Distal triceps tendon rupture repair results in high return to sport rates for amateur and professional athletes: a systematic review
Caleb J. Vandenberg, Daniel C. Touhey, Robert H. Brophy, Matthew V. Smith, Derrick M. Knapik

TL;DR
Surgical repair of distal triceps tendon ruptures in athletes leads to high return to sport rates, with most patients resuming sports within 5 months.
Contribution
This systematic review provides the first comprehensive analysis of return to sport outcomes after DTTR repair in amateur and professional athletes.
Findings
93% of athletes successfully returned to sport at a mean of 5.2 months post-surgery.
Tendon rerupture occurred in 4.4% of cases, with 7.8% requiring reoperations.
Weightlifting and American football were the most common sports associated with DTTR.
Abstract
Distal triceps tendon ruptures (DTTRs) typically occur in active patients engaged in sports and exercises involving resisted elbow extension. Surgical repair is generally recommended to restore arm function and strength. There is currently limited evidence to guide expectations for return-to-sport (RTS) among active patients. The purpose of this investigation is to systematically review the literature to better understand outcomes after repair of DTTR, particularly in amateur and professional athletes, with a focus on RTS rate and timing, along with the incidence of post-operative complications. Studies included in PubMed, EMBASE, and Cochrane Library databases from inception to September 2025 reporting on patients identified as athletes undergoing DTTR repair were identified. Inclusion criteria included studies reporting injury mechanism, tear characteristics (extent and location),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
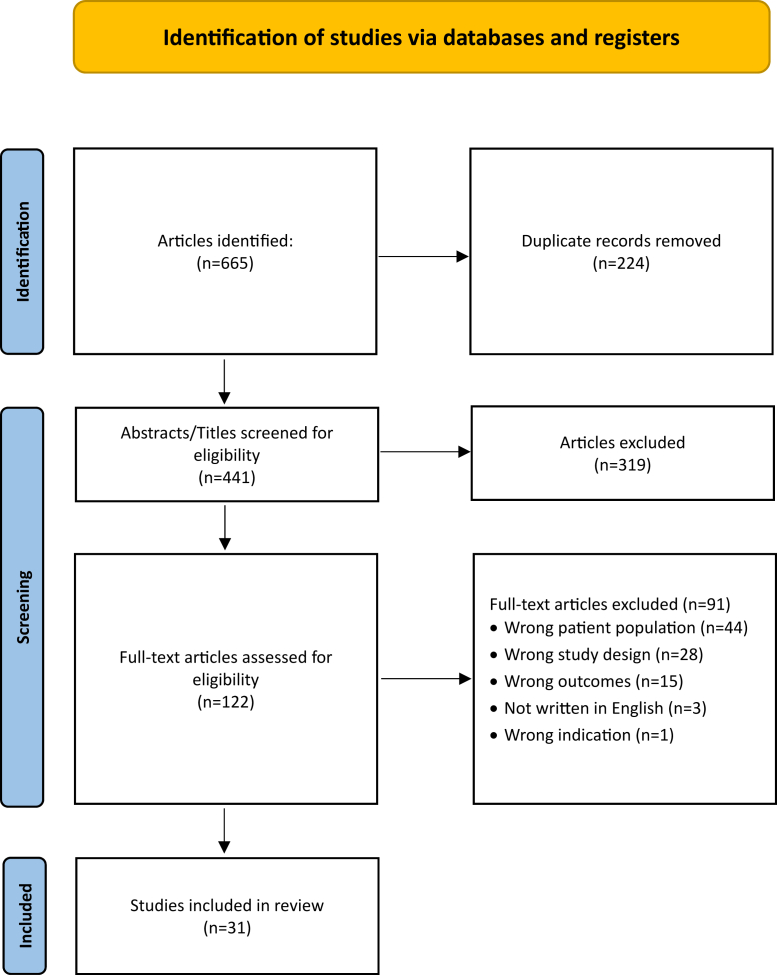 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElbow and Forearm Trauma Treatment · Tendon Structure and Treatment · Shoulder Injury and Treatment
Introduction
Distal triceps tendon ruptures (DTTRs) account for less than 1% of all tendon injuries.3^,^5^,^31^,^51 DTTRs are most commonly reported in middle-aged males and are generally associated with forceful eccentric loading across the elbow, typically during activities such as weightlifting, football, or as a result of a traumatic fall.26^,^50 In athletes and other active individuals, DTTR results in disability due to loss of elbow extension strength, limiting performance and the potential to return to preinjury activity levels. While partial DTTR may be managed conservatively, the high functional demands of athletic patients typically necessitate repair for symptomatic ruptures to restore function and strength.46^,^51
Outcomes following DTTR repair are currently limited to small case series and retrospective cohort studies, often with heterogeneous patient populations and surgical techniques. Reported return-to-sport (RTS) rates following repair are generally favorable, with studies on professional football players and military service members observing successful RTS in greater than 90% of patients.5^,^11^,^13^,^29 However, considerable variability exists in the RTS timing, criteria defining successful RTS, as well as the level of competition. In addition, complications such as rerupture, persistent pain, and/or the presence of post-operative neurologic symptoms are inconsistently reported, further confounding comparisons across studies. As such, there remains a limited understanding of RTS outcomes in athletes following DTTR repair. The purpose of this study is to systematically review the current literature to better understand RTS outcomes, timing, and the incidence of complications among athletes undergoing DTTR repair.
Methods
Search strategy and eligibility criteria
A systematic review was conducted in accordance with the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement, utilizing a Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist.37 A literature search was conducted on September 25, 2025, to identify studies reporting on patients with DTTR undergoing repair. Two authors (C.J.V., D.C.T.) independently performed a qualitative systematic review of the literature using the PubMed, Cochrane Database for Systematic Reviews, Cochrane Central Register of Controlled Trials, and Embase databases from inception to September 2025. The search was performed using various combinations of the following search terms with Boolean operators: “distal triceps tendon,” “injury,” “rupture,” “tear,” “tendon repair,” “return to sport,” return to play, “return to activity,” and “athlete.”
Inclusion criteria consisted of clinical studies written in English reporting on patients identified as athletes with DTTR with reported mechanism of injury and sporting activity, pertinent physical examination findings (eg, range of motion, palpable tendon defect), rupture characteristics (eg, defect location [eg tendon avulsion, tear at tendinous insertion, midsubstance tear]), surgical technique (eg suture repair, suture anchor, transosseous tunnel vs. tendon–tendon vs. tendon–bone repair), graft augmentation, reported post-operative complications and reoperations, as well as the rate of successful RTS, including RTS timing and level of competition (amateur, collegiate, semiprofessional, professional). Exclusion criteria consisted of non-English studies; cadaveric, biomechanical, and animal studies; previous meta-analyses and systematic reviews; review articles; editorial commentaries; as well as studies consisting of patients not identified as athletes either by means of professional sport involvement or consistent engagement in sport at the amateur level.
Title and abstract screenings were independently performed by 2 authors (C.J.V., D.C.T.), followed by a full-text screening to determine which studies met inclusion criteria. The senior author (D.M.K.) was assigned to consult if any disagreements were encountered, classified as any discrepancy raised by one of the 2 authors for article inclusion, of which none were encountered. References from the included studies were reviewed to ensure that all studies meeting the inclusion criteria were identified and included.
Data extraction
For studies meeting inclusion criteria, the following study characteristics from each article were recorded and entered into a Microsoft Excel spreadsheet (version 16.101, Redmond, WA): study title, year published, first author, level of evidence, patient demographics (mean age at time of surgery, sex), mechanism of injury, pertinent physical examination findings, mean interval time from injury to surgery, presence of concomitant injuries, tear characteristics (location, severity), surgical technique, graft type if reconstruction was performed, mean follow-up time, the incidence of post-operative complications, any patient-reported outcomes, ability to RTS, RTS time, and level of competition.
Study quality assessment
To assess bias, a methodological quality assessment was performed by 2 independent authors (C.J.V., D.C.T.) using the Joanna Briggs Institute (JBI) critical appraisal tools for case series (Appendix Table 1) and the JBI critical appraisal tool for case reports (Appendix Table 2). A third author (D.M.K.) was consulted in case of any disagreements, of which none were encountered. The JBI critical appraisal tools consist of 10 questions for case series and 8 questions for case reports, with each question scored as follows: “Y,” yes; “N,” no; “U,” unclear; and “NA,” not applicable. The total percentage of “Y” (yes) responses was recorded for each study and each question, with the highest achievable score being 100% (range, 0%-100%).4^,^32
Data analysis
Patient demographics and study characteristics were compiled and analyzed using Microsoft Excel (version 16.101, Redmond, WA). Variables such as patient age, body mass index, time from injury to surgery, and mean follow-up time were calculated and displayed as weighted means. Individual sporting activities were classified according to the relative injury risk categories defined by Rice.40 These categories ranged from greatest to least risk of injury and included contact and limited-contact sports. Contact sports included American football, basketball, jiu-jitsu, Kabbadi, snowboarding, and soccer; limited-contact sports consisted of weightlifting and bouldering.
Results
The initial literature search identified 665 articles. After removal of duplicates, 441 articles underwent title and abstract screening. A total of 122 studies were selected for full-text review. Thirty-one studies published between 1984 and 2025 were identified as meeting inclusion criteria (Fig. 1), encompassing 277 athletes with 283 elbows undergoing DTTR repair. A total of 22 studies were of Level V evidence,7^,^10^,^12^,^14^,^15^,^17^,^19^,^20^,^24^,^30^,^33, 34, 35, 36^,^38^,^39^,^41, 42, 43^,^47^,^52^,^53 while 9 were of Level IV evidence.1^,^5^,^11^,^13^,^16^,^18^,^25^,^27^,^29 The methodological quality of included studies was assessed using the JBI critical appraisal tools [Appendix Tables 1 and 2]. When assessing the mean “yes” score for case series was 87% (range, 70-100%), while the mean “yes” score for case reports was 89% (range, 63-100%).Figure 1PRISMA diagram. PRISMA, Preferred Reporting Items for Systematic Review and Meta-analyses.
Study and patient characteristics
A total of 277 athletes undergoing surgical repair for DTTR were identified from the 31 included studies (Table I). The weighted mean patient age was 36.2 years (range, 12-62 years), with 96.4% (n = 267/277) of patients being male. Body mass index was reported for 38.6% (n = 107/277) of patients, with a weighted mean of 32.7 kg/m^2^. In the subset of patients where arm dominance was reported, the dominant extremity was involved in 55.6% (n = 50/90) of cases. Bilateral DTTR repairs were performed in 2.2% (n = 6/277) of patients. Professional athletes comprised 24.8% (n = 53/214) of patients,12^,^13^,^17^,^29^,^35^,^36^,^42 while the remainder were either amateur athletes or athletes of an unspecified competitive level. The weighted mean duration of follow-up was 23.4 months (range, 12-108 months), while follow-up was not reported in 4 studies.1^,^12^,^13^,^19Table IOverview of clinical studies and patients.StudyLOENo. of patients% male patientsMean age, yrMOISporting activityRepair techniqueConcomitant Procedure(s) performedComplications/ReoperationsOutcomes (% RTS, other post-operative scores)Mean follow-up, moAgarwalla1IV689346.6Traumatic (n = 44), sports-related (n = 22)Running (n = 22), weightlifting (n = 9), swimming (n = 14), golf (n = 18), basketball (n = 14), cycling (13), baseball (n = 16), football (n = 7), and soccer (n = 3)POSR (n = 25), OSA (n = 18), OTBT (n = 25)NoneNoneRTS (89.7), VAS (2), QuickDASH (8.2), and MEPS (89.5)NRBalazs5IV5410037NRWeightlifting (n = 54)POSR (n = 54), graft augmentation (n = 1)Radial head fracture (n = 1), osteochondral injury of capitellum (n = 2), UCL injury (n = 5), anconeus tear (n = 3), flexor–pronator injury (n = 5), and biceps tendon tear (n = 1)TRF (n = 6), prolonged weakness/pain (n = 5), nerve palsy (n = 1)RTS (93.8)18Bunshah7V110040Traumatic (n = 1)Weightlifting (n = 1)POSR (n = 1)NoneNoneRTS (100), MEPS (85)12Chorba10V110035Sports-related (n = 1)Weightlifting (n = 1)NRNoneNoneRTS (100)24Dunn11IV379738.4Atraumatic (n = 3), Sports-related (n = 16), direct blow/fall (n = 8)NROTBT (n = 9), TBR (n = 3)UCL injury (n = 2), flexor–pronator mass injury (n = 2)TRF (n = 1)RTS (83.8), DASH (4.7), MEPS (85.4)49.8Figueiredo12V110042Direct blow/fall (n = 1)Jiu-jitsu (n = 1)OTBT (n = 1)NoneNoneRTS (100)NRFinstein13IV37100nrSports-related (n = 37)Football (n = 37)NRNoneNoneRTS (100)NRGoodrich14V110037Direct blow/fall (n = 1)Running (n = 1), basketball (n = 1)OTBT (n = 1)NoneNoneRTS (100)12Greer15V110043Direct blow/fall (n = 1)Weightlifting (n = 1)OTBT (n = 1)NoneNoneRTS (100)6Gruber16IV2210044.3Traumatic (n = 2), atraumatic (n = 1), sports-related (n = 18), and direct blow/fall (n = 1)NROTBT (n = 22)NoneNoneRTS (95.5), VAS (1.5)38Gupta17V110025Sports-related (n = 1)Kabaddi (n = 1)OTBT (n = 1), graft augmentation (n = 1)NoneNoneRTS (100), DASH (4.2)60Hall18IV710038Sports-related (n = 5), direct blow/fall (n = 2)Golf (n = 1), lacrosse (n = 1), cycling (n = 1), rugby (n = 1), and hockey (n = 1)OTBT (n = 7)NoneInfection-related partial rerupture (n = 1), intermittent ulnar neuropathy (n = 1)RTS (100), VAS (0), DASH (1.3), MEPS (99.3)49.2Hernandez19V1012Direct blow/fall (n = 1)Soccer (n = 1)OSA (n = 1)NoneNoneRTS (100)NRHolmes20V110050Direct blow/fall (n = 1)Weightlifting (n = 1)Graft augmentation (n = 1)NoneNoneRTS (100)18Khalil24V110013Sports-related (n = 1)Football (n = 1)OSA (n = 1)UCL rupture (n = 1)NoneRTS (100)12Kose25IV87525.1Traumatic (n = 1), sports-related (n = 3), and direct blow/fall (n = 4)Weightlifting (n = 1)OTBT (n = 8)Radial head fracture (n = 2)Ulnar nerve entrapment (n = 1), posterior interosseus nerve palsy (n = 1)RTS (100)18.8Lempainen27IV1010035Sports-related (n = 9), direct blow/fall (n = 1)Weightlifting (n = 10)POSR (n = 6), TBR (n = 4)NoneNoneRTS (90)60Mair29IV1110029Sports-related (n = 11)Football (n = 11)TBR (n = 11)NoneTRF (n = 1)RTS (90.9)36.0Mangano30V110052Sports-related (n = 1)Weightlifting (n = 1)OTBT (n = 1)NoneNoneRTS (100)24Naito33V110018Sports-related (n = 1)Football (n = 1)OTBT (n = 1)NoneNoneRTS (100)24Naula34V110052Sports-related (n = 1)Weightlifting (n = 1)TBR (n = 1), arthroscopic (n = 1)NoneNoneRTS (100), QuickDASH (18), MEPS (95)7Nikolaidou35V110028Sports-related (n = 1)Weightlifting (n = 1)TBR (n = 1), graft augmentation (n = 1)NoneNoneRTS (100)18Ntourantonis36V110032Atraumatic (n = 1)Weightlifting (n = 1)TBR (n = 1)NoneNoneRTS (100), MEPS (100), OES (48)12Pilih38V110032Direct blow/fall (n = 1)Weightlifting (n = 1)TBR (n = 1), graft augmentation (n = 1)NoneRepair failure (n = 1)RTS (100), DASH (0), OES (44)12Qin39V1027Direct blow/fall (n = 1)Climbing (n = 1)TBR (n = 1)NoneNoneRTS (100), DASH (18.3), MEPS (85), OES (42)5.5Schreiderer41V110030Direct blow/fall (n = 1)Snowboarding (n = 1)TBR (n = 1)NoneNoneRTS (100)3Sherman42V110034Direct blow/fall (n = 1)Weightlifting (n = 1)TBR (n = 1)NoneNoneRTS (100)6Shivdasani43V110053Sports-related (n = 1)Weightlifting (n = 1)TBR (n = 1)NoneNoneRTS (100), MEPS (100)12Tramer47V110038Sports-related (n = 1)Weightlifting (n = 1)TBR (n = 1)Biceps tendon repair (n = 1)NoneRTS (100)12Weistroffer52V110049Sports-related (n = 1)Weightlifting (n = 1)TBR (n = 1), graft augmentation (n = 1)NoneNoneRTS (100)24Welborn53IV210050Sports-related (n = 1), direct blow/fall (n = 1)Golf (n = 1), wrestling (n = 1)TBR (n = 2)NoneNoneRTS (100), QuickDASH (0), MEPS (100)42DASH, Disabilities of the Arm, Shoulder, and Hand; LOE, level of evidence; MEPS, Mayo Elbow Performance Score; MOI, mechanism of injury; NR, not reported; OES, Oxford Elbow Score; OSA, open suture anchor; OTBT, open transosseous bone tunnel; POSR, primary open suture repair; TBR, tendon–bone repair; TRF, traumatic repair failure; RTS, return to sport; VAS, visual analog scale; UCL, ulnar collateral ligament.
Injury characteristics, associated injuries
Rupture characteristics were reported across 59.2% (n = 164/277) of patients, with complete tears1^,^7^,^11^,^14^,^15^,^17, 18, 19, 20^,^25^,^27^,^29^,^30^,^33, 34, 35, 36^,^39^,^41, 42, 43^,^52^,^53 being most frequent (58.5%, n = 96/164), and partial tears1^,^10, 11, 12^,^18^,^24^,^27^,^38^,^47 comprising 41.5% (n = 68/164) of injuries. Location of complete rupture was reported for 27.1% (n = 26/96) of patients, including tendon avulsions from the olecranon14^,^15^,^19^,^25^,^27^,^30^,^33, 34, 35, 36^,^39^,^42^,^43^,^52^,^53 in 96.2% (n = 25/26) and tears at the musculotendinous junction17 in 3.8% (n = 1/26). The location of partial rupture was reported in 14.7% (n = 10/68) of patients, with tendon avulsions and tears at the tendinous insertion10^,^24^,^47 accounting for 30.0% (n = 3/10) and tears at the musculotendinous junction12 accounting for 70% (n = 7/10). The mechanism of injury was reported in 80.1% (n = 222/277) of patients, with sports-related injuries1^,^10^,^11^,^13^,^16, 17, 18^,^24^,^25^,^27^,^29^,^30^,^33, 34, 35^,^43^,^47^,^52^,^53 being most common (59.5%, n = 132/222), followed by unspecified traumatic injuries1^,^7^,^16^,^25^,^29 (21.6%, n = 48/222), direct blows/falls11^,^12^,^14, 15, 16^,^18, 19, 20^,^25^,^27^,^29^,^38^,^39^,^41^,^42^,^53 (11.7%, n = 26/222), and atraumatic injuries11^,^16^,^36 (2.3%, n = 5/222) (Table I).
Sport-specific activity at the time of injury was reported in 214 athletes across 29 studies. Weightlifting was the most frequent activity, reported in 40.7% (n = 87/214) of patients,1^,^5^,^7^,^10^,^15^,^20^,^25^,^27^,^30^,^34, 35, 36^,^38^,^42^,^43^,^47^,^52 followed by American football1^,^13^,^24^,^29^,^33 in 26.6% (n = 57/214). Other athletic activities included running (n = 23),1^,^14 golf (n = 20),1^,^18^,^53 and baseball (n = 16)1 (Table I). No specific sporting activity was reported in 9 patient athletes across 2 studies.18^,^25 Professional athletes comprised 24.8% (n = 53/214) of patients,12^,^13^,^17^,^29^,^35^,^36^,^42 while the remainder were either amateur athletes or athletes of an unspecified competitive level (Table I).
The use of diagnostic imaging was reported in 54.2% (n = 150/277) of patients, with magnetic resonance imaging5^,^7^,^10^,^11^,^14^,^19^,^20^,^24^,^25^,^27^,^29^,^30^,^34, 35, 36^,^38^,^41^,^43^,^47^,^52^,^53 accounting for the most common imaging modality (79.3%, n = 119/150), followed by standard radiographs5^,^7^,^12^,^14, 15, 16^,^19^,^20^,^24^,^25^,^27^,^30^,^33^,^34^,^36^,^38^,^39^,^41, 42, 43^,^47^,^52^,^53 (29.3%, n = 44/150), ultrasound (12.0%, n = 18/150),10^,^12^,^24^,^25^,^27^,^30^,^34^,^36^,^38 and computed tomography (2.7%, n = 4/150).25^,^33 Pertinent physical examination findings were reported in 54.2% (n = 150/277) of patients, consisting of pain and weakness with triceps extension7^,^10^,^12^,^14^,^17^,^19^,^20^,^24^,^27^,^29^,^30^,^33, 34, 35, 36^,^38^,^41, 42, 43^,^47^,^52^,^53 (28.7%, n = 43/150) followed by restricted elbow motion7^,^10^,^12^,^14^,^17^,^19^,^20^,^27^,^29^,^30^,^34, 35, 36^,^39^,^41^,^43^,^47^,^53 (25.3%, n = 38/150), prodromal discomfort along the posterior elbow5^,^10^,^27^,^29^,^38 (18.7%, n = 28/150), and a palpable gap along the posterior arm (16.0%, n = 24/150).14^,^15^,^17^,^20^,^24^,^29^,^30^,^34^,^35^,^39^,^42^,^47^,^52^,^53 Anabolic steroid7^,^11^,^25^,^35^,^36^,^38^,^43 use was reported in 9 patients, while 8 patients had undergone prior corticosteroid injection27^,^29^,^52 to the posterior elbow.
The presence or absence of concomitant injuries was reported in 51.6% (n = 143/277) of patients, with concomitant injuries present in 12.6% (n = 18/143) of patients across 5 studies.5^,^11^,^24^,^25^,^47 The most frequently reported concomitant injury was to the ulnar collateral ligament5^,^11^,^24 (n = 8), followed by flexor–pronator injury (n = 7)5^,^11 and radial head fracture (n = 4)5^,^25 (Table I).
Surgical characteristics and techniques
Repair for DTTR was reported at a weighted mean of 2.3 months (range, 0.1-12 months) following injury. Repair technique was reported in 77.3% (n = 214/277) of cases, most commonly involving open transosseous bone tunnel1^,^11, 12, 13, 14, 15, 16, 17, 18^,^24^,^25^,^29^,^30^,^33^,^34^,^36^,^38^,^39^,^42^,^43^,^47^,^52 (45.3%, n = 97/214), followed by primary open suture repair1^,^5^,^7^,^27 (40.2%, n = 86/214). Additional techniques included open suture anchor1^,^11^,^19^,^27^,^35^,^41^,^53 repair (14.0%, n = 30/214), DTTR reconstruction5^,^12^,^17^,^20^,^35^,^38^,^52 (3.3%, n = 7/214), and arthroscopic repair34 (0.5%, n = 1/214; Table I). Location of fixation consisted of tendon-to-bone repair,1^,^11^,^12^,^14, 15, 16, 17, 18, 19, 20^,^24^,^25^,^27^,^29^,^30^,^33, 34, 35, 36^,^38^,^39^,^41, 42, 43^,^47^,^52^,^53 reported in 80.5% (n = 128/159) of cases, and tendon-tendon repairs27 in 2.8% (n = 6/159).
Postoperative complications and reoperations
The presence or absence of post-operative complications and reoperations was reported for 74.4% (n = 206/277) of patients. A total of 10.2% (n = 21/206) of cases had a reported complication,5^,^11^,^18^,^25^,^29^,^38 most commonly involving tendon rerupture5^,^11^,^29^,^38 in 4.4% (n = 9/206) of patients, prolonged pain/weakness5^,^29^,^38 in 2.4% (n = 5/206), and nerve palsy5^,^18^,^25 (1.5%, n = 3/206) involving the ulnar nerve (n = 2) and posterior interosseous nerve (n = 1). Delayed wound healing,5 infection,18 nerve entrapment,25 and a blistering skin rash5 were each reported in a single patient. Reoperations were performed in 7.8% (n = 16/206) of patients,1^,^5^,^11^,^25^,^29^,^38 consisting of revision repair5^,^11^,^29^,^38 (n = 5), nerve decompression1^,^25 (n = 4), hardware removal1 (n = 2), and ulnar nerve repair1 (n = 2). Débridement,1 ligament repair,1 postrepair reconstruction,5 and scar tissue excision1 were each performed in a single patient (Table I).
Return to sport and functional outcomes
RTS was reported in 97.8% (n = 271/277) of patients across all 31 studies, with 93.0% (n = 252/277) successfully returning to sport at a weighted mean of 5.6 months (range, 1.6-10.6 months). A total of 63.6% (n = 42/66) of patients returned to their previous or a higher level of competition,1^,^7^,^14, 15, 16, 17^,^24^,^25^,^27^,^30^,^35^,^36^,^38^,^39^,^41^,^43^,^52^,^53 while 36% (n = 24/66) returned to sport at a lower level.1^,^16^,^27
Individual sporting activities were classified according to the relative injury risk categories defined by Rice,40 including contact and limited-contact sports. When reported, athletes participating in contact sports12, 13, 14^,^17^,^19^,^24^,^29^,^33^,^41 achieved successful RTS in 98.2% (n = 54/55) of cases at a weighted mean of 5.3 months (range, 1.6-10.6). For those participating in limited-contact sports,5^,^7^,^10^,^15^,^20^,^27^,^30^,^34, 35, 36^,^38^,^39^,^42^,^43^,^47^,^52 successful RTS was reported for 94.4% (n = 68/72) of athletes at a weighted mean of 4.4 months.
Post-operative patient-reported outcome measures were reported at final follow-up (weighted mean 23.4 months; range, 12-108 months). The weighted mean post-operative visual analog s-cale pain score1^,^16^,^18 of 1.7 (n = 97), while the weighted mean Disabilities of the Arm, Shoulder, and Hand (DASH)11^,^17^,^18^,^38^,^39 score was 4.1 (n = 24). The weighted mean QuickDASH1^,^34^,^53 score was 8.1 (n = 71), and the weighted mean Mayo Elbow Performance Score1^,^11^,^18^,^34^,^36^,^39^,^43^,^53 was 89.1 (n = 119) (Table I).
Discussion
Of the 31 identified studies comprising 277 athletes undergoing DTTR repair, males represented 96.4% of patients, with injuries most commonly reported during weightlifting and American football. DTTR repair was frequently performed using a transosseous technique at a weighted mean of 2.3 months following injury. Complications were reported in 10.2% of cases, with tendon rerupture occurring in 4.4%. Successful RTS was reported in 93% of athletes at a mean of 5.2 months following repair, with 63.6% returning to their prior or a higher level of competition.
Weightlifting and American football represented the most common athletic activities resulting in DTTR, accounting for 67.3% of reported cases when athletic activity was reported. Injury typically occurs secondary to eccentric forces applied across the elbow as a result of triceps muscle lengthening during elbow extension,11^,^23^,^55 accompanied by associated muscle contraction during resistance training, primarily occurring during the lowering phase of bench press or overhead pressing movements.10^,^11^,^30^,^35^,^43^,^47 When combined with high training volume, muscle fatigue, or pre-existing tendon degeneration secondary to tendinopathy, the risk of injury to the distal triceps tendon increases during resistance training.2^,^49 Moreover, prior corticosteroid injection and the use of anabolic steroids have also been implicated in contributing to triceps injury in weightlifting athletes.23^,^28^,^44^,^45 Meanwhile, triceps injuries in American football players are frequently associated with axial loading onto an extended upper extremity, commonly associated with blocking and tackling maneuvers. These mechanisms subject the distal triceps to eccentric overload, compounded by repetitive direct contact forces. As such, athletes participating in frequent resistance training, as well as football athletes engaged in repeated blocking, should be advised regarding the risk of DTTR, particularly athletes with a prior diagnosis of triceps tendinitis, and especially athletes utilizing anabolic steroids.
Fixation of distal triceps tears most commonly involved the use of transosseous bone tunnels. In a cadaveric study comparing 10 matched elbows undergoing either transosseous bone tunnel repair or knotless, double-row, anatomic footprint, suture anchor repair, Carpenter et al8 reported no significant difference in tendon displacement during cyclic loading or load-to-failure testing. In a multicenter retrospective cohort of 56 cases, Horneff et al22 reported excellent post-operative Mayo Elbow Performance Scores using both transosseous and suture anchor techniques (92.8 vs. 95.6; P = .25, respectively). While DASH scores following transosseous repair were 3 points lower (P = .03), this result was reported as not being clinically meaningful.22 Post-operative visual analog scale scores were equivalent between techniques (P = .6), while 2 tendon reruptures occurred in each group.21 In a systematic review comprising 16 studies (n = 591 patients), suture anchor repair was reported to yield superior results to transosseous repair based on isokinetic strength testing (95% vs. 82%), complication rates (8% vs. 18%, P = .008), and rerupture rates (2% vs. 7%, P = .03), respectively.48 Future prospective studies comparing fixation constructs with standardized RTS definitions are warranted to more accurately assess long-term outcomes in athletes returning to high-demand activities.
While overall complication rates following DTTR were relatively low, the tendon rerupture was 4.4%. Brush et al6 reported rerupture rates following transosseous tunnel repair, suture anchor repair, and combined transosseous tunnel plus suture anchor repair of 6.1%, 4.4%, and 12.5%, respectively (P = .260). Contributing factors reported to play a role in tendon rerupture include a premature RTS,5^,^16 inadequate biological healing at the tendon–bone interface,41 and overly aggressive rehabilitation.5^,^9 While anabolic and corticosteroid use are established risk factors for DTTR,28^,^45 their continued use is reported to contribute to repair failure by weakening tendon structure. Specifically, Lee et al26 reported that prior recent anabolic steroid use led to a 3.4-fold increase in the 1-year revision rate following DTTR (P < .001), with additional studies citing steroid use as a modifiable risk factor during surgical planning and post-operative management.9^,^22 While both acute and chronic DTTR undergoing primary repair generally yield satisfactory functional outcomes,21^,^31 there is no clear evidence that delayed treatment alone predicts failure.50^,^54 Further high-level evidence studies are warranted to clarify the impact of surgical timing on long-term outcomes and more accurately identify specific risk factors leading to distal tricep tendon rerupture.
A major limitation of this review was the predominance of small case series and case reports with lower levels of evidence due to selection bias, lack of control groups, and incomplete reporting of outcomes. As such, there is a need for higher-quality, prospective investigation to better guide management in athletes based on competition level, specific sport, and particularly those reporting preinjury anabolic steroid use. Moreover, the generalizability of these findings to broader athletic populations may be limited as differentiation between amateur and professional athletes was infrequent, preventing analysis evaluating differences in outcomes or RTS rate/timing based on competition level. Substantial heterogeneity was present among studies based on patient demographics, mechanisms of injury, tear characteristics, surgical techniques, rehabilitation protocols, and outcome measures. Furthermore, the heterogeneous spectrum of pathology, including both partial and full-thickness ruptures, further limited the generalizability of outcomes following surgical repair and/or reconstruction. This variability effectively prevented the performance of any meaningful statistical analysis examining these factors based on sport or level of competition. Detailed reporting of injury mechanisms, rehabilitation progression, and patient comorbidities was inconsistent, further limiting the ability to conclude specific risk factors for initial injury or rerupture. Finally, we only reported on surgical repair of these injuries, without any comparison to nonoperative management outcomes, which may be indicated in patients with partial tendon tears with preserved strength and function.
Conclusion
The vast majority of patients undergoing DTTR repair are male, most commonly engaged in weightlifting or American football. Successful RTS was reported in 93% of patients at a mean of 5.2 months following repair, while tendon rerupture was reported in 4.4% and reoperations in 7.8%.
Disclaimers:
Funding: No funding was disclosed by the authors.
Conflicts of interest: D.M.K. has received support for education from Synthes, Smith & Nephew, Elite Orthopedics, and Medwest Associates; hospitality payments from Arthrex, Elite Orthopaedics, Encore Medical, Stryker, and Smith & Nephew; honoraria from Encore Medical; and a grant from Arthrex. M.V.S. has received speaking and faculty, education, and hospitality payments from Arthrex; and education and hospitality payments from Elite Orthopaedics, and hospitality payments from Medical Device Business Services. R.H.B. has received support for education and hospitality payments from Elite Orthopaedics and hospitality payments from Zimmer Biomet. The other authors, their immediate families, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agarwalla A.Gowd A.K.Garcia G.H.Jan K.Naami E.Wysocki R.W.Return to sport following distal triceps repair J Hand Surg 482023507.e 501507.e 50810.1016/j.jhsa.2021.11.02135074247 · doi ↗ · pubmed ↗
- 2Andarawis-Puri N.Flatow E.L.Tendon fatigue in response to mechanical loading J Musculoskelet Neuronal Interact 112011106114 https://hylonome-publications.fra 1.digitaloceanspaces.com/jmni/published/44/04PURI.pdf. Accessed August 21, 202521625047 PMC 4408766 · pubmed ↗
- 3Anzel S.H.Covey K.W.Weiner A.D.Lipscomb P.R.Disruption of muscles and tendons; an analysis of 1, 014 cases Surgery 45195940641413635217 · pubmed ↗
- 4Aromataris E.Lockwood C.Porritt K.Pilla B.Jordan Z.JBI Manual for Evidence Synthesis Available at:https://jbi-global-wiki.refined.site/space/MANUAL
- 5Balazs G.C.Brelin A.M.Dworak T.C.Brooks D.I.Mauntel T.C.Tintle S.M.Outcomes and complications of triceps tendon repair following acute rupture in American military personnel Injury 4720162247225110.1016/j.injury.2016.07.06127507547 · doi ↗ · pubmed ↗
- 6Brush P.L.Trenchfield D.Pohl N.B.Swan T.L.Santana A.Jones C.M.A comparison of distal triceps tendon repair outcomes by surgical technique JSES Rev Rep Tech 4202479079610.1016/j.xrrt.2024.06.00839474181 PMC 11514082 · doi ↗ · pubmed ↗
- 7Bunshah J.J.Raghuwanshi S.Sharma D.Pandita A.Triceps tendon rupture: an uncommon orthopaedic condition Case Rep 20152015 bcr 201420644610.1136/bcr-2014-206446 PMC 436896325766435 · doi ↗ · pubmed ↗
- 8Carpenter S.R.Stroh D.A.Melvani R.Parks B.G.Camire L.M.Murthi A.M.Distal triceps transosseous cruciate versus suture anchor repair using equal constructs: a biomechanical comparison J Shoulder Elbow Surg 2720182052205610.1016/j.jse.2018.05.02530093233 · doi ↗ · pubmed ↗