Compression of the Left Brachiocephalic Vein by a Type II Right Aortic Arch: A Rare Vascular Anomaly With Unique Clinical Presentation
Ali Hamade, Mahmoud Awti, Kassem Haidar, Hasan Tarhini, Tony E Bechara

TL;DR
A rare vascular anomaly involving a right-sided aortic arch caused visible chest protrusion by compressing a major vein.
Contribution
This case report highlights a rare clinical presentation of a right aortic arch with left brachiocephalic vein compression.
Findings
A 62-year-old woman presented with a visible chest bump due to a right-sided aortic arch compressing the left brachiocephalic vein.
CT angiography confirmed the presence of an aberrant left subclavian artery and Kommerell’s diverticulum.
The anomaly led to vein dilation and protrusion, emphasizing the need for patient education and monitoring.
Abstract
Right-sided aortic arch (RAA) is an uncommon anatomical variation of the thoracic vasculature, occurring in approximately 0.1% of adults. In nearly half of these instances, the left subclavian artery follows an abnormal course. The left subclavian artery typically emerges from a tapered dilation at its origin from the aorta, referred to as Kommerell’s diverticulum (KD). Based on available literature, only a few cases have been documented. We describe a 62-year-old female patient who presented with a painless chest bump persisting for four weeks. She reported no symptoms such as cough, shortness of breath, fainting, or difficulty swallowing. Upon chest inspection, the middle of the chest exhibited a mild protrusion. Her vital signs were stable, and both pulmonary and cardiovascular examinations were normal. After an initial workup, a CT angiogram of the chest was performed and revealed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
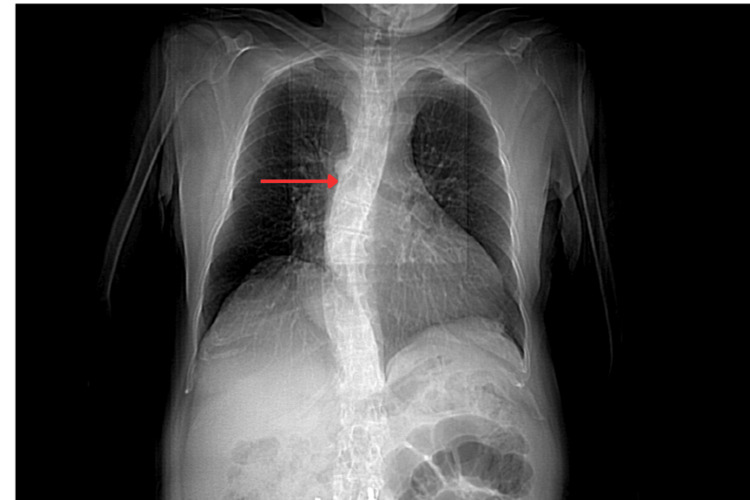 Figure 1
Figure 1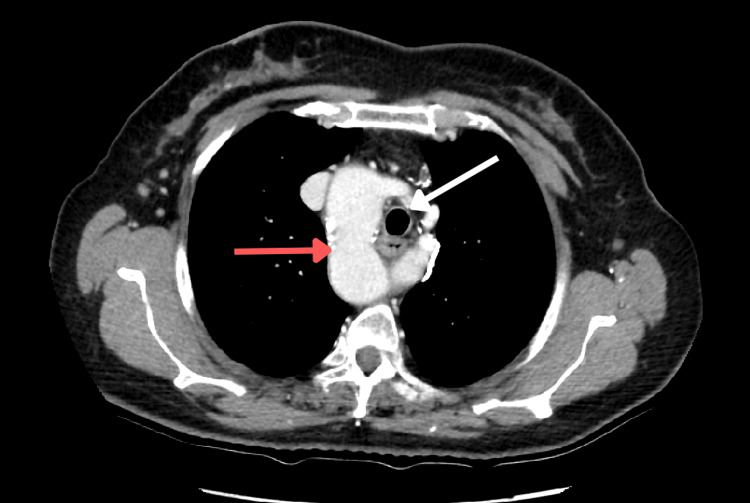 Figure 2
Figure 2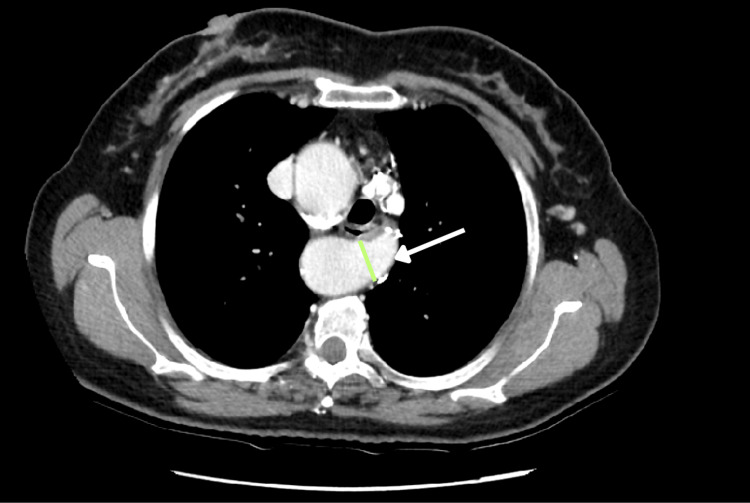 Figure 3
Figure 3 Figure 4
Figure 4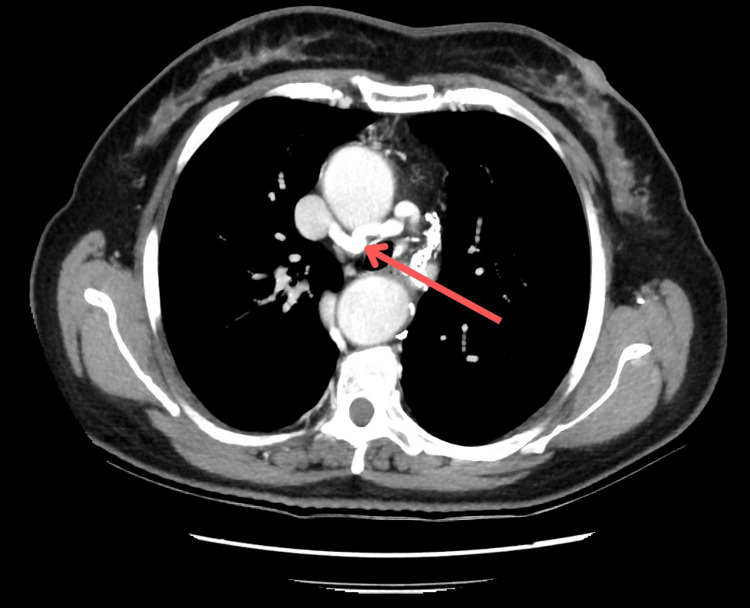 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Aortic Disease and Treatment Approaches · Congenital Heart Disease Studies
Introduction
Right-sided aortic arch (RAA) is an uncommon congenital configuration of the thoracic aorta, originally described by Fioratti and Aglietti in 1763, and identified in roughly 0.1% of adults [1]. About two out of five patients with this anomaly have an accompanying aberrant left subclavian artery (ALSA) [2]. In these instances, the altered vessel most often arises from a localized outpouching of the aortic wall, referred to as Kommerell’s diverticulum (KD) [3]. According to published reports, an estimated 50-80 cases combining RAA and ALSA originating from a KD have been documented [4].
Case presentation
A 62-year-old female patient presented with a chest protrusion at the clinic. She was a smoker and had chronic hypertension treated with valsartan/hydrochlorothiazide 160 mg/12.5 mg, amlodipine 5 mg daily, and bisoprolol 5 mg. Her past surgical history included a spinal surgery for herniated disc disease localized in her lumbar vertebrae 10 years ago. At this visit, she mentioned that the protrusion had appeared about four weeks earlier. She denied any associated pain, discomfort, or dyspnea. The protrusion was not affected by any position. The vital signs were in normal range. Thoracic examination showed a central chest hump at the level of the second and third ribs toward the right of the sternum. No thrill nor bruit was noticed. No change in skin color was noticed. Pulmonary, cardiovascular, and laryngeal examinations were unremarkable. The complete blood count (CBC), electrocardiogram (EKG), and echocardiography showed no abnormality.
A chest X-ray performed revealed a widened superior mediastinum. The trachea was shifted toward the left. Both the lung parenchyma and the pulmonary vasculature appeared unremarkable. The aortic arch and descending thoracic aorta were visualized to the right of the vertebral column.
Based on the chest X-ray findings raising suspicion for RAA, further evaluation with contrast-enhanced chest CT was done. Coronal and axial reconstructions were utilized to better delineate the mediastinal vascular anatomy. The CT scan demonstrated that the ascending aorta arched to the right of the trachea (Figures 1, 2 ) and followed a deviated course toward the left. The aortic arch gave rise to the left common carotid artery, right common carotid artery, and right subclavian artery sequentially from proximal to distal.
Coronal view of a CT chest showing the deviated descending aorta (red arrow)
Axial view of a CT scan showing the right aortic arch (red arrow) to the right of the trachea (white arrow)
The left subclavian artery was observed originating near the distal portion of the aortic arch, displaying a bulbous appearance at its origin. It coursed posterior to both the trachea and esophagus, crossing the midline toward the left and causing posterior indentation of these structures. This focal dilation at the artery’s origin (referred to as KD) measured 17 mm in its anteroposterior diameter (Figure 3).
Axial view of the CT scan showing KD (green arrow) and the left aberrant subclavian artery (white arrow)KD: Kommerell’s diverticulum
The thoracic aorta initially descended along the right side of the vertebral column before gradually shifting leftward as it approached the diaphragmatic hiatus. Adjacent to the diverticulum, the descending thoracic aorta reached a maximum diameter of 42.2 mm. Regarding the venous system, the left brachiocephalic vein (LBCV) was found to be compressed by the deviated aortic arch (Figure 4).
Axial view showing the compression of the left brachiocephalic vein (yellow arrow)
Consequently, it drained into the superior vena cava via collaterals above the azygos vein (Figure 5). At the level of the middle mediastinum, a contralateral flow joined the superior vena cava above the azygos veins (Figure 5). The esophagus was minimally compressed.
Axial view showing the collateral flow (red arrow) reaching the superior vena cava
Following a multidisciplinary team evaluation, the patient was diagnosed with a type II RAA anomaly, which was exerting compression on the LBCV. As the major mediastinal structures (including the trachea, esophagus, and pulmonary vessels) were unaffected, surgical intervention was deemed unnecessary. Further genetic testing was also considered unnecessary, as the patient’s phenotype did not suggest any chromosomal abnormalities.
Discussion
In a normal anatomy, the aortic arch curves to the left of the trachea. During the development of the embryonic arch, it can abnormally deviate from the usual pattern and course to the right, forming an RAA. Most patients with this condition have no identifiable genetic alteration; however, this variant can be associated with chromosomal abnormalities such as 22q11 deletion (DiGeorge syndrome) and with congenital cardiac malformations, including tetralogy of Fallot, truncus arteriosus, and d-transposition of the great arteries [5].
In 1948, Edwards categorized RAA into three anatomical variants (type I, II, III ) based on the branching pattern of its vessels [6-8].
The most frequent form (type II) involves an ALSA originating from KD. Less commonly, the arch may exhibit mirror-image branching of the major arteries (type I) or complete isolation of the left subclavian artery collateralization (type III), both of which are often linked to cyanotic congenital heart conditions [9].
In the type II pattern, the first vessel to arise from the aortic arch is the left common carotid artery, which is followed in order by the right common carotid, the right subclavian, and lastly the ALSA. In this subtype, the descending thoracic aorta is usually positioned on the right side of the vertebral column or close to the midline. The ALSA often stems from a remnant of the left dorsal aorta, referred to as Kommerell's diverticulum. It was named for Burckhard F. Kommerell, a German radiologist who described it in 1936 after detecting an esophageal indentation caused by a pulsating mass on a barium swallow. This vascular arrangement develops when the proximal portion of the left fourth aortic arch regresses before the origin of the left subclavian artery [10].
RAA is often asymptomatic. In pediatric cases, clinical manifestations typically stem from coexisting congenital heart defects or from esophageal or tracheal compression caused by an ALSA. Among adults with type II RAA, symptoms occur in roughly 5% of cases and are generally attributed to pressure on adjacent structures, leading to issues such as difficulty swallowing, shortness of breath, or nonspecific chest discomfort [11].
Kommerell’s diverticulum can lead to serious complications, including diverticular rupture (4%), aortic dissection (11%), rupture of an aortic aneurysm, or rupture of an aberrant subclavian artery aneurysm. As these conditions are rare, standardized management guidelines are lacking. In general consensus, surgery is recommended when the diverticulum’s orifice diameter exceeds 30 mm and/or when the adjacent descending aorta measures more than 50 mm in diameter [12,13].
Returning to our case, as the left brachiocephalic vein drained into the superior vena cava through collateral pathways (thereby restoring venous return), surgical repair was not indicated. Neither anticoagulation nor antiplatelet therapy was recommended by our medical team, as no thrombosis was observed or suspected within the venous system. The exact mechanism and timing of this presentation at such an age remain unclear; however, the most likely explanation is age-related widening and structural remodeling of the aorta, which progressively compressed the LBCV.
The patient was advised to undergo regular follow-up and to report any alarming symptoms that had been explained prior to discharge.
Conclusions
In conclusion, RAA represents a rare congenital anomaly, with an aberrant left subclavian artery being even less common. Although these vascular anomalies are uncommon, they may underlie a variety of clinical signs and symptoms. Therefore, heightened awareness of such conditions is essential for timely diagnosis and appropriate management. Notably, no documented cases of brachiocephalic vein compression secondary to RAA have been identified in the current literature. However, with the increasing accessibility and utilization of advanced imaging modalities, the incidental detection of RAA is becoming more frequent. Further research and comprehensive data are necessary to develop a standardized diagnostic and therapeutic algorithm for these anomalies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Right-sided aorta. I. Occurrence of right aortic arch in various types of congenital heart disease. II. Right aortic arch, right descending aorta, and associated anomalies Br Heart J Hastreiter AR D'Cruz IA Cantez T Namin EP Licata R 722739281966533277910.1136/hrt.28.6.722PMC 490086 · doi ↗ · pubmed ↗
- 2Right aortic arches Stat Pearls [Internet] Law MA Mohan J Treasure Island (FL)Stat Pearls Publishing 2026 http://www.ncbi.nlm.nih.gov/books/NBK 431104/28613756 · pubmed ↗
- 3Vascular rings Semin Pediatr Surg Worhunsky DJ Levy BE Stephens EH Backer CL 1511283020213493059610.1016/j.sempedsurg.2021.151128 · doi ↗ · pubmed ↗
- 4A right-sided aortic arch and aberrant left subclavian artery with proximal segment hypoplasia Interact Cardiovasc Thorac Surg Margolis J Bilfinger T Labropoulos N 3703711420122215558410.1093/icvts/ivr 032PMC 3290394 · doi ↗ · pubmed ↗
- 5Aortic arch variants and anomalies: embryology, imaging findings, and clinical considerations J Cardiovasc Imaging Bae SB Kang EJ Choo KS Lee J Kim SH Lim KJ Kwon H 2312623020223628026610.4250/jcvi.2022.0058 PMC 9592245 · doi ↗ · pubmed ↗
- 6Anomalies of the derivatives of the aortic arch system Med Clin North Am Edwards JE 9259493219481887761410.1016/s 0025-7125(16)35662-0 · doi ↗ · pubmed ↗
- 7Right aortic arch and esophageal atresia: understanding the anatomy and approach Thoracoscopic Repair of Esophageal Atresia Kanojia RP Singapore Springer 2024
- 8Interarm blood pressure difference revealing a right-sided aortic arch and occluded aberrant left subclavian artery JACC Case Rep Vanreusel I De Wolf D Van der Zijden T Van Berendoncks A 1022462920243854984910.1016/j.jaccas.2024.102246 PMC 10966364 · doi ↗ · pubmed ↗