UMG1 Defines a Targetable Subset of T‐Cell Lymphomas and Enables Precision Immunotherapy With a First‐in‐Class CD3ε Bispecific Engager
Daniele Caracciolo, Carlo Gentile, Sara Squillacioti, Stefania Signorelli, Caterina Riillo, Pinuccia Faviana, Francesco Conforti, Katia De Ieso, Elisabetta Procopio, Emanuela Altomare, Nicoletta Polerà, Maria Gaetano, Estelle Balducci, Omer Beganovic, Franca Maria Tuccillo

TL;DR
A new precision immunotherapy targeting UMG1 shows promise for treating aggressive T-cell lymphomas.
Contribution
UMG1 is identified as a targetable biomarker in T-cell lymphomas, enabling a first-in-class bispecific immunotherapy.
Findings
UMG1 is highly expressed in 62.3% of T-cell lymphoma samples, including PTCL-NOS and ALK-negative ALCL.
UMG1/CD3ε-BTCE induces strong cytotoxicity against UMG1-expressing T-cell lymphoma cells.
Combining UMG1/CD3ε-BTCE with SAHA enhances anti-tumor activity.
Abstract
T‐cell lymphomas (TCLs) account for a relatively small fraction of lymphoid malignancies and are characterized by highly aggressive course often refractory to current available therapies. We previously reported potent in vitro and in vivo antitumor activity of a Bispecific T‐Cell Engager (UMG1/CD3ε‐BTCE) directed against UMG1, a unique CD43 epitope that is abundantly expressed on T‐cell acute lymphoblastic leukemia (T‐ALL) and diffuse large B‐cell lymphoma (DLBCL) cells, while absent in most normal tissues, except thymocytes and a small fraction of peripheral blood T lymphocytes (< 5%). Here, we investigated the in vitro efficacy of UMG1/CD3ε‐BTCE against TCLs. IHC analysis of Tissue Micro Arrays (TMAs) revealed high UMG1 expression in 62.3% of TCL samples, including peripheral T‐cell lymphoma‐not otherwise specified (PTCL‐NOS) and ALK‐negative anaplastic large cell lymphoma (ALCL).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
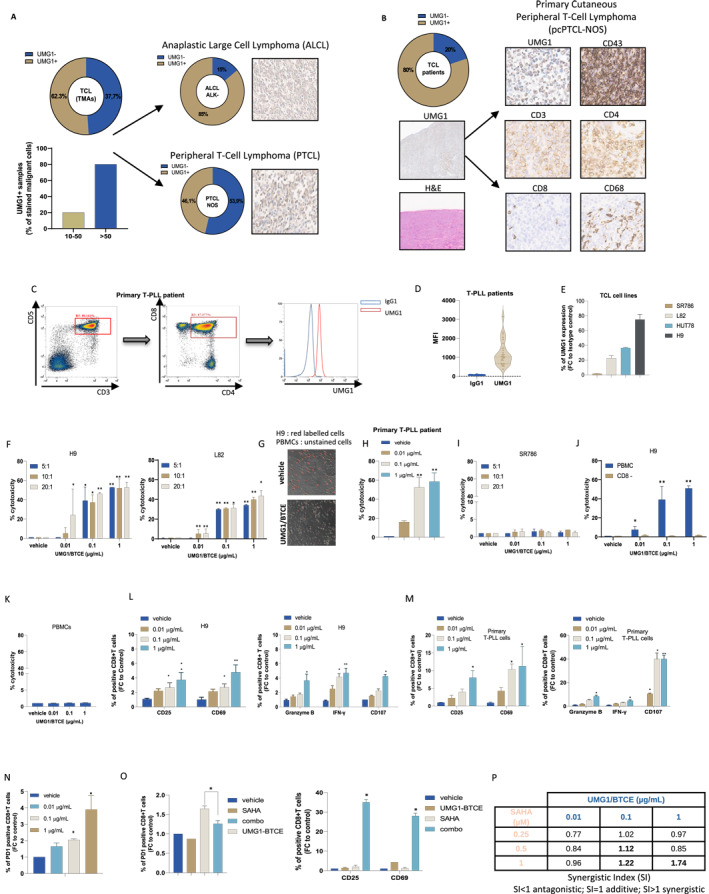 Figure 1
Figure 1- —Italian Ministry of Health PSC Salute 2014‐2020–POS4 “Cal‐Hub‐Ria”
- —BiovelocITA
- —Fondazione Roche per la Ricerca
- —Italian Ministry of Health, Ricerca Corrente 2024
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMonoclonal and Polyclonal Antibodies Research · Lymphoma Diagnosis and Treatment · CAR-T cell therapy research
T‐cell lymphomas (TCLs) are rare and aggressive hematologic malignancies that include approximately 10%–15% of non‐Hodgkin lymphomas. They include highly heterogeneous histologic entities, molecular profiles, and poor clinical outcomes, particularly in the relapsed or refractory setting [1].
In this context, UMG1, a cancer‐associated epitope of CD43, represents a high promising therapeutic target. Unlike the canonical pattern of CD43 expression, which is broadly found across a wide variety of normal hematopoietic cells, the UMG1 epitope exhibits a highly restricted distribution, limited to cortical thymocytes and a small subset of peripheral T lymphocytes (< 5%). No other normal cells/tissues express UMG1. This restricted tissue specificity opens the possibility for selective immune targeting while minimizing on‐target/off‐tumor toxicity [2, 3]. Indeed, UMG1‐directed monoclonal antibodies and bispecific T‐cell engagers (BTCEs) previously demonstrated selective cytotoxicity in T‐acute lymphoblastic leukemia (T‐ALL) [4] and diffuse large B‐cell lymphoma (DLBCL) [5], supporting UMG1 translational potential as agnostic target.
Building on this rationale, we tested the expression of UMG1 across TCLs and assessed the cytotoxic and immune‐modulatory activities of asymmetric 2 + 1 IgG‐like UMG1/CD3ε‐BTCE in both cell lines and primary patient samples.
Immunohistochemistry (IHC) on tissue microarrays (TMAs) revealed that UMG1 was expressed in 62.3% (38/61) of TCLs, with more than 50% of malignant cells showing strong membrane staining in the majority of positive cases (Figure 1A, left), including 46.1% (18/39) of peripheral T‐cell lymphoma not otherwise specified (PTCL‐NOS) and 85% (6/7) of ALK‐negative anaplastic large cell lymphomas (ALCL) (Figure 1A, right). Among primary samples, UMG1 was detected in 8 out of 10 diagnostic tissue sections, including Mycosis Fungoides and rare Primary Cutaneous Peripheral T‐cell Lymphoma (Figure 1B) (Table S1). Most notably, all tested T‐prolymphocytic leukemia (T‐PLL) samples (27/27) expressed UMG1, with a variable ratio (UMG1/IgG1 negative control) of median fluorescence intensities (MFI) (ranging from 8.5 to 3149), indicating a consistent targetability of this aggressive and rare leukemia subtype (Figure 1C–D) (Table S2).
UMG1 expression was also confirmed in 3 out of 4 TCL cell lines: H9 (high), HUT78 and L82 (low), while SR‐786 were UMG1‐negative (Figure 1E).
Importantly, UMG1/CD3ε‐BTCE treatment induced dose‐dependent cytotoxicity selectively against UMG1+ targets. H9 and L82 cell lines exhibited significant cell death, with up to 60% lysis of primary T‐PLL cells (Figure 1F–H), while no significant cytotoxicity was detected in UMG1‐ cells or in the absence of effector CD8 T cells (Figure 1I–J), confirming antigen‐specific and T cell‐dependent killing. Most importantly, our results show that UMG1/CD3ε‐BTCE did not induce significant cytotoxicity in PBMCs, indicating no fratricide effects (Figure 1K).
UMG1/CD3ε‐BTCE treatment led to robust T‐cell activation, demonstrated by CD69 and CD25 increased expression on CD8+ T lymphocytes, CD107a degranulation marker upregulation, and granzyme B and IFN‐γ secretion. These effects were observed both in cell lines and in primary patient‐derived specimens (Figure 1L–M). UMG1/CD3ε‐BTCE thus demonstrates effective immune synapse formation and cytolytic function, translating antigen engagement into effective tumor cell killing.
Of note, a subset of T cells engaged by UMG1/CD3ε‐BTCE exhibited increased expression of exhaustion markers, including PD‐1 (Figure 1N), suggesting that prolonged stimulation might induce a negative regulatory phenotype. To overcome this counteracting effect, we investigated the activity of UMG1/CD3ε‐BTCE in combination with histone deacetylase inhibitor (HDACi) SAHA (vorinostat), which has demonstrated immune‐sensitizing properties and is approved for relapsed Cutaneous and Peripheral T‐cell Lymphoma (CTCL and PTCL) [6].
Pre‐treatment of PBMCs with sub‐lethal doses of SAHA decreased UMG1/CD3ε‐BTCE‐induced exhaustion marker upregulation, enhanced activation of CD8+ T‐cell, and increased cytotoxicity against H9 cells (Figure 1O–P). Notably, since H9 cells exhibit constitutive UMG1 expression exceeding 90%, and sub‐lethal doses of SAHA were employed to avoid direct intrinsic cytotoxicity, the increased anti‐tumor activity appeared driven by enhanced T‐cell effector function, providing a rationale for combining UMG1/CD3ε‐BTCE with epigenetic modulators to overcome T‐cell exhaustion mechanisms and prolong therapeutic responses in TCLs.
The therapeutic index of bispecific antibodies targeting T‐cell malignancies remains a critical concern. Previous strategies targeting pan‐T‐cell markers, like CD4, CD5, CD7, and TCR constant regions, suffer significant challenges, including T‐cell aplasia and fratricide effects [7, 8]. In contrast, the restricted expression profile of UMG1 provides a safe therapeutic window. Additionally, the asymmetric 2 + 1 UMG1/CD3ε‐BTCE architecture ensures lower activation of circulating T cells, extending half‐life and improving tolerability.
The clinical implications of our research are substantial. T‐PLL remains one of the most difficult‐to‐treat leukemias, with a median overall survival of less than 1 year after relapse and few therapeutical options [9]. The extensive expression of UMG1 in T‐PLL strongly supports its use as a therapeutic biomarker and candidate for targeted and personalized intervention. Moreover, despite the high histologic heterogeneity of TCL, approximately 60% of tested TMAs and 80% of diagnostic tissues, including ALK negative ALCL and PTCL‐NOS, showed positive staining for UMG1. Importantly, our data indicate that UMG1 act as onco‐fetal antigen appearing during thymic ontogeny [4], being silenced in mature T‐cells, and re‐emerging upon malignant transformation, suggesting UMG1 as a stable marker linked to malignant transformation.
These results establish UMG1/CD3ε‐BTCE as a first‐in‐class candidate for immunotherapy of TCLs. Its favorable target profile, strong cytotoxic activity, and amenability to biomarker‐driven patient selection suggest potential applications in different treatment lines. Considering the challenges of CAR T‐cell manufacturing [10], especially in T‐cell neoplasms, BTCEs offer a practical and off‐the‐shelf alternative with rapid translational potential.
In summary, our study identifies UMG1 as a relevant tumor‐associated target significantly expressed in a variety of TCLs and demonstrates that UMG1/CD3ε‐BTCE can elicit a potent, antigen‐specific cytotoxicity through redirection of T‐cell effector functions. These findings support further development of UMG1‐directed immune therapeutics for precision approaches for these challenging and still lethal malignancies.
Author Contributions
D.C., C.R., S.S., S.S., M.G., N.P., and E.A. performed experiments and/or analyzed the data. C.G., F.C., L.L., E.B., and O.B. provided biological samples and analyzed the data. P.T. developed the mAb. C.G., P.F., K.D.I., E.P., and F.C. performed I.H.C. analysis. D.C., C.R., F.M.T., P.B., K.G., and L.L. provided critical evaluation of experimental data and of the manuscript. D.C. and PTagliaferri and PTassone conceived the study and wrote the manuscript. PTagliaferri and PTassone supervised the study.
Funding
This manuscript has been supported by BiovelocITA, Italy, and partially by Italian Ministry of Health PSC Salute 2014‐2020–POS4 “Cal‐Hub‐Ria” (Grant T4‐AN‐09), Fondazione Roche (Grant Fondazione Roche per la Ricerca 2024) and Italian Ministry of Health, Ricerca Corrente 2024.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Supporting Information S1
Table S1: IHC analysis of primary TCL subtypes evaluated for UMG1 expression.
Table S2: MFI of 27 T‐PLL primary samples positive to UMG1 staining. MFI of isotype control (IgG1), and the ratio between UMG1 and IgG1 MFI are also reported.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. E. Yoon and W. S. Kim , “Peripheral T‐Cell Lymphoma: What's Next?,” supplement, Hematological Oncology 43, no. S 2 (2025): e 70069, 10.1002/hon.70069.40517441 PMC 12167640 · doi ↗ · pubmed ↗
- 2F. M. Tuccillo , C. Palmieri , G. Fiume , et al., “Cancer‐Associated CD 43 Glycoforms as Target of Immunotherapy,” Molecular Cancer Therapeutics 13, no. 3 (2014): 752–762, 10.1158/1535-7163.mct-13-0651.24356816 PMC 3954431 · doi ↗ · pubmed ↗
- 3P. Tassone , H. Bond , P. Bonelli , et al., “UN 1, a Murine Monoclonal Antibody Recognizing a Novel Human Thymic Antigen,” Tissue Antigens 44, no. 2 (1994): 73–82, 10.1111/j.1399-0039.1994.tb 02362.x.7817381 · doi ↗ · pubmed ↗
- 4D. Caracciolo , C. Riillo , A. Ballerini , et al., “Therapeutic Afucosylated Monoclonal Antibody and Bispecific T‐Cell Engagers for T‐Cell Acute Lymphoblastic Leukemia,” Journal for Immunotherapy of Cancer 9, no. 2 (2021): e 002026, 10.1136/jitc-2020-002026.33597219 PMC 7893666 · doi ↗ · pubmed ↗
- 5D. Caracciolo , N. Polera , B. Belmonte , et al., “UMG 1/CD 3epsilon‐bispecific T‐cell Engager Redirects T‐Cell Cytotoxicity Against Diffuse Large B‐Cell Lymphoma,” British Journal of Haematology 204, no. 2 (2024): 555–560, 10.1111/bjh.19183.37963444 · doi ↗ · pubmed ↗
- 6A. Younes , “Beyond Chemotherapy: New Agents for Targeted Treatment of Lymphoma,” Nature Reviews Clinical Oncology 8, no. 2 (2011): 85–96, 10.1038/nrclinonc.2010.189.PMC 319243521151205 · doi ↗ · pubmed ↗
- 7N. Maciocia , B. Wade , and P. Maciocia , “CAR T‐Cell Therapies for T‐cell Malignancies: Does Cellular Immunotherapy Represent the Best Chance of Cure?,” Blood Advances 9, no. 4 (2025): 913–923, 10.1182/bloodadvances.2023012263.39715467 PMC 11876835 · doi ↗ · pubmed ↗
- 8D. Caracciolo , A. Mancuso , N. Polera , et al., “The Emerging Scenario of Immunotherapy for T‐Cell Acute Lymphoblastic Leukemia: Advances, Challenges and Future Perspectives,” Experimental Hematology & Oncology 12, no. 1 (2023): 5, 10.1186/s 40164-022-00368-w.36624522 PMC 9828428 · doi ↗ · pubmed ↗