Relearning the epistemology, history, and future of neuropsychiatry
Juan Camilo Castro Martínez, Felipe Botero-Rodríguez, Jesús Ramírez-Bermúdez, Vaughan Bell, Gabriel Oviedo-Lugo, José Manuel Santacruz-Escudero, Ángela Iragorri, Joan Camprodon, Brian Lawlor, Hernando Santamaría-García

TL;DR
This paper reviews the history and future of neuropsychiatry, proposing a new framework that integrates brain, body, and subjective experience.
Contribution
The paper introduces a renewed paradigm for neuropsychiatry emphasizing dimensional research and lived experience integration.
Findings
A historical analysis reveals persistent tensions in conceptualizing neuropsychiatric symptoms.
A new paradigm is proposed using dimensional frameworks and integrative models.
Education and clinical reforms are suggested to enhance interdisciplinary collaboration.
Abstract
Neuropsychiatry is a transdisciplinary field at the intersection of neuroscience, psychiatry, neurology, and humanities. Despite this strategic position, a comprehensive framework is still needed to bridge these domains. This review examines the historical evolution of how neurological, mental, and neuropsychiatric symptoms have been conceptualized, from antiquity to contemporary models, using the brain–body dilemma as a guiding thread. This historical analysis provides the epistemological and ontological foundations of neuropsychiatry, which are then connected with current definitions to critically assess the field's persistent tensions. Building on this foundation, a renewed paradigm is proposed where a crosstalk between them is enabled, grounded in deep phenotyping, dimensional research frameworks [e.g., Research Domain Criteria (RDoC), Hierarchical Taxonomy of Psychopathology…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
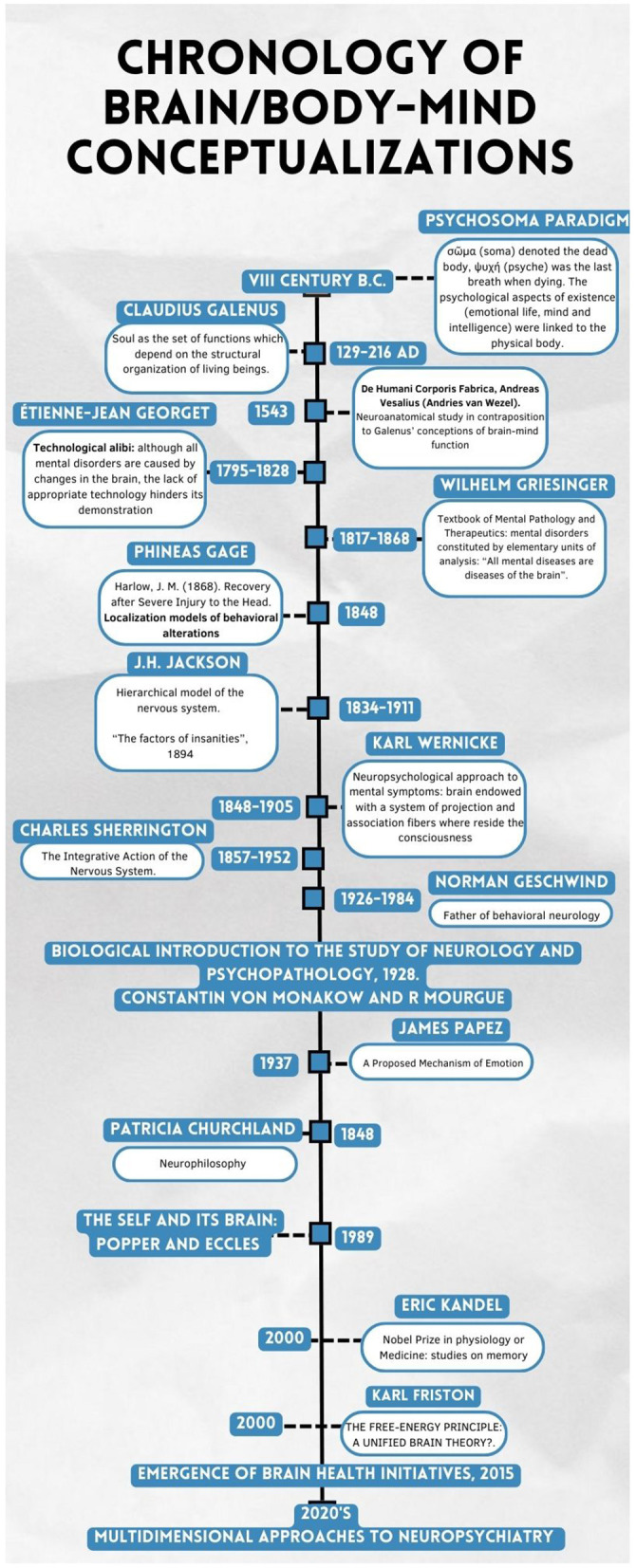 Figure 1
Figure 1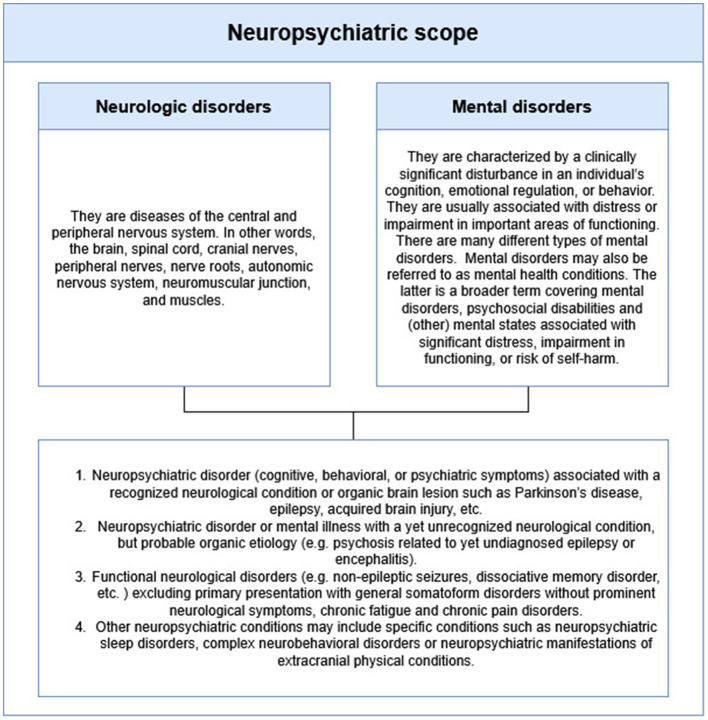 Figure 2
Figure 2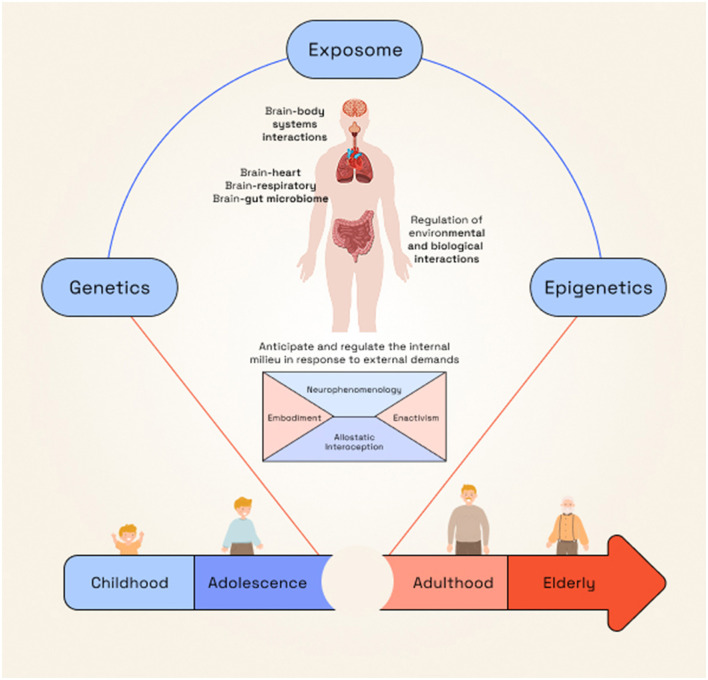 Figure 3
Figure 3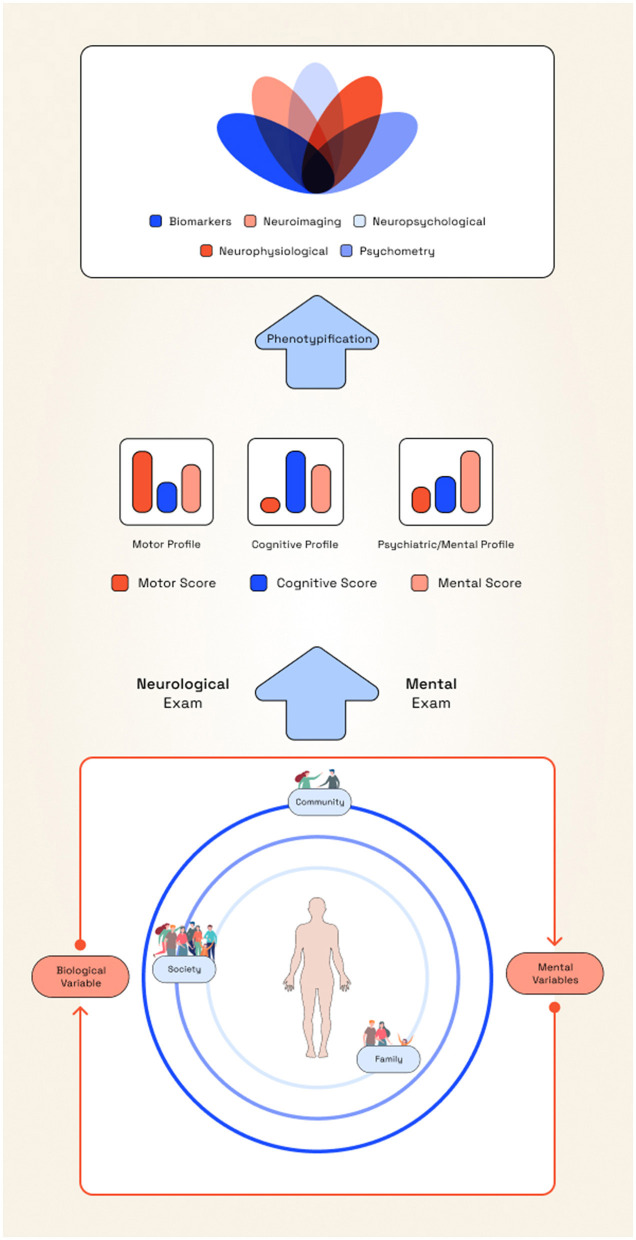 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMental Health and Psychiatry · Historical Psychiatry and Medical Practices · Neurology and Historical Studies
Introduction
Neuropsychiatry is a discipline at the crossroads of medicine, neurology, psychiatry, neuroscience, psychology, physiology, phenomenology, and philosophy. It investigates behavioral abnormalities, cognitive dysfunction, and mental symptoms in neurological and somatic conditions, while also advancing neurobiological explanations of psychiatric disorders (Berríos, 2007). Yet, defining its scope remains difficult (Sachdev P. S., 2005; Berríos, 2007; Poole and Bolton, 2020), and it is often described as a “no man's land” between neurology and psychiatry (Sachdev P. S., 2005).
Neuropsychiatric disorders are highly prevalent and rank among the leading global causes of disease burden (Nichols et al., 2019; Ferrari et al., 2022; Steinmetz et al., 2024). Conditions such as stroke, migraine, dementias, epilepsy, and autism account for significant disability-adjusted life-years (DALYs; Steinmetz et al., 2024), and depressive and anxiety disorders, including somatic equivalents like pain and insomnia, rank among the top contributors to DALYs worldwide (Ferrari et al., 2022). Their impact extends beyond tissue damage, affecting cognitive, affective, behavioral, social, and functional domains.
Despite progress, neuropsychiatry faces persistent theoretical and pragmatic challenges, including a lack of consensus on the study and care of affected patients, and the absence of a unified praxis or epistemological framework (Ramirez-Bermudez et al., 2017). In part, this is based on the epistemological difficulties encountered in psychiatry, where the object of study is defined by complex interplay between social, political, historical processes and folk psychology dynamics (Berrios and Marková, 2018). Parting from that point, neuropsychiatry puts forward a critical point, the need for dialogical bridges to give responses to clinical and research questions. These gaps have led to fragmented clinical and research approaches, shaped by enduring tensions surrounding the body–mind problem (Thibaut, 2018).
This paper offers an overview of neuropsychiatry: the historical evolution of symptom conceptualization describing the tensions between mental and neurologic symptoms both at epistemological and ontological levels; its epistemological bases, current definitions, and future directions. Although these developments are presented sequentially to support the subsequent epistemological discussion, such structure does not imply a linear or cumulative progression of knowledge, which often unfolds through non-continuous and contingent processes (De Domenico et al., 2016). This review highlights shifts in neurological and mental concepts, the persistence of the mind–body dilemma, and the role of philosophy and technology in shaping research and care. Finally, we discuss challenges in clinical, academic, and training contexts, proposing an integrative orientation aimed at translating neuroscientific knowledge and subjective understanding into innovative practice.
Historical background of mental and neurological symptoms
It is important to acknowledge at the outset that the historical literature most relevant to neuropsychiatry is underdeveloped, although some general aspects of its historical development can be discerned (Scull, 2017). In ancient Greece, neurologic and psychiatric symptoms were viewed as a single domain. Guided by the Hippocratic humoral theory, behavior and mental states were interpreted as manifestations of bodily imbalance (Trimble, 2016). In the 16th century, Andreas Vesalius and Thomas Willis re-anchored mind and behavior in brain biology, although humoral and ventricular doctrines persisted (Trimble, 2016). The 17th century brought systematic case descriptions by Thomas Sydenham and René Descartes' substance dualism, which formalized the mind–body split still echoing in today's debates (Trimble, 2016; Thibaut, 2018). Willis emphasized brain matter over ventricles and proposed “animal spirits” as mediators of mental life (Trimble, 2016). John Locke reframed mental symptoms as cognitive phenomena (Trimble, 2016), and Karl Jaspers later established phenomenological psychopathology, stressing first-person experience (Park, 2019).
By the late 19th century, figures such as Emil Kraepelin and Jean-Martin Charcot contributed to the institutional consolidation of psychiatry and neurology as distinct disciplines; however, this divide cannot be attributed solely to their work: Kraepelin through classification systems grounded in psychopathology (Heckers et al., 2022), and Charcot through the anatomo-clinical method, correlating clinical signs with post-mortem findings (Drouin et al., 2022). Yet, the divide was not absolute; neurology remained highly influential for the development of modern psychiatry from alienism (Bogousslavsky and Moulin, 2009), and scholars like Hughlings Jackson proposed hierarchical models of brain function, emphasizing integration rather than localization (Martin, 2002; Trimble, 2016). Furthermore, there were notable alienists who contributed to the study of the nervous system, effectively serving as early “neuropsychiatrists,” such as Baillarger and Lasègue (Bogousslavsky and Moulin, 2009).
The early 20th century saw major advances in neurobiology by Santiago Ramón y Cajal, Franz Nissl, and Alois Alzheimer, alongside a growing specialization in medicine, particularly in the US (Goetz et al., 2003). Clinicians increasingly distinguished between cases with clear neuropathology and those with primarily behavioral symptoms (Tyler et al., 2003).
French scholars countered this emerging binary. Paul Lhermitte and Julian de Ajuriaguerra promoted body–mind unity, while Henri Ey proposed a hierarchical model linking localized (neurological) and global (psychiatric) disintegration (Drouin et al., 2022). Nonetheless, France abolished neuropsychiatry in 1968 amid psychodynamic and sociopolitical pressures (Drouin et al., 2022). In contrast, Alexander Luria advanced a synthesized neuropsychological model (Peña-Casanova et al., 2024), and Germany retained combined training (Drouin et al., 2022).
Global conflicts, particularly World War I and II, catalyzed the recognition of combat-related mental and neurological conditions, advancing their conceptualization and care. During World War I, the US Army created neuropsychiatric units at the front lines, marking the first formal use of the term neuropsychiatry in 1917 (Crocq and Crocq, 2000; AMEDD Center of History and Heritage, n.d.). These developments laid the foundation for specialized battlefield care and institutional frameworks. In 1933, the American Board of Psychiatry and Neurology (ABPN) was founded to certify training in neurology, psychiatry or both in the US (Benjamin, 2024). After World War II, however, the trend shifted toward specialization, as the World Health Organization (WHO) and the World Psychiatric Association (WPA) endorsed separating neurology and psychiatry into distinct disciplines in 1963 and 1966, respectively (Estingoy, 2019).
The first edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) in 1952 categorized psychiatric conditions as either organic or non-organic (Fischer, 2012). Psychiatry's alliance with psychoanalysis widened the gap (Berrios and Marková, 2002). This is also reflected in the decreased of dual-boarded neuropsychiatrists observed after the creation of the ABPN, especially in the 60's and 70's (Benjamin, 2024).
The 1980s reopened integration. DSM-III adopted an atheoretical, symptom-based approach (Wilson, 1993; Fischer, 2012). The American Neuropsychiatric Association (ANPA, 1988) and UK neuropsychiatric centers, staffed by dual-trained physicians, created a clinical “third space” (Coffey, 1999). In parallel, the British Neuropsychiatry Association (BNPA, 1987) was founded to promote interdisciplinary dialogue among psychiatrists, neurologists, neuropsychologists, and other neuroscience professionals interested in brain–behavior relationships (Agrawal et al., 2015; Bhattacharya et al., 2015).
Parallel advances in cognitive science and neuroimaging reframed many psychiatric disorders as brain-based (Bolton, 2013; Tian et al., 2023). Yet, as Eric Kandel noted, articulating a model intelligible to both neuroscientists and psychiatrists remains the core challenge (Kandel, 1998). Despite this progress, the development of neurodiagnostic tools and academic structures continues to reinforce separation, perpetuating a dualistic paradigm that still hinders interdisciplinary integration (Tyler et al., 2003; Thibaut, 2018).
Since the early 2000s, technology and large-scale research initiatives have reshaped the neuropsychiatric landscape, helping bridge neurology and psychiatry. Functional MRI (fMRI), PET, SPECT, and high-resolution MRI have mapped brain activity with unprecedented precision (Tu et al., 2021; Tozzi et al., 2024). These tools have revealed overlapping neural circuits implicated in both psychiatric and neurological conditions (Tu et al., 2021).
The Human Connectome Project and other large-scale neuroimaging studies have standardized multimodal brain mapping, showing how traditionally “psychiatric” and “neurological” disorders affect common neural pathways (Thompson et al., 2020; Tu et al., 2021). Computational psychiatry has begun to integrate multi-level perspectives of neuropsychiatric disorders (Castro Martínez and Santamaría-García, 2023).
Genetic imaging consortia, such as ENIGMA and PsychENCODE, have identified polygenic overlaps between epilepsy, schizophrenia, and bipolar disorder (Thompson et al., 2020), reinforcing the convergence of psychiatric and neurological disease architectures. Conceptual models such as the Research Domain Criteria (RDoC) and Hierarchical Taxonomy of Psychopathology (HiTOP) frameworks further encourage a dimensional, brain-behavior-based understanding of mental illness (Michelini et al., 2021). Digital phenotyping through smartphones and wearable technologies now offers real-time behavioral markers that can inform diagnosis and relapse prediction in both mood and seizure disorders (Onnela and Rauch, 2016).
Contemporary neuropsychiatry increasingly integrates connectomic models with active inference frameworks (Friston et al., 2017) and constructivist approaches to behavior and mind (Barrett, 2017) reflecting a paradigm shift toward multiscale, embodied perspectives. These models converge on the idea that mental functions emerge from complex, dynamic patterns of brain connectivity rather than isolated regions. At the same time, they emphasize that cognition, emotion, and behavior are constructed from the interplay between neural architecture, bodily biology (e.g., inflammation, autonomic, and metabolic systems), and contextual interactions with the world. This integrated perspective moves beyond reductionist, dualistic models, highlighting how mind and psychopathology arise from distributed, brain–body–environment systems (Santamaría-García et al., 2024).
Rather than offering a chronological account of neuropsychiatry as a discipline, the preceding section traced how mental and neurological symptoms have been framed across time, highlighting the cultural and scientific influences that shaped their meaning and exposed enduring conceptual tensions. Some caveats must be mentioned as this description is linear since it is not the aim of the review to give a thorough historical recount but to give a succinct recount of how the object of study of neuropsychiatry has been shaped by historical processes involving cultural factors and philosophical currents. This historical lens provides the basis for reexamining the epistemological foundations and ontological concepts of neuropsychiatry, enabling a better understanding of neuropsychiatry as previously Berríos and Markova have stated that this understanding requires an understanding of the history and the idiographic needs (Berrios and Marková, 2024).
Unraveling definitions, global variations, and debates in neuropsychiatry
The evolving conceptions of the brain–mind relationship continue to shape epistemological practices in neurology, psychiatry, and neuropsychiatry by mediating at the same time the ontology (Figure 1), influencing how disciplinary boundaries are drawn. Philosophical divergences historically contributed to separating neurological from mental symptoms, whereas moments of convergence fostered a “third space” connecting them. Building on these ideas, this section reviews contemporary definitions of neuropsychiatry to clarify its epistemological scope and present-day challenges (Poole and Bolton, 2020).
Chronology of brain/body-mind conceptualizations as a means to understand neuropsychiatry. Key milestones in the framing of neurological and psychiatric symptoms. This historical overview highlights enduring tensions in the brain–body–mind relationship that continue to shape neuropsychiatry.
The International Neuropsychiatric Association defines neuropsychiatry as “a field of scientific medicine that concerns itself with the complex relationship between human behavior and brain function, and endeavors to understand abnormal behavior and behavioral disorders based on an interaction of neurobiological and psychological–social factors” (Sachdev P., 2005). This positions neuropsychiatry as a broad scientific domain, rather than a purely clinical specialty, focused on behavior–brain interactions and mind–body interfaces.
ANPA, in turn, describes neuropsychiatry as both a scientific field and clinical subspecialty targeting mental disorders linked to nervous system disease (Sachdev and Mohan, 2017). The Joint Committee on Subspecialty Certification of the ANPA and the Society for Behavioral and Cognitive Neurology (SBCN) have explicitly stated the core philosophical position that brain and behavior are inseparable by merging historically separate but parallel disciplines of behavioral neurology and neuropsychiatry into one subspecialty (Arciniegas and Kaufer, 2006). This medical subspecialty aims to improve understanding of the links between neuroscience and behavior and to advance the care of individuals with neurologically based behavioral impairments (Arciniegas and Kaufer, 2006).
Globally, neuropsychiatry's structure varies, however, there is an agreement of insufficient integration at training (Molina-Ruiz et al., 2024). In the US, dual training programs in psychiatry and neurology and formal fellowships have made it a leading center for neuropsychiatric research and practice (Arciniegas and Kaufer, 2006; Benjamin, 2024). In Australia and New Zealand, neuropsychiatry services are based in tertiary hospitals and focus on epilepsy, neurodevelopmental disorders, traumatic brain injury, and Huntington's disease. Care often includes multidisciplinary approaches with neurostimulation and rehabilitation, and telehealth is used to reach remote areas (Finucane et al., 2020).
In Europe, the field is more heterogeneous. In France, Henry Ey's organo-dynamic model (Drouin et al., 2022) and sociopolitical movements led to the dissolution of neuropsychiatry and the establishment of separate neurology and psychiatry tracks (Estingoy, 2019; Drouin et al., 2022). Germany, in contrast, retained a unified discipline (“Nervenheilkunde”) and strong ties to psychosomatic medicine (Northoff, 2008). The UK maintained neuropsychiatry services rooted in the work of Hughlings Jackson and W. A. Lishman, including master's-level training and extensive research on care models (Agrawal et al., 2015; Bhattacharya et al., 2015).
In Japan, the aging population has driven development in neuropsychiatry with significant overlap with geriatric psychiatry (Miyoshi, 2020). Academic neuroscience in Japan has linked neurological and psychiatric research, with contributions on the behavioral effects of environmental exposures like heavy metals.
In many Low- and Middle-Income Countries (LMICs), neuropsychiatry lacks formal institutional support. In Southeast Asia, training is limited to high-complexity centers and often consists of cross-specialty placements between neurology and psychiatry (Krishnamoorthy and Misra, 2020). Despite this, recovery-oriented programs emphasizing cultural and functional adaptation and psychosocial support have emerged (Krishnamoorthy and Misra, 2020). In Latin America, Argentina and Mexico have had neuropsychiatry advances as collaborations among behavioral neurology institutes and academic centers (Ramirez-Bermudez et al., 2017; Slud Brofman and Brusco, 2020). In general, in LMICs, neuropsychiatric expertise has developed within consultation–liaison and clinical neuroscience models, often focused on dementia diagnostics, functional neurologic disorder clinics, epilepsy and movement disorders programs (Krishnamoorthy and Misra, 2020; Slud Brofman and Brusco, 2020).
Beyond clinical and organizational variations, fundamental ontological debates remain central to neuropsychiatry. These debates, rooted in longstanding questions about the mind–body relationship, shape how neuropsychiatry defines its scope, methods, and prospects for integration. Mind–body substance dualism, the philosophical view that mental phenomena are ontologically distinct from physical processes, has profoundly shaped psychiatry and neurology by historically encouraging the separation of mental disorders from neurological disease. The nature of the relationship between these ontological domains remains contested (Berrios, 2018; Thibaut, 2018).
Materialism posits that mental phenomena must ultimately be explained or reduced to physical processes (Poole and Bolton, 2020), identifying neurobiological substrate as the necessary level of explanation for apparently mental phenomena (Van Oudenhove and Cuypers, 2010). Eliminative materialism additionally argues that mental constructs are incoherent folk concepts that will eventually be eliminated with neuroscience as the sole viable level-of-explanation for experience and behavior (Churchland, 1981). These reductionist and eliminativist approaches are hard to reconcile with the need to deal with lived experience as it presents clinically and so their applicability to psychiatry remains limited. Interactionist approaches (Berrios, 2018), recognizing both brain-mind and mind-brain causality, and patchy reductionism (Kendler, 2005), where mental phenomena can be partially reduced to biological mechanisms in some domains, while in others, requiring irreducibly psychological or social explanations, are more widely cited as a fruitful philosophical basis for neuropsychiatry.
A substantial portion of ontological reflection concerns the nature of the mind itself. Functionalism conceptualizes mental states as functional systems defined by the relations among mental functions. While grounded in physical structures, the emphasis lies on the organization and interdependence of functional relations (Levin, 2023), highlighting their relational character (Van Oudenhove and Cuypers, 2010) and dependence on physical substrates. Epiphenomenalism also acknowledges such dependence but conceives mental symptoms as secondary by-products of brain activity, lacking causal influence (Van Oudenhove and Cuypers, 2010). In contrast, emergentism grants mental states an autonomous causal powers, beyond mere dependence, allowing them to influence physical domains (Kim, 1999; Van Oudenhove and Cuypers, 2010). Other positions, such as Hughlings Jackson's parallelist perspective, deny any interaction between mental and physical domains (Berrios, 2018), challenging the possibility of integrating neurology and psychiatry (Pies, 2005).
Beyond these ontological debates, neuropsychiatry's epistemological foundations draw on diverse philosophical and scientific traditions. Naturalized epistemologies view neuropsychiatric knowledge as grounded in empirical and neuroscientific investigation, assuming that understanding of mental phenomena arises from biological observation and experimentation (Northoff, 2022; Ramírez-Bermúdez et al., 2024). In contrast, constructivist and critical epistemologies highlight that concepts such as mental disorder or brain dysfunction are historically and socially mediated, shaped by prevailing paradigms rather than discovered as fixed entities (Slade, 2012). Hermeneutic and phenomenological traditions further emphasize the experiential and interpretive dimensions of clinical understanding (Parnas et al., 2013; Aragona and Marková, 2015). Pluralistic and non-reductive epistemologies argue that metaphysical, phenomenological, and ethical dimensions cannot be disentangled from the study of brain–behavior relationships (Northoff, 2014).
The interplay between ontological and epistemological dimensions is especially evident in the study of mental symptoms within neuropsychiatry. Addressing this interdependence requires an integrative framework capable of accommodating complexity, dynamism, and multilevel and transdisciplinary explanations in both neurological diseases and mental disorders. Several challenges must be met to ensure translational validity: the problem of contested concepts, which requires the neurobiopsychosocial model to adopt a truly systemic perspective that bridges the diverse cultures of psychiatry; the inherent complexity of mental symptoms; and the value-ladenness embedded in their interpretation (Fulford et al., 2014). Consequently, it is essential to acknowledge the continuum between empirical sciences and philosophy, fostering an enriched dialogue that supports the development of renewed conceptualizations (Klar, 2021).
Contemporary neuropsychiatry, challenges and pitfalls
While international and national associations have contributed to defining and expanding neuropsychiatry, refining epistemological and clinical approaches across neuroscience, psychiatry, and neurology (Berrios and Marková, 2002; Bhattacharya et al., 2015), key limitations persist. Considering neuropsychiatry, and psychiatry more broadly, solely as a branch of medicine constrains the potential for a contextualized understanding of mental symptoms, which extends beyond statistical correlations of proxy variables (Berrios and Marková, 2024).
Despite a growing conceptual overlap between mind and brain functions, integration between neurology and psychiatry remains incomplete (Martin, 2002; Pies, 2005). This reflects limitations in current conceptual heuristics, which inadequately capture the complexity of mental symptoms, particularly their pleiotropic and heterogeneous nature (McGorry et al., 2025). Furthermore, the persistent difficulty in achieving a shared ontological understanding of mental symptoms across disciplines generates parallel epistemological approaches, producing disparate narratives that hinder deeper integration and compromise translational validity (Fulford et al., 2014). These issues underscore the need for a constructivist epistemic framework that can offer coherence without presupposing a single reductive ontology.
Clinical practice continues to reflect this dualism, although training environments have shown increased convergence, albeit without a distinct neuropsychiatric curriculum (Molina-Ruiz et al., 2024). Neurological and psychiatric conditions share a substantial disease burden (Nichols et al., 2019; Ferrari et al., 2022; Steinmetz et al., 2024), and their comorbidities are poorly quantified and insufficiently addressed, impairing efforts to provide unified care and accurately assess the full impact on quality of life and disease progression (Taslim et al., 2024).
Neurology relies on structured diagnostic certainty and algorithmic frameworks (Graus et al., 2016, 2021), which, while effective for many disorders, remain limited in conditions such as autoimmune psychosis (Pollak et al., 2020) or neuropsychiatric lupus (Emerson et al., 2023). Psychiatry, by contrast, is anchored in symptom-based nosology, yielding broad categories that fail to identify specific endophenotypes or neurobiologically distinct subtypes (Stephan et al., 2016). This disjunction is reinforced by high rates of comorbidity, without adequate models to determine whether these reflect shared mechanisms, causal interactions, or diagnostic overlap (Hesdorffer, 2016). Consequently, neuropsychiatry often lacks a conceptual bridge between symptom-based classification and neural models of dysfunction (Taslim et al., 2024).
The theoretical disjunction between disciplines is thus echoed in clinical practice, giving rise to two parallel and only partially integrated models of care: managing psychiatric symptoms in neurological patients, which dominates current services; and addressing neurological contributions to psychiatric illness, which is less common and under-resourced (Lykouras and Douzenis, 2008; Tian et al., 2023). These practices remain siloed within health systems, facing heterogeneous development and structural barriers across countries (Agrawal et al., 2015; Bhattacharya et al., 2015), particularly at the outpatient level (Agrawal et al., 2015).
The absence of approaches linking neurobiological variables with contextual and psychosocial factors undermines the translational potential of clinical neuroscience (Satel and Lilienfeld, 2014). Studies in this area disproportionately originate from high-income countries (HICs), limiting their global applicability. Psychosocial influences on aging and disease processes are well documented (Santamaría-García et al., 2021), yet remain underrepresented in neuropsychiatric models. “One-size-fits-all” frameworks fail to account for local variability, particularly in the Global South (Greene et al., 2022; Baez et al., 2023). In addition, subjective processes, such as meaning-making and identity, remain insufficiently incorporated into diagnostic and treatment paradigms (Ibáñez et al., 2023).
Neuropsychiatry still lacks a comprehensive integrative orientation. Although neurobiopsychosocial models are frequently invoked (Bolton, 2013), they rarely translate into multilevel, complexity-informed clinical tools. Methodological constraints, small sample sizes, and insufficient analytic depth limit current integrative approaches (Ibanez and Zimmer, 2023; Wu et al., 2023).
Finally, fragmentation in training exacerbates previously mentioned issues. Most neuropsychiatrists today are either self-taught (Sachdev P. S., 2005) or trained via research, with few structured clinical programs available worldwide (Bolton, 2013). Although core curricula have been proposed (Sachdev and Mohan, 2017), training is often confined to tertiary care settings, with minimal community-based integration (Agrawal et al., 2015), having repercussions in the process of construction of knowledge (Fulford et al., 2014).
Toward a new neuropsychiatry: framework for an integrative paradigm
To address the longstanding conceptual and practical limitations of neuropsychiatry, diverse approaches across disciplines have begun to converge. Advances in neuroscience have facilitated closer integration between neurology and psychiatry, while insights from the humanities have reinforced the importance of subjective experience within neuroscientific perspectives (Fuchs, 2020; Kyzar and Denfield, 2023; Northoff and Ventura, 2025). These convergences support the need for a more coherent synthesis of clinical and research practices that can foster a dialogue between objective and subjective domains. In this section, we propose an epistemological structure aligned with contemporary research frameworks to lay the groundwork for a new neuropsychiatric paradigm, grounded in a non-reductive neurophilosophy informed by cooperative naturalism (Klar, 2021).
Neuropsychiatry is a hybrid discipline situated at the intersection of the humanities and natural sciences (Berríos, 2011), requiring a delimitation of its scope (Figure 2). It aims not only to explain brain states in neurological or psychiatric disorders but also aims to understand mental phenomena as dynamic, context-specific experiences imbued with emotional, volitional, and cognitive dimensions (Berríos, 2011). Unlike impairments in memory or language, mental symptoms acquire context-dependent meaning shaped by subjectivity and intersubjectivity (Fuchs, 2010). Thus, addressing mental phenomena within neurological disorders requires an inter-field approach; one that aims to integrate biological, environmental, and developmental dimensions while enabling a dialogue subjective experience and objective data (Kyzar and Denfield, 2023). This requires a domain and methodological pluralism (Klar, 2021).
Neuropsychiatric scope. Neuropsychiatry requires epistemological boundaries to avoid being a “no man's land.” This figure contrasts WHO definitions of neurological and mental disorders with the scope proposed by Bhattacharya et al. (2015) highlighting the need for conceptual and clinical integration.
Constructing knowledge within this paradigm requires viewing mental and body–brain domains as reciprocally interactive systems. A constructivist stance operationalizes this view through concept–fact iterativity, linking logical and empirical plausibility (Northoff, 2022). Neuropsychiatric inquiry must therefore incorporate empirical data while also integrating three levels of analysis: behavior, neuropsychological functions, and subjective experience (Ramírez-Bermúdez et al., 2024), highlighting the embodied nature of the human mind (Jingzhu and Qiaohua, 2018).
This integration necessitates combining qualitative and quantitative approaches, bridging nomothetic and idiographic forms of knowledge (Slade, 2012). The tension between standardized measures and individual meaning can be productively addressed through constructionism, which acknowledges knowledge as negotiated and shaped by researchers and clinicians as active participants (Slade, 2012). This highlights the need for reflexive scientific practice within neuropsychiatry (Kamenova, 2010). Consequently, a non-reductive methodology is essential for developing ecological models integrating cognitive, affective, and social neuroscience with descriptive psychopathology (Stanghellini and Broome, 2014), neuropsychology, and phenomenology (Van Oudenhove and Cuypers, 2014). We put forward a proposal described in Figure 3.
Framework for integrating subjective and objective perspectives. Neuropsychiatry requires regarding the person simultaneously as a subject and an object. Clinical and research assessments must therefore rely on frameworks that bridge subjective and objective perspectives, conceiving neurological and mental phenomena as components of an integrated body–brain system. Within this view, allostatic interoception offers a fundamental mechanism for understanding how the brain predicts and regulates bodily physiology while also giving rise to subjective experience, as proposed in constructed emotion theory (Barrett, 2017; Katsumi et al., 2022). Through this integrative process, allostasis shapes neurocognitive, affective, and social functioning (Santamaría-García et al., 2024). Allostatic interoception can be productively combined with research methodologies grounded in predictive coding and Bayesian brain models, with computational approaches (Castro Martínez and Santamaría-García, 2023; Santamaría-García et al., 2024). These frameworks enable the characterization of low-dimensional body states that typically lie outside awareness and that, upon becoming conscious, manifest as subjective experience (Aragona and Marková, 2015; Katsumi et al., 2022; Berrios and Marková, 2024). Accordingly, subjective accounts are indispensable for capturing the full complexity of neuropsychiatric phenomena. Neurophenomenology complements these models by characterizing the generic structures of experiences accessible to conscious awareness (Varela, 1996; Berkovich-Ohana et al., 2020), thus enabling mutual enrichment through the joint analysis of first-person and third-person data (Daly et al., 2024). To establish a clear dialogue between these levels: embodiment, as a way of subjective experience modulating biological variables, and enactivism, as a framework for conceptualizing person-environment interactions, provide crucial integrative bridges or points of convergence. Achieving this integration requires a systematic matching process between empirical and philosophical domains. Mental symptoms should be understood as empirical–ontological relations among brain, body, and world. In this context, philosophical concepts function as inputs that must be translated and operationalized for empirical investigation, thereby granting empirical plausibility to the conceptual framework and allowing for reciprocal refinement of its ontological claims. This bidirectional dialogue is essential for advancing a coherent, scientifically grounded neuropsychiatric paradigm.
Contemporary research frameworks exemplify this shift toward more integrative perspectives, due to the limitations of descriptive diagnostic categories that do not align with neuroscientific data, thus not capturing underlying mechanisms of dysfunction (Insel et al., 2010; Insel, 2014). This has produced a validity problem (Kendell and Jablensky, 2003). RDoC reconceptualizes mental disorders as brain disorders, promoting dimensional, translational models to identify dysfunctions in different units of analysis (Morris and Cuthbert, 2012). From an epistemological standpoint RDoC opens place to various research paradigms, enhancing a constructionist perspective (Fulford et al., 2014). Although promising, RDoC remains limited in its integration of social determinants and its applicability to neurological disorders.
HiTOP offers a dimensional approach to psychopathology that models symptom co-occurrence and provides a more precise phenotypic basis for neuroscientific research (Latzman et al., 2020). Nonetheless, HiTOP focuses on the content of subjective experience rather than its form, thus underrepresenting subjectivity (Stanghellini and Broome, 2014). Nonetheless, gaps remain in representing spectral conditions and sensorimotor domains fundamental to neuropsychiatry (Michelini et al., 2021). Together, RDoC and HiTOP offer promising, though incomplete, attempts to align biological and experiential perspectives.
Integrating dimensional frameworks can pave the way for neuropsychiatric phenotypes that capture multiple causal layers. These phenotypes may enhance neurobiological research and support individualized clinical decisions. Nonetheless, challenges remain in developing nosographic classifications that adequately reflect mechanistic diversity.
Early efforts have incorporated subjective measures (Kyzar and Denfield, 2023), aligning with the field's goal of reaching individualized, ecologically valid explanations. As research increasingly incorporates multilayered analyses, neuropsychiatrists are called to account for the multifactorial and developmental nature of brain–mind disorders (Bolton, 2013).
To get closer to this vision, neuropsychiatry could adopt deep phenotyping strategies both at neurobiological and subjective levels. This involves the fine-grained characterization of individuals through multi-level integration of biological (genomic, epigenomic, proteomic, metabolic, neurological), environmental (exposomic), and subjective dimensions (Figure 4). These complex datasets enable the identification of meaningful subtypes and promote precision medicine approaches. Additionally, deep phenotyping could facilitate iterative conceptual analysis that recognizes the historical and context-sensitive construction of meaning, as exemplified by the functional–organic distinction (Bell et al., 2020; Chesterfield et al., 2023).
Proposed neuropsychiatric assessment model. The assessment and management of neuropsychiatric disorders should begin at the epistemological level, recognizing objective and subjective domains as inherently interrelated. When approaching a patient with a neuropsychiatric condition such as epilepsy, clinicians and researchers should adopt a constructivist stance, drawing on multiple theories to construct knowledge that is contextually meaningful and aligned with specific clinical or research aims. In doing so, neuropsychiatrists may employ theoretical models and clinical proposals that account for the heterogeneity of mental symptoms in neurological conditions, such as neurobehavioral profiles (Hermann et al., 2021). These profiles must be characterized through comprehensive clinical examinations, including both neurological and mental status assessments. Data acquisition emerges through the interaction between the clinician's or researcher's epistemological position, and the patient's lived experience (extended, enactive, embodied and embedded), thereby requiring ecological and context-sensitive evaluations. This approach allows distinct profiles to emerge, which can then guide efforts toward phenotypification. Deep phenotyping may be conducted across multiple levels, such as ion channel dysfunction, predictive brain processes, or subjective accounts, depending on the pragmatic needs of the assessment. The methods selected should facilitate inquiry at the relevant level of analysis, but also should have a dialogical construction to reach a conceptual ceiling. These different accounts must then be integrated, making use of their strengths while acknowledging their limitations. Each level offers distinct affordances for developing neurobiopsychosocial formulations. By adopting this approach, clinicians and researchers can select appropriate tools from their methodological repertoire and combine them with dimensional frameworks. This process of knowledge construction supports the development of individualized treatment plans and the design of research interventions, whether at the level of the individual or within the broader exposome, incorporating rehabilitative and psychosocial–community perspectives. Through this integrative framework, mental symptoms are understood as empirical–ontological relations among brain, body, and world.
Notably, multiomics and connectomic models are now able to characterize how brain connectivity and systemic physiological processes (e.g., inflammation, autonomic regulation, metabolic activity) interact with structural social risk factors, trauma, and environmental exposures (Chen et al., 2019). Yet integrating these biological insights with subjective experience remains a major challenge. Mixed methods approaches are therefore necessary to achieve translational validity (Fulford et al., 2014).
Critically, this integrative proposal incorporates the subjective dimension as the lived, affectively charged experience of symptoms. The development of subjective patterns associated with deep phenotyping, subjective phenotypes, may allow neuropsychiatry to incorporate personal narratives and first-person data into multilevel analysis. This holistic integration promotes a nuanced science of the brain–body–mind–context interface and supports ethical, individualized, and clinically actionable care (Ritunnano, 2022), but also putting forward idiographic knowledge (Slade, 2012).
In this context, predictive coding and allostasis offer conceptual tools with implications at both biological and experiential levels (Santamaría-García et al., 2024). Predictive coding emphasizes the brain's capacity to generate and update models of the body and environment, while allostatic models explain how chronic dysregulation in stress responses may underpin both psychiatric and neurological symptoms, as sensed through interoception, making itself aware as an embodied affect, requiring categorization for the construction of an emotion (Seth and Friston, 2016; Barrett, 2017). These perspectives are especially useful in conditions like functional neurological disorders, where symptoms reflect dysregulated perception, prediction, and bodily control (Jungilligens et al., 2022). They also align with the brain's cytoarchitecture, offering a bridge between physical and psychological processes (Barrett, 2017; Katsumi et al., 2022).
In sum, a new neuropsychiatric orientation must transcend dualism and embrace complexity. Neuropsychiatry can offer a structured way to interpret disorders at the intersection of brain function, mental experience, and lived context through a constructionist epistemology that employs dimensional taxonomies, computational models, embodied cognitive science, and subjective data.
Mobilizing innovation and integration through contextualized thinking
Overcoming the challenges of neuropsychiatry requires a systemic approach grounded in robust epistemology and integrative clinical-research translation (Berríos, 2007, 2011; Berrios, 2018). This effort must operate across academic, clinical, and regulatory levels and foster interdisciplinary models that combine subjective and objective perspectives (Berríos, 2007).
Academic Formation and Clinical Training: Training should be based in part to the UCNS core curriculum (Sachdev and Mohan, 2017), preparing clinicians to assess and treat neuropsychiatric symptoms, apply disease-modifying therapies, and work within multidisciplinary teams. Additionally, the syllabus components should be adapted to priorities within the region they are embedded (Kerr et al., 2025). Clinics should be collaborative, rooted in both psychiatry and neurology, and supported by biomarkers, neuroimaging, and precision medicine frameworks (Bateman et al., 2024). Tertiary care centers must align with primary and secondary levels and integrate with community mental health systems, as previous studies have highlighted as priority areas (Mary et al., 2017). Training should include applied neuroscience, computational methods (Castro Martínez and Santamaría-García, 2023), and bedside assessments, linking psychopathology with neurodiagnostics (Peña-Casanova et al., 2024), as a tool that enables a way to connect first-person subjective experience with brain functioning (Stanghellini and Broome, 2014). Thus, collaborative enterprises with other mental health professionals is a necessity.
This integrative education should also emphasize dynamic-functional anatomy (Northoff, 2008), neuromodulation (Siddiqi et al., 2021), and interdisciplinary rehabilitation, including leadership and task-sharing strategies (Le et al., 2022). Core questions remain on balancing neurology, psychiatry, and neuropsychiatric training in systems with limited resources.
Clinical Practice: Clinical expertise must integrate subjective experience with objective data, combining clinical skill with qualitative and quantitative research knowledge, grounded in an epistemically oriented mindset. Neuropsychiatrists should assess motor-cognitive-behavioral profiles of neuropsychiatric disorders and integrate neuroimaging and physiological data via translational models (Tozzi et al., 2024). This includes conditions such as gambling disorder (Szerman et al., 2020), functional neurological disorder (Jungilligens et al., 2022), and others with social and neurobiological risk factors (Koob and Volkow, 2016). A neurodevelopmental lens can aid in early detection and effective, low-cost interventions (Uhlhaas et al., 2023), supported by genetic, epigenetic, and developmental neuroscience (Nees et al., 2021).
Neuropsychology offers cognitive assessments aligned with functional neuroanatomy (Peña-Casanova et al., 2024) aligning with the needs of other clinical disciplines like neurosurgery, neurology and psychiatry, which are central to clinical evaluation through the use of theoretical models from normal cognitive psychology in a principled and testable manner (Halligan and David, 2001). In parallel, greater convergence across disciplines is needed around known gaps; specifically, specialized training and evidence-based assessment practices embedded within advocacy, to enhance integration into the broader medical landscape (Sweet et al., 2021). Neurosurgical collaboration, especially in refractory or surgically treated cases like epilepsy, is vital for identifying relevant neurocircuitry and managing postsurgical sequelae (Bauerle et al., 2023). Interdisciplinary practices can innovate therapeutic models (Pedrotty et al., 2021; Özge et al., 2023).
Psychotherapy Enriched by Neuroscience: Psychotherapy in neuropsychiatry must integrate subjective and neurobiological insights. The therapeutic alliance can be explored through affective, cognitive, and social neuroscience (Cammisuli and Castelnuovo, 2023), especially from an intersubjective perspective (Schilbach, 2016). Neuropsychoanalysis exemplifies how psychodynamic constructs can modulate and be modulated by brain function (Solms, 2013; Flores Mosri, 2021). The therapeutic potential of psychedelics further demands neurobiological frameworks to guide their integration (Reiff et al., 2020). However, despite these conceptual advances, clear and operational models specifying how such neuroscientific insights can be systematically translated into everyday psychotherapeutic practice remain largely underdeveloped.
Neuromodulation: Neuromodulation (rTMS, tDCS, DBS, VNS) is safe, and circuit-based (Hyde et al., 2022), integrating connectomic perspectives and advancing from circuit identification to system-level modeling (Tu et al., 2021). Understanding neuroanatomical mechanisms (Leaver et al., 2022) aids in localizing stimulation (Cocchi and Zalesky, 2018) and predicting outcomes (Pinna et al., 2018). Combining neuromodulation with psychotherapy and pharmacology represents a frontier in individualized treatment (Pedrotty et al., 2021).
Research: Neuropsychiatric research integrates first-, second-, and third-person perspectives, bridging psychiatry and neurology through computational tools (Castro Martínez and Santamaría-García, 2023), consortia (Thompson et al., 2020), and frameworks like RDoC and HiTOP (Michelini et al., 2021). Neurophenomenology (Berkovich-Ohana et al., 2020) links subjective experience with neuroscience, enabling personalized care models. These efforts can identify reversible causes or refine diagnoses. Longitudinal and idiographic methods enrich developmental trajectories (Piccirillo and Rodebaugh, 2019), while inclusion of diverse populations supports culturally grounded practices (Kleinman and Benson, 2006). Knowledge production becomes a collective, contextual process. Through this lens, social determinants gain relevance in neuroscience, prompting integration with humanities and social sciences.
Discussion
This review offers a comprehensive and integrative framework for reconceptualizing neuropsychiatry as a distinct scientific field, grounded in naturalized philosophical currents, while maintaining a strong empirical foundation. Rather than a simple synthesis of neurology and psychiatry, we argue that neuropsychiatry is defined by its hybrid epistemology, which requires a constructivist posture and a multidimensional, interdisciplinary understanding of the dynamic interface between brain function and mental phenomena (Berrios and Marková, 2002; Berríos, 2011). From this standpoint, neuropsychiatry operates as a “third space”, conceptually and methodologically, where scientific models, subjective experience and contextual determinants converge in a dialogical and iterative manner.
Historically, the field has been shaped by heterogeneous and contingent processes. Enduring effects of Cartesian substance dualism (Berrios and Marková, 2002; Berrios, 2018; Thibaut, 2018) entrenched divisions between neurology and psychiatry, between objective and subjective accounts, and between reductionist vs non reductionist models of mental symptoms. Many of these challenges stem from epistemological limitations inherited from psychiatry, yet neuropsychiatry faces additional conceptual tensions arising from the particular niche of mental symptoms in neurological diseases. Moving beyond these binary frameworks requires a shift toward a constructivist and contextualized paradigm that incorporates developmental, dimensional, and socially informed models. This repositioning allows neuropsychiatry to leverage advances in neuroscience, including predictive coding and allostatic inference (Tu et al., 2021; Santamaría-García et al., 2024), alongside philosophical contributions from non reductive neurophilosophy (Van Oudenhove and Cuypers, 2014), neurophenomenology (Berkovich-Ohana et al., 2020), and enactive and embodied approaches (Krueger, 2021).
Consistent with this view, our analysis underscores that neuropsychiatric disorders frequently occupy a conceptual “no man's land” within traditional nosology systems. Strict categorical boundaries fail to capture the complexity of syndromic presentations. Dimensional and translational models (e.g., RDoC, HiTOP) (Latzman et al., 2020) provide more productive avenues for research and clinical practice, particularly when integrated with subjective and ecological data. These frameworks facilitate the delineation of neuropsychiatric phenotypes grounded in both brain-body dysfunction and lived experience, thereby enhancing diagnosis, rehabilitation, and treatment strategies (Estingoy, 2019), and conceptual analysis.
A central contribution of this review is its emphasis on contextualization. Cultural, technological, and socioeconomic factors shape how neuropsychiatric disorders are conceptualized, assessed, and treated (Berrios and Marková, 2002; Drouin et al., 2022). Thus, reflexivity becomes fundamental for framing those concepts. This is particularly relevant in regions like Latin America, where research capacity, training opportunities, and access to specialized care remain uneven (Baez et al., 2023; Ramírez Bermúdez et al., 2026). A globally sensitive neuropsychiatry must therefore integrate clinical neuroscience with local knowledge systems, low-cost diagnostic tools, and community-based practices. Such alignment improves ecological validity and helps mitigate persistent health inequities.
Training and clinical practice must reflect this complexity. Such programs should be vertically and horizontally integrated across levels of care (Mary et al., 2017), combining clinical exposure, neuroscientific knowledge, and cultural competence (Kleinman and Benson, 2006), with clinical competency with psychiatric and neurologic assessments in multidisciplinary teams and shared research infrastructures (Chemali, 2005). These systems should facilitate precision medicine approaches that account for genetic, epigenetic, and connectomic data, as well as social determinants and environmental exposures (Castro Martínez and Santamaría-García, 2023).
Our manuscript additionally advances the need for deep phenotyping frameworks capable of integrating body–brain biology, multi-omics, developmental trajectories, and environmental exposure. Neuropsychiatry is uniquely positioned to model the complexity of mental symptoms using computational approaches grounded in predictive processing and allostatic inference, while simultaneously engaging constructivist and relational perspectives (Barrett, 2017; Jungilligens et al., 2022). This integration enables more precise prediction, individualized interventions, and the development of system-level models that reflect the multilevel nature of neuropsychiatric disorders. It also contributes to the development of a “subjective phenotype”, a layer of lived experience that complements and enriches neurobiological and behavioral dimensions (Berkovich-Ohana et al., 2020), and fosters new methods for constructing knowledge (Figure 3).
This integrative and convergent view is exemplified by emerging dialogues between psychotherapy and neuroscience. Therapeutic encounters are inherently relational fields shaped by intersubjectivity, affectivity, and second-person neuroscience (Schilbach, 2016). Consequently, psychotherapeutic models should adopt a transdisciplinary orientation that incorporates these intersubjective processes while remaining grounded in, or explicitly informed by, neurobiological mechanisms. This is evident in novel modalities such as psychedelic-assisted psychotherapy (Reiff et al., 2020), which require conceptual frameworks capable of integrating neurobiological and subjective dimensions of the individual.
Conclusions
Neuropsychiatry is poised to become a truly transdisciplinary field that unites empirical rigor with subjective insight and social relevance. Future development depends not on consolidating a single overarching theory but on adopting a constructive orientation that enables navigation through the multicausal, non-linear, and layered nature of mental disorders. This endeavor requires bridging basic and clinical science, objectivity and intersubjectivity, and global and local contexts. Such bridges define both the central challenge and the promise of contemporary neuropsychiatry. Rather than resolving longstanding ontological debates, neuropsychiatry can offer epistemic tools and methodological principles for integrating diverse explanatory levels, biological, psychological, phenomenological, and sociocultural, into clinically meaningful accounts.
By adopting pluralistic, non-reductive frameworks informed by dimensional models, deep phenotyping, embodied cognition, and subjective data, neuropsychiatry can advance toward individualized, context-sensitive, and ecologically valid approaches to understanding and treating mental symptoms.
This comprehensive, philosophically grounded, and practice-oriented vision outlines a roadmap for a neuropsychiatry that is scientifically robust, clinically innovative, and ethically attuned to diverse populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agrawal N. Bhattacharya R. Rickards H. (2015). Provision of neuropsychiatry services: variability and unmet need. BJ Psych. Bull. 39, 297–301. doi: 10.1192/pb.bp.114.04732426755990 PMC 4706222 · doi ↗ · pubmed ↗
- 2AMEDD Center of History and Heritage (n.d.). History of Neuropsychiatry in World War I. Available online at: https://achh.army.mil/history/book-wwi-neuropsychiatry-section 2chapter 1 (Accessed July 12, 2025).
- 3ANPA (1988). American Neuropsychiatric Association.
- 4Aragona M. MarkováI. S. (2015). L'herméneutique de symptômes mentaux selon l'École de cambridge. Revista Latinoamericana de Psicopatologia Fundamental 18, 599–618. doi: 10.1590/1415-4714.2015 v 18n 4p 599.2 · doi ↗
- 5Arciniegas D. B. Kaufer D. I. (2006). Core curriculum for training in behavioral neurology and neuropsychiatry the joint advisory committee on subspecialty certification of the American Neuropsychiatric Association and the society for behavioral and cognitive neurology. J. Neuropsychiatry Clin. Neurosci. 18:6. doi: 10.1176/jnp.18.1.616525065 · doi ↗ · pubmed ↗
- 6Baez S. Alladi S. Ibanez A. (2023). Global South research is critical for understanding brain health, ageing and dementia. Clin. Transl. Med. 13:e 1486. doi: 10.1002/ctm 2.148637987144 PMC 10660824 · doi ↗ · pubmed ↗
- 7Barrett L. F. (2017). The theory of constructed emotion: an active inference account of interoception and categorization. Soc. Cogn. Affect. Neurosci. 12, 1–23. doi: 10.1093/scan/nsx 06027798257 PMC 5390700 · doi ↗ · pubmed ↗
- 8Bateman J. R. Josephy-Hernandez S. Apostolova L. G. Benjamin S. Barrett A. M. Boeve B. F. . (2024). Promoting growth in behavioral neurology: a path forward. Cogn. Behav. Neurol. 37, 49–56. doi: 10.1097/WNN.000000000000036838717325 · doi ↗ · pubmed ↗