is a more dominant cause of death within the female cohort. Furthermore, the mean age of stroke death for women (73.1 years) was significantly higher than for men (69.0 years). This mirrors observations by Kalkonde et al., where stroke was a major killer across both sexes, but emphasizes that in Ludhiana, stroke mortality is heavily concentrated in the geriatric population, with 57.4% of deaths occurring in those aged 71 and above [13].
A critical finding in our registry is the high acute mortality rate, with 219 (83.6%) of deaths occurring within 30 days and 126 (48.1%) within the first seven days. This "acute-heavy" mortality profile is even more pronounced than that seen in other Indian verbal autopsy studies and highlights a severe lack of access to specialized acute care [21,22]. The overwhelming presence of hypertension (214, 81.7%) as the leading risk factor in our cohort reinforces the conclusion by Kalkonde et al. [13] that stroke is the "new epidemic" in rural India, driven primarily by uncontrolled blood pressure in communities with limited healthcare access [23].
From a public health perspective, these findings necessitate a multi-level intervention strategy focused on prevention, early recognition, and infrastructure development. Given that over 80% of stroke victims were hypertensive, we should intensify efforts through the India Hypertension Control Initiative (IHCI) to ensure a steady supply of antihypertensive medications at primary health centers (PHCs) and improve patient adherence [24]. To address the 126 (48.1%) deaths occurring in the first week, we should launch community awareness campaigns using Face, Arm, Speech, and Time (FAST), training community health workers (ASHAs and auxiliary nurse midwives {ANMs}) to educate families on symptom recognition to reduce prehospital delays [25]. Furthermore, Ludhiana is strengthening its "hub-and-spoke" model by equipping tertiary centers with dedicated stroke units while training rural PHCs to stabilize and rapidly transfer patients, as Tezpur has adopted [26]. In remote blocks such as Sidhwan Bet and Pakhowal, tele-consultation services are being explored to allow rural clinicians to consult with neurologists in real time, facilitating earlier diagnosis and treatment initiation before a patient reaches a tertiary facility [27].
Study strengths and limitations
The major strength of this study is its prospective, community-based design covering a large census population of over 236,000 individuals, which minimizes the selection bias often found in hospital-based registries. The use of physician-adjudicated verbal autopsy provides a reliable estimate of mortality in a region where formal medical certification of death is often unavailable. However, this study has certain limitations. The reliance on verbal autopsy involves inherent recall bias regarding symptoms and risk factors. To minimize the resulting risk of misclassification, we employed a rigorous quality control framework, including independent dual-physician adjudication and standardized WHO-ICMR protocols. Additionally, as a mortality registry, it does not capture nonfatal strokes, which means the total "stroke burden" (including disability) is likely much higher than reported here.
Conclusions
This community-based mortality registry confirms that stroke has become the leading cause of death in rural Ludhiana, accounting for nearly one-quarter of all fatalities. The high cause-specific mortality fraction (22.2%) and the stark 30-day mortality rate (83.6%) highlight a critical public health crisis in rural Punjab. These findings suggest that the region is experiencing an advanced epidemiological transition, where the burden of vascular disease now surpasses traditional infectious etiologies. The overwhelming prevalence of hypertension among stroke victims underscores the urgent need for robust primary prevention and grassroots blood pressure control programs, such as the India Hypertension Control Initiative (IHCI). Furthermore, the high rate of early mortality within the first week of symptom onset points to a significant gap in acute care access and community awareness.
To mitigate this burden, a comprehensive strategy integrating and expanding the FAST acronym for early symptom recognition, a decentralized "hub-and-spoke" model for acute care, and the expansion of tele-stroke services are essential. Addressing these systemic gaps is vital to reducing stroke-related mortality and improving the survival outcomes of rural populations in India.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Stroke Organization (WSO): global stroke fact sheet 2022 Int J Stroke Feigin VL Brainin M Norrving B 18291720223498672710.1177/17474930211065917 · doi ↗ · pubmed ↗
- 2Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019 Lancet Neurol GBD 2019 Stroke Collaborators 7958202020213448772110.1016/S 1474-4422(21)00252-0PMC 8443449 · doi ↗ · pubmed ↗
- 3Stroke systems of care in South-East Asia Region (SEAR): commonalities and diversities Lancet Reg Health Southeast Asia Sebastian IA Gandhi DB Sylaja PN 1002891720233784993010.1016/j.lansea.2023.100289 PMC 10577144 · doi ↗ · pubmed ↗
- 4The burden, risk factors and unique etiologies of stroke in South-East Asia Region (SEAR)Lancet Reg Health Southeast Asia Pandian JD Padma Srivastava MV Aaron S 1002901720233784993310.1016/j.lansea.2023.100290 PMC 10577147 · doi ↗ · pubmed ↗
- 5The burden of neurological disorders across the states of India: the Global Burden of Disease Study 1990-2019 Lancet Glob Health India State-Level Disease Burden Initiative Neurological Disorders Collaborators 0449202110.1016/S 2214-109X(21)00164-9PMC 829504334273302 · doi ↗ · pubmed ↗
- 6Stroke in India: a systematic review of the incidence, prevalence, and case fatality Int J Stroke Jones SP Baqai K Clegg A 1321401720223411491210.1177/17474930211027834 PMC 8821978 · doi ↗ · pubmed ↗
- 7Stroke incidence, mortality, subtypes in rural and urban populations in five geographic areas of India (2018-2019): results from the National Stroke Registry Programme Lancet Reg Health Southeast Asia Rangamani S Huliyappa D Kulothungan V 1003082320243840451310.1016/j.lansea.2023.100308 PMC 10884975 · doi ↗ · pubmed ↗
- 8A prospective community-based study of stroke in Kolkata, India Stroke Das SK Banerjee TK Biswas A 9069103820071727277310.1161/01.STR.0000258111.00319.58 · doi ↗ · pubmed ↗