Oropouche fever in Minas Gerais, Brazil, 2024: Epidemiological characterization, spatial distribution, and clinical implications
Edmundo Rinolino Magalhães Flores, Flavia Ribeiro Soares Cruzeiro, Iara Fabíola Rocha, Caroline Macedo Gonçalves, Thais Cristina Nazaré Freitas, Daniela Caldas Teixeira

TL;DR
This study reports the spread of Oropouche fever to Minas Gerais, Brazil, highlighting its new patterns and implications for public health.
Contribution
The study provides the first detailed epidemiological characterization of Oropouche virus in a non-endemic region of Brazil.
Findings
278 confirmed cases were reported in 10 municipalities, mainly in rural and peri-urban areas.
Women made up 55% of cases, with two distinct temporal peaks observed in different locations.
Symptom recurrence occurred in 25.5% of cases, and comorbidities like hypertension and diabetes were common.
Abstract
Oropouche fever (OF), caused by the Oropouche virus (OROV), has historically been endemic to the Amazon region; however, it is now emerging in other Brazilian states. This study describes the sociodemographic, clinical, and spatial characteristics of OROV cases identified in Minas Gerais in 2024 and contributes to the understanding of its transmission dynamics in non-endemic regions. This descriptive epidemiological study used the official surveillance data from the State Health Department of Minas Gerais (SES/MG). The confirmed cases were those with laboratory-confirmed OROV infection by RT-PCR at the Ezequiel Dias Foundation (FUNED). Demographic, geographic, and clinical data were analyzed using descriptive statistics. Exploratory comparisons by sex and age were performed. A total of 278 confirmed autochthonous cases were reported across 10 municipalities, primarily in rural and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
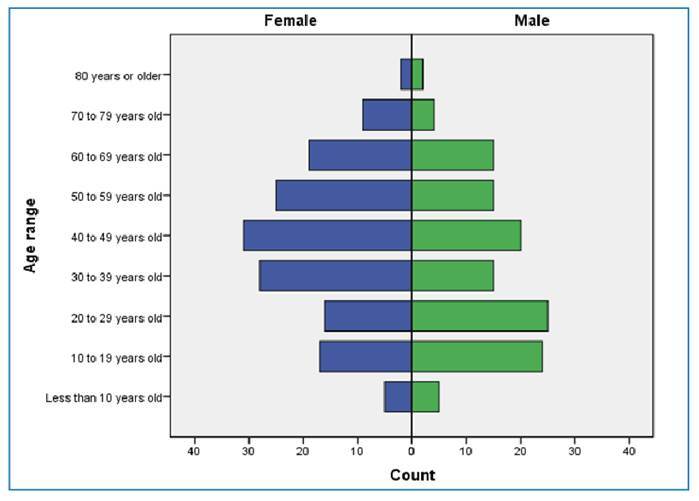 Figure 1
Figure 1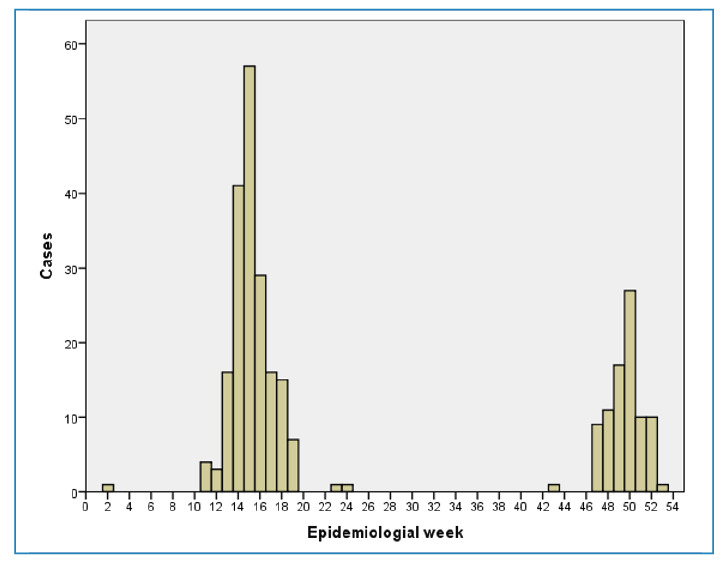 Figure 2
Figure 2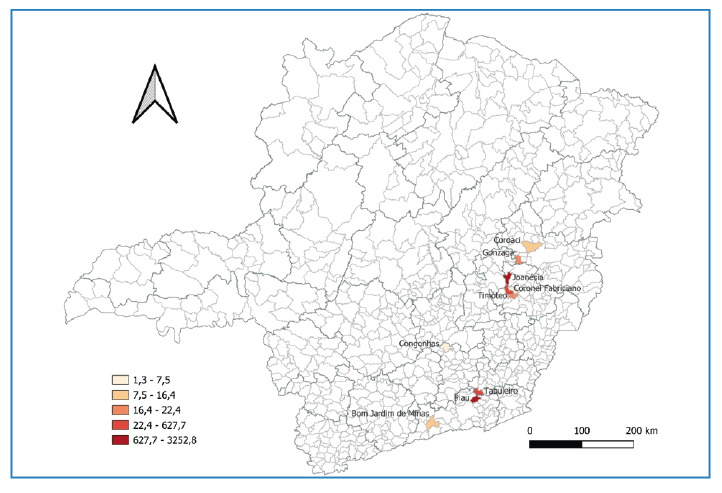 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVector-Borne Animal Diseases · Mosquito-borne diseases and control · Viral Infections and Vectors
INTRODUCTION
Oropouche fever (OF) is an acute febrile illness caused by the Oropouche virus (OROV), an arbovirus belonging to theOrthobunyavirusgenus of thePeribunyaviridaefamily1 ^,^ 2 ^.^ The virus is primarily transmitted through the bite ofCulicoides paraensisand circulates in two transmission cycles, urban and sylvatic, which may also involveAedesandCulexmosquitoes as well as vertebrate hosts such as primates and birds3 ^,^ 4. Since its identification in the 1960s, more than 500,000 human cases have been estimated to have occurred, although the true burden is possibly higher because of underdiagnosis and the clinical similarity of OF to other arboviral infections, such as dengue, Zika, and chikungunya5 ^,^ 6.
Oropouche fever is endemic to the humid tropical regions of Central and South America, including Brazil, and has historically shown a higher incidence in the Amazon region. However, reports from other states such as Minas Gerais and São Paulo indicate a geographic expansion of OROV transmission7 ^,^ 8. Although the disease is generally self-limiting, it can result in prolonged or recurrent symptoms, impaired quality of life, and productivity losses9 ^,^ 10. In addition, outbreaks in resource-limited settings pose challenges for local health systems.¹ In addition, limited access to specific diagnostic tools and gaps in clinical and epidemiological data hinder accurate case detection and the development of effective control strategies11 ^,^ 12.
According to the 2024 epidemiological update for the Region of the Americas13, 16,239 confirmed OF cases have been reported, including four deaths. The disease has occurred in 11 countries, including the Cayman Islands, with Brazil accounting for 13,785 cases and all reported deaths. The Amazon region, where OROV is endemic, accounts for 42.0% of Brazilian cases. Nonetheless, detection of the virus in regions outside the Amazon has led to confirmed infections in more than 15 states, including Minas Gerais. Fatal cases were reported in Bahia, Paraná, and Espírito Santo.
Given the recent detection of OROV in non-endemic areas, this study aims to describe the epidemiological profile of confirmed OF cases in Minas Gerais by 2024, thereby contributing to improved surveillance, case management, and public health policy planning in Brazil. In addition, exploratory analyses were performed to compare the frequency of key symptoms and comorbidities according to sex and age, with the aim of providing a more detailed clinical characterization of confirmed cases.
METHODS
Study design
This descriptive study analyzed all confirmed cases of OROV infection in Minas Gerais, Brazil. The data presented in this study correspond to cases with symptom onset dates beginning in 2024. Data were extracted on February 10, 2025, using the official health surveillance information system. Subsequent updates to the database may result in changes to the reported numbers. Therefore, comparisons with data extracted at different time points should account for potential modifications due to the ongoing data validation and consolidation processes.
In 2024, OF cases were reported exclusively upon laboratory confirmation by molecular biology (RT-PCR), as no official definition of a suspected case had yet been established. Confirmed cases were reported via GoData and registered in theSistema de Informação de Agravos de Notificação(SINAN).
This observational study followed the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement14.
Minas Gerais comprises 853 municipalities distributed over a territorial area of 586,513.984 km² and has an estimated population of 20,539,989 inhabitants as of 2023, making it the second most populous state in Brazil. For administrative and epidemiological purposes, the State Health Department of Minas Gerais (SES/MG) divided the territory into 28 Regional Health Units (RHU) as established by SES/MG Resolution No. 9,224 on December 12, 2023.
Sample and surveillance procedures
Following the detection of OF cases outside the Amazon region in May 2024, the Ezequiel Dias Foundation (FUNED), in collaboration with SES/MG, developed a sampling and laboratory testing protocol to identify potential cases in Minas Gerais. In this study, confirmed cases were strictly defined as individuals with laboratory-confirmed OROV infection by RT-PCR. The inclusion criteria were as follows: (i) residence in Minas Gerais, (ii) availability of complete sociodemographic and clinical data from GoData, and (iii) laboratory confirmation at FUNED. The exclusion criteria included incomplete records or indeterminate RT-PCR results.
Sentinel surveillance of arboviruses will be implemented in June 2024. Based on the initial detection of OROV-positive samples by RT-PCR, the diagnostic investigation was expanded beyond the sampling strategy to include broader local surveillance in the municipalities with identified cases.
Once cases were confirmed, standardized OROV investigation forms were completed in GoData by municipal health teams following the same procedures routinely adopted for other notifiable diseases in Brazil. All information analyzed in this study originated from official surveillance records, which were filled out by local health professionals during the case investigation as part of their public health duties. The authors did not conduct interviews or collect primary data. Rather, they accessed de-identified secondary data extracted from the GoData system, which includes more detailed fields than the standard SINAN notification forms.
Variables
The sociodemographic variables analyzed included sex, age, race/skin color, educational level, municipality of residence, RHU, and area of residence (urban or rural). Clinical variables included the presence of signs and symptoms, symptom duration, date and epidemiological week of symptom onset, symptom recurrence, and the presence of comorbidities. Epidemiological context variables included the presence of animals in the peridomicile, reports on epizootics, and other relevant environmental observations.
Data analysis
Data were exported from GoData in the CSV format and subsequently analyzed using IBM® SPSS 21.0.0.0. Numerical variables are summarized using measures of central tendency (mean or median) and dispersion (standard deviation or interquartile range), according to their distribution. Categorical variables are described as absolute and relative frequencies. Graphs and tables were used to visualize the temporal and spatial trends in OROV cases across Minas Gerais. The incidence rates per 100,000 inhabitants were calculated using the estimated population for Minas Gerais in 2024, published by the Instituto Brasileiro de Geografia e Estatística (IBGE) in Diário Oficial da União on August 29, 2024.
In addition to descriptive statistics, exploratory analyses were conducted to compare the distribution of selected symptoms by sex and age. These symptoms were selected because of their high prevalence and clinical relevance. A chi-square test was used to explore the relationship between the presence of symptoms and sex. Associations between sex and symptoms were estimated using Poisson regression with robust variance to obtain prevalence ratios (PRs) and 95% confidence intervals. For age comparisons, the Mann-Whitney U test was applied (because the data did not present a normal distribution). One patient was excluded from the analysis because of missing information. The Chi-square test was used to assess differences in proportions between groups, as is commonly recommended for categorical data. In addition, PR with 95% confidence intervals was estimated using Poisson regression with robust variance to quantify the magnitude of the associations. All analyses were performed using IBM SPSS Statistics, version 21.0.0.0.
Ethical considerations
This study was approved by the Research Ethics Committee of the Hospital Foundation of the State of Minas Gerais (approval number: 7,399,279). Because it relied exclusively on secondary de-identified data from official surveillance systems, it complied with the principles outlined in Resolution No. 466/2012 of the Brazilian National Health Council, ensuring the confidentiality, privacy, and ethical use of epidemiological information.
RESULTS
In 2024, 278 confirmed cases of OF were reported in Minas Gerais. Most cases were observed in females (55.0%). The mean age of the affected individuals was 40.14 years (SD ± 19.19), with a median age of 40 years (interquartile range [IQR]: 25-56) (Table 1; Figure 1). Most patients self-identified as mixed race (46.8%) or White (32.4%), and over half (54.7%) had completed elementary education.
TABLE 1:Sociodemographic profile of confirmed Oropouche fever cases, Minas Gerais, Brazil, 2024 (N = 278).CharacteristicsConfirmed cases (%) Sex
Female153 (55.0)Male125 (45.0) Race/Color
Asian4 (1.4)White90 (32.4)Mixed-race130 (46.8)Black38 (13.7) Education level
No schooling/Incomplete elementary school103 (37.0)Complete elementary school/Incomplete high school49 (17.6)Complete high school/Incomplete vocational or higher education86 (30.9)Complete technical/vocational or higher education20 (7.2) Regional health unit/Municipality of residence
Barbacena
Congonhas1 (0.4) Coronel Fabriciano
Coronel Fabriciano30 (10.8)Ipatinga3 (1.1)Joanésia140 (50.4)Timóteo15 (5.4) Governador Valadares
Coroaci1 (0.4)Gonzaga1 (0.4) Juiz de Fora
Bom Jardim de Minas1 (0.4)Piau84 (30.2)Ubá Tabuleiro2 (0.7) Residential area
Peri-urban78 (28.1)Rural or sylvatic106 (38.1)Urban74 (26.6)Note: The number of cases in certain categories may vary due to missing information. This table presents the data on cases reported in 2024, extracted from the official surveillance system on February 10, 2025.
FIGURE 1:Confirmed Oropouche fever cases by sex and age group, Minas Gerais, Brazil, 2024 (N = 278). Note: This figure presents the data on cases reported in 2024, extracted from the official surveillance system on February 10, 2025.
Two cases of OF were diagnosed in pregnant women, both in the second trimester and without comorbidities. One resided in Joanésia and the other in Piau. The reported symptoms included fever, headache, myalgia, arthralgia, chills, nausea, vomiting, dysgeusia, ageusia, photophobia, dizziness, pruritus, fatigue, malaise, and ecchymosis. Both patients received regular prenatal care, and no maternal or fetal complications were reported.
The most frequent symptoms among confirmed cases were fever, headache, myalgia/arthralgia, gastrointestinal manifestations, and retroorbital pain (Table 2). Upper respiratory tract symptoms such as nasal discharge, odynophagia, and cough were less common. Dermatological findings included petechiae, ecchymosis, rash, and erythema, whereas gastrointestinal symptoms included nausea, diarrhea, vomiting, and abdominal pain.
TABLE 2:Clinical profile of confirmed Oropouche fever cases, Minas Gerais, Brazil, 2024 (N = 278).CharacteristicsCases (%) Signs and symptoms
Fever231 (83.1)Headache212 (76.3)Myalgia196 (70.5)Gastrointestinal symptoms164 (59.0)Retro-orbital pain140 (50.4)Ageusia137 (49.3)Arthralgia128 (46.0)Chills120 (43.2)Dysgeusia120 (43.2)Dizziness92 (33.1)Fatigue or weakness87 (31.3)Malaise79 (28.4)Back pain77 (27.7)Pruritus76 (27.3)Skin lesions58 (20.9)Photophobia30 (10.8)Flu-like or upper respiratory symptoms28 (10.1)Nuchal pain28 (10.1)Conjunctivitis15 (5.4)Dark urine14 (5.0)Shortness of breath13 (4.7)Oliguria7 (2.5)Jaundice5 (1.8)Sensitivity to touch5 (1.8)Leg pain5 (1.8)Tachycardia2 (0.7) Comorbidities
Hypertension65 (23.4)Diabetes28 (10.1)Heart disease6 (2.2)Lung disease (chronic obstructive pulmonary disease, asthma, tuberculosis)5 (1.8)Hematological diseases3 (1.1)Chronic kidney disease2 (0.7) Note: This table presents the data on cases reported in 2024 extracted from the official surveillance system on February 10, 2025.
The temporal distribution of cases demonstrates two distinct peaks in epidemiological weeks 15 and 50 in 2024 (Figure 2). These peaks coincided with the detection of outbreaks in Joanésia and Piau, municipalities with the largest number of confirmed cases during the study period.
FIGURE 2:Confirmed OF cases by epidemiological week of symptom onset, Minas Gerais, Brazil, 2024 (N = 278). Note: This figure presents the data on cases reported in 2024, extracted from the official surveillance system on February 10, 2025.
The mean symptom duration was 6.77 days (SD ± 5.25), with a median of 5 days (IQR, 4-7). Symptom recurrence was reported in 71 cases (25.5%), with an average time of reappearance of 9.88 days (SD ± 13.57) and a median of 5 days (IQR: 3-10).
The most frequent comorbidities among the confirmed cases were hypertension (23.4%) and diabetes mellitus (10.1%) (Table 2). Other comorbidities were less common and included chronic respiratory diseases (COPD, asthma, or tuberculosis), cardiovascular conditions, hematologic disorders, chronic kidney disease, leprosy, dyslipidemia, gastritis, depression, anxiety, migraines, hypothyroidism, and musculoskeletal disorders.
The largest clusters of cases observed in the state were located in the municipalities of Joanésia (n = 140) and Piau (n = 84). The neighboring municipalities also reported confirmed cases, although in smaller numbers (Figure 3).
FIGURE 3:Spatial distribution of incidence per 100,000 inhabitants of confirmed Oropouche fever cases by municipality of residence, Minas Gerais, Brazil, 2024. Notes: Thicker lines indicate the boundaries of regional health units (RHU), whereas thinner lines represent municipal limits. This figure presents the data on cases reported in 2024, extracted from the official surveillance system on February 10, 2025.
Ultimately, 144 individuals (51.8%) reported the presence of domestic or livestock animals in their households, workplaces, or study environments. Dogs were most frequently mentioned (126), followed by chickens (54), cattle (48), horses (38), cats (37), ducks (2), bees (1), goats (1), and pigs (1). In addition, 13 notifications (5.1%) included reports of non-accidental deaths of sylvatic or peridomestic animals (such as monkeys, birds, armadillos, anteaters, and sloths) near areas of residence or work.
An exploratory analysis was performed to compare the frequencies of key symptoms and selected clinical features between female and male patients. Fever was highly prevalent in both groups; however, the difference was not statistically significant. However, headaches (83.6% vs. 68.0%, p < 0.01), myalgia (76.3% vs. 64.0%, p < 0.05), and gastrointestinal symptoms (65.1% vs. 52.0%, p < 0.05) were significantly more frequent in females. Dysgeusia (52.0% vs. 32.8%, p < 0.01), pruritus (35.5% vs. 16.6%, p < 0.01), and skin lesions (28.3% vs. 12.0%, p < 0.01) were more common in females. The detailed results are provided in Supplementary Table S1.
TABLE S1:Clinical profile of confirmed Oropouche fever cases by sex, Minas Gerais, Brazil, 2024 (N = 277).Signs and symptoms Female (n = 152)
Male (n = 125) X^2^ Prevalence ratio (95% CI)Fever (%)130 (85.5)101 (80.8)1.1060.94 (0.85-1.05)Headache (%)127 (83.6)85 (68.0)9.2380.81 (0.71-0.94)Myalgia (%)116 (76.3)80 (64.0)5.0280.84 (0.72-0.98)Gastrointestinal symptoms (%)99 (65.1)65 (52.0)4.8970.80 (0.65-0.98)Retro-orbital pain (%)82 (53.9)58 (46.4)1.5630.86 (0.68-1.09)Ageusia (%)80 (52.6)57 (45.6)1.3570.87 (0.68-1.11)Arthralgia (%)71 (46.7)57 (45.6)0.0340.98 (0.76-1.26)Chills (%)68 (44.7)52 (41.6)0.2750.93 (0.71-1.22)Dysgeusia (%)79 (52.0)41 (32.8)10.2700.63 (0.47-0.85)Dizziness (%)53 (34.9)39 (31.2)0.4160.89 (0.64-1.26)Fatigue or weakness (%)49 (32.2)38 (30.4)0.1070.94 (0.66-1.34)Malaise43 (28.3)36 (28.8)0.0091.02 (0.70-1.48)Back pain42 (27.6)35 (28.0)0.0051.01 (0.69-1.48)Pruritus54 (35.5)22 (16.6)11.0710.50 (0.32-0.77)Skin lesions43 (28.3)15 (12.0)10.9940.42 (0.25-0.73)Photophobia22 (14.5)8 (6.4)4.630*0.44 (0.20-0.96)Flu-like or upper respiratory symptoms18 (11.8)10 (8.0)1.1140.68 (0.32-1.41)Nuchal pain16 (10.5)12 (9.6)0.0650.91 (0.45-1.86)Conjunctivitis10 (6.6)5 (4.0)0.8910.61 (0.21-1.73)Dark urine7 (4.6)7 (5.6)0.1411.22 (0.44-3.37)Shortness of breath7 (4.6)6 (4.8)0.0061.04 (0.36-3.02) Note: This table presents data on cases reported in 2024 extracted from the official surveillance system on February 10, 2025. * p-value < 0.05, ** p-value < 0.01, *** p-value < 0.001
The same key symptoms considered in the analysis of female and male patients were considered in the evaluation of possible age-related differences. Only patients with retroorbital pain had a significantly lower median age (37 vs. 44 years, U = 10,971; p = 0.038). No statistically significant differences were reported in other signs and symptoms.
In addition, isolated reports of fainting, ageusia, burning sensation, confusion, facial edema, hematemesis, erythematous itchy lesions, rib pain, altered taste perception, drowsiness, swelling, paresthesia in the extremities, tremors, arrhythmia, leg fatigue, blurred vision, palpitations, dysuria, and listlessness were reported.
DISCUSSION
The findings of this study highlighted the occurrence of OF outbreaks in Minas Gerais by 2024. This investigation fills an important gap in the epidemiological literature, as OROV infection has historically been restricted to the Amazon region, but has recently expanded to other areas of Brazil7 ^-^ 9, representing an emerging public health challenge12.
Several factors likely contribute to the geographic expansion of OROV beyond the Amazon basin, including the increasing distribution of vector species1 ^,^ 4 ^,^ 7, climatic and environmental changes6 ^-^ 9, human and animal migration4 ^,^ 9, underreporting and diagnostic confusion with other arboviruses6 ^,^ 15 ^-^ 17, urbanization, and socioeconomic vulnerabilities7 ^.^ 9. In 2024, autochthonous cases were reported in all 27 federative units of Brazil, spanning the northeast, southeast, central-west, and southern regions12, underscoring the nationwide spread of the virus.
In Minas Gerais, more cases have been reported among females than males, with a broad age distribution, predominantly among young adults. The literature does not indicate a consistent sex- or age-related pattern of infection, though Scachetti et al. (2024) found that individuals aged 20-59 years, regardless of sex, presented the highest incidence rates compared to the national cumulative incidence of 5.22 cases per 100,000 inhabitants.
Spatial analysis revealed a bimodal distribution of cases in the two municipalities, with Joanésia showing a peak around epidemiological week 15, and Piau around week 50 in 2024. The predominance of cases in rural and peri-urban areas suggests that transmission is associated with ecologically favorable environments for vector proliferation, despite the urbanized landscape of the state. Culicoides paraensis, the primary vector, thrives in humid habitats rich in decomposing organic matter such as banana or cacao debris4. Similar patterns have been described in Iquitos, Peru, where peri-urban transmission cycles have been identified, and most OROV isolates were obtained from rural and suburban areas18.
The temporal distribution of cases observed in this study indicated possible seasonal transmission, consistent with increased vector reproduction in humid or flooded environments, coinciding with the rainy season in the Minas Gerais6 ^,^ 12 ^,^ 19 ^,^ 20. These findings highlight the need for continuous entomological surveillance and predictive models that integrate climatic and ecological data.
Clinically, fever, headache, myalgia, and retro-orbital pain were the most frequently reported symptoms, which is in agreement with the findings from other endemic areas. The occurrence of symptom recurrence in over one-quarter of the cases is noteworthy, suggesting that OROV infection may have a prolonged impact on patient well-being and productivity. Comorbidities such as hypertension and diabetes are common and may influence both the course and perception of illness.
The clinical presentation of OF is non-specific and overlaps with that of other arboviral infections, complicating the differential diagnosis. Studies have described a wide spectrum of symptoms, including fever, headache, myalgia, arthralgia, chills, dizziness, photophobia, nausea, vomiting, rash, and conjunctivitis1 ^,^ 7 ^,^ 8 ^,^ 21 ^,^ 22. Although typically self-limiting, OF can occasionally progress to neurological involvement such as meningitis or meningoencephalitis2 ^,^ 3 ^,^ 12 ^,^ 23. In the present study, no severe neurological manifestations were observed in confirmed cases.
With regard to pregnancy, the two confirmed cases evolved without complications. Although the vertical transmission of OROV is rare, it has been documented in the literature, including reports of fetal death and congenital anomalies3, underscoring the importance of monitoring this group in future investigations.
The high proportion of individuals who reported contact with domestic or livestock animals raises the hypothesis that environmental factors contribute to viral maintenance or amplification. Furthermore, reports of wildlife deaths, although limited, warrant further investigation into the possible role of sylvatic vertebrates as reservoirs or sentinels in OROV transmission cycles4 ^,^ 5.
This study had certain limitations that should be considered when interpreting the findings. The dependence on surveillance notifications and laboratory confirmations may underestimate the true incidence of OROV infection. In addition, spatial differences in testing availability and health infrastructure could have influenced case distribution. Nevertheless, this investigation has significant strengths, including the detailed clinical, epidemiological, and spatial characterization of OROV cases in non-endemic regions.
These results provide valuable insights into the ongoing expansion of Oropouche fever in Brazil and highlight the need for strengthened surveillance systems, differential diagnostic capacities, and integrated vector control strategies. Furthermore, the evidence generated contributes to the understanding of the social and environmental determinants of OROV transmission and supports the development of effective public health policies to mitigate its spread.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Andreolla AP Borges AA Nagashima S Vaz de Paula CB de Noronha L Zanchin NIT Development of monoclonal antibodies against oropouche virus and its applicability to immunohistochemical diagnosis Virol J 202421811133858989610.1186/s 12985-024-02323-z PMC 11000289 · doi ↗ · pubmed ↗
- 2Murillo JL Cabral AD Uehara M Silva VM Santos JV Muniz JRC Nucleoprotein from the unique human infecting Orthobunyavirus of Simbu serogroup (Oropouche virus) forms higher order oligomers in complex with nucleic acids in vitro Amino Acids 20185067117212962630110.1007/s 00726-018-2560-4 · doi ↗ · pubmed ↗
- 3Martins-Filho PR Carvalho TA Santos CA Oropouche fever: reports of vertical transmission and deaths in Brazil Lancet Infect Dis 20242411 e 662e 6633918250010.1016/S 1473-3099(24)00557-7 · doi ↗ · pubmed ↗
- 4Romero-Alvarez D Escobar LE Oropouche fever, an emergent disease from the Americas Microbes Infect 20182031351462924771010.1016/j.micinf.2017.11.013 · doi ↗ · pubmed ↗
- 5Grisales-Nieto JC Luz SLB Nascimento VA Naveca FG Murcia-Montaño LM Romero-Vesga KN First case of Oropouche fever detected in the international border region of the Colombian Amazon: clinical characteristics and molecular diagnosis Mem Inst Oswaldo Cruz 2024119 e 2302213874785510.1590/0074-02760230221 PMC 11095112 · doi ↗ · pubmed ↗
- 6Pereira RS Colangelo JF Souza PGA Carvalho LGF da Cruz Nizer WS Lima WG Epidemiological aspects of the Oropouche virus (Orthobunyavirus) in South America: A systematic review Rev Colomb Cienc Quim Farm 2022511166184
- 7Lima RC Dias HG Souza TMA Familiar-Macedo D Ribeiro ED Corrêa VC Oropouche Virus Exposure in Febrile Patients during Chikungunya Virus Introduction in the State of Amapá, Amazon Region, Brazil Pathogens 20241364694693892176710.3390/pathogens 13060469 PMC 11206884 · doi ↗ · pubmed ↗
- 8Vasconcelos HB Azevedo RSS Casseb SM Nunes-Neto JP Chiang JO Cantuária PC Oropouche fever epidemic in Northern Brazil: Epidemiology and molecular characterization of isolates J Clin Virol 20094421291331911779910.1016/j.jcv.2008.11.006 · doi ↗ · pubmed ↗