Self-Reported Treatment for Hearing Loss in Adults Living With or Without Human Immunodeficiency Virus (HIV)
Peter Torre III, Deanna Ware, Chukwuemeka N Okafor, Gayle Springer, Howard Hoffman, Christopher Cox, Michael Plankey

TL;DR
This study examines how HIV status and hearing loss affect treatment-seeking behavior for hearing problems in adults.
Contribution
It explores the intersection of HIV-related stigma and hearing loss treatment uptake in a clinical cohort.
Findings
15.3% of participants with hearing problems reported using hearing amplification, with no difference by HIV status.
Nearly 50% of those with significant hearing trouble did not use any amplification.
The study highlights the need for increased public education on hearing loss and treatment options.
Abstract
Human immunodeficiency virus (HIV) and its treatment have been associated with hearing loss. For those who can benefit from treatment for hearing loss (i.e., hearing aids), uptake for services is low, likely due to stigma. There is also stigma for people living with HIV (PWH). As such, it is not known how both hearing loss and HIV status affect whether or not adults seek treatment for hearing loss. Therefore, the purpose of this cross-sectional (PT1) study was to evaluate self-reported hearing ability and hearing loss treatment in middle-aged and aged PWH and people without HIV (PWOH). Participants in the Multicenter AIDS Cohort Study (MACS) Women's Interagency HIV Study (WIHS) Clinical Cohort Study (MWCCS) were asked questions related to their hearing ability and whether they sought hearing services. Among the 933 participants who reported hearing problems, 143 (15.3%) reported using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
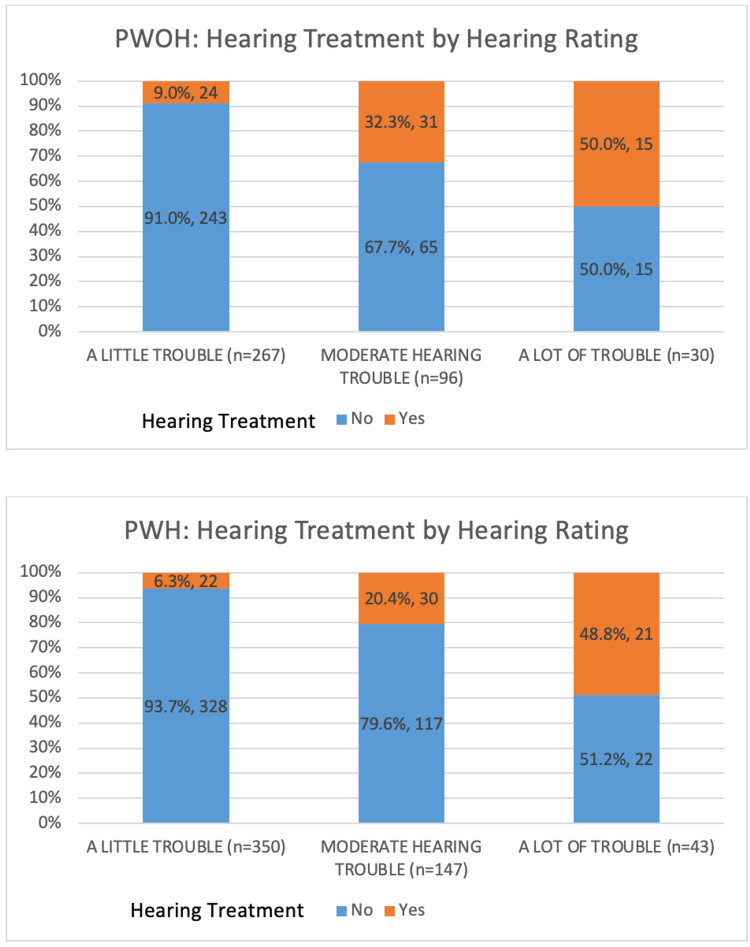 Figure 1
Figure 1| Overall (N=933) | Test statistic | ||
| No hearing amplification (N=790) | Hearing amplification (N=143) | ||
| Age in years, median (IQR)1 | 60 (52-66) | 69 (60-76) | Z=8.39; p<0.001 |
| HIV status | |||
| PWOH | 323 (40.9%) | 70 (49.0%) | χ2(1; N=933)=3.23; p=0.07; f=-0.06 |
| PWH | 467 (59.1%) | 73 (51.1%) | |
| Sex | |||
| Female | 413 (52.3%) | 42 (29.4%) | χ2(1; N=933)=25.43; p<0.01; f=0.17 |
| Male | 377 (47.7%) | 101 (70.6%) | |
| Race/ethnicity2 | |||
| White non-Hispanic | 267 (33.8%) | 92 (64.3%) | p<0.01 |
| Black non-Hispanic | 387 (49.0%) | 34 (24.8%) | |
| Hispanic | 106 (13.4%) | 15 (10.5%) | |
| Other | 30 (3.8%) | 2 (1.4%) | |
| Insurance coverage2,3 | |||
| None | 50 (6.7%) | 1 (0.8%) | p<0.01 |
| Private | 135 (18.5%) | 15 (11.5%) | |
| Medicaid | 198 (27.2%) | 15 (11.5%) | |
| Medicare | 282 (38.7%) | 83 (63.9%) | |
| Other | 15 (2.1%) | 10 (7.7%) | |
| Non-specified | 48 (6.6%) | 6 (4.6%) | |
| Doctor visit since last visit (6 months)3 | |||
| No | 74 (10.2%) | 79 (6.9%) | χ2(1; N=858)=1.33; p=0.25; f=0.04 |
| Yes | 654 (89.8%) | 121 (93.8%) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHearing Loss and Rehabilitation · Vestibular and auditory disorders · Hearing, Cochlea, Tinnitus, Genetics
Introduction
The prevalence of hearing loss in older US adults (71 years or older) is approximately 65% [1]. It is projected that the number of older US adults with hearing loss will be >73 million by 2060 [2]. Hearing loss is associated with poorer physical function [3], but also, older adults with untreated hearing loss experience greater healthcare costs and higher healthcare utilization than those with normal hearing [4]. However, between 20% [5] and 30% [1] of older adults with hearing loss report using a hearing aid. These estimates are lower in Black and Hispanic older adults and low-income individuals [1,6].
The process of acquiring hearing aids is a complex one; individuals are aware of hearing problems for approximately 10 years before acting [7]. Greater self-reported hearing problems are a significant predictor of entering a hearing aid evaluation period [8] and hearing aid adaptation [9-11]. There are non-audiological barriers to hearing aid uptake that extend beyond the cost; perceived benefit, personality traits, and locus of control (a psychological concept describing how much people believe their own actions influence the outcomes and events in their lives) are the complex factors affecting hearing aid utilization [12].
Human immunodeficiency virus (HIV) disproportionally affects those who are socially and economically marginalized, and those with the highest social vulnerability may endure barriers to HIV care services because of housing insecurity, limited access to transportation, and HIV stigma [13]. Although the gap in life expectancy between people with HIV (PWH) with access to care and people without HIV (PWOH) is down to eight years [14], access to care for PWH is improving; it remains suboptimal [15]. Maintaining access to care, for HIV or general health, is important. Unfortunately, in a longitudinal study of over 12,000 PWH, after 10 years of entry into HIV care, over 20% of PWH were lost to care [16].
Older PWH are at greater risk for hearing loss compared to older PWOH [17]. Moreover, hearing loss affects one's ability to perceive auditory events and communication with others, which can contribute to social isolation leading to a decreased quality of life [18], conditions that are also prevalent among PWH. Given the rate of PWH lost to follow-up in HIV care and the delay in acquiring hearing intervention, it is important to examine whether or not PWH seek hearing health services. As a result, the purpose of this study was to evaluate self-reported hearing ability and hearing loss treatment in PWH and PWOH.
Materials and methods
The Multicenter AIDS Cohort Study (MACS), which began in 1984, and the Women's Interagency HIV Study (WIHS), which began in 1994, were combined in 2019 to become the MACS/WIHS Combined Cohort Study (MWCCS) [19]. MWCCS participants attend annual visits for standardized clinical examinations, specimen collection, and self-reporting of sociodemographic, behavioral, and medical data. Hearing-specific data were obtained at a separate visit and included participants who responded to interviewer-administered questions related to their hearing ability between October 1, 2020, and September 30, 2022. Given that individuals who report excellent hearing are unlikely to seek hearing services, participants who reported a little trouble hearing or worse were included in this study.
Measures
Participants were asked two questions specific to their hearing from the 2019-2020 National Health and Nutrition Examination Survey (NHANES) hearing questionnaire [20]. First, they were asked: "Is your hearing 'excellent', 'good', 'a little trouble hearing', 'moderate trouble hearing', or 'a lot of trouble hearing'?" Participants with at least a little trouble hearing were then asked: "Have you used any type of device to amplify sounds (i.e., hearing aid, assistive listening device) to treat hearing impairment?" (Hearing amplification: yes, no).
Covariates
Covariates included age (years), HIV serostatus (yes, no), assigned sex at birth (female, male), race/ethnicity (White non-Hispanic, Black non-Hispanic, Hispanic, other), health insurance coverage (none, private, Medicare, Medicaid, Veterans Affairs (VA), other/unspecified), and doctor visits within six months (yes, no).
Statistical methods
Sample characteristics, by hearing amplification status, were described using median/interquartile range (IQR) and frequency/percentage, as appropriate. The differences in the distributions of sample characteristics were tested using the chi-squared, Fisher's exact (for cell sizes <10%), and Wilcoxon (for continuous variables) tests. Stacked bar charts were generated by HIV status to visualize the distributions of hearing amplification status by hearing rating. P-values less than 0.05 were considered statistically significant. All analyses were performed in SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
There were 3704 who answered the hearing-related questions, and 933 (25.2%) reported a little trouble hearing or worse. Among those 933 participants who reported hearing problems and were included in the analysis, 790 (40.9% PWOH, 59.1% PWH) of whom reported no hearing amplification (84.7%) (Table 1). Those who did not report hearing amplification were significantly younger (median age 60 years vs 69 years) than those who did report hearing amplification. A higher percentage of PWH did not report hearing amplification compared to PWOH, and the percentages were similar between PWH and PWOH who did report hearing amplification; this difference, however, was not statistically significant. Additional demographic variables (e.g., sex, race/ethnicity, insurance, and medical visits) are also shown in Table 1.
Table 1: Analytic sample characteristics stratified by hearing treatment status1Wilcoxon two-sample test. 2Fisher's exact test due to at least one cell <5. 375 participants had missing data.IQR: interquartile range; PWOH: people without human immunodeficiency virus; PWH: people with human immunodeficiency virus
For PWOH, 24 (9.0%), 31 (32.3%), and 15 (50.0%) participants who reported a little trouble, moderate trouble, and a lot of trouble hearing, respectively, used hearing amplification. Among PWH, 22 (6.3%), 30 (20.4%), and 21 (48.8%) participants who reported a little trouble, moderate trouble, and a lot of trouble hearing, respectively, reported using hearing amplification (Figure 1).
Hearing treatment status by hearing rating, stratified by HIV serostatusHIV: human immunodeficiency virus; PWOH: people without HIV; PWH: people with HIV
Discussion
Almost 85% (790 of 933) of those who reported a little trouble or worse hearing did not report using any hearing amplification. For the 15% (N=143) who did report some type of amplification, this percentage is lower than recent data for those who specifically use hearing aids [1]. Those who did report using hearing amplification were significantly older and male, yet there was no unadjusted association observed between HIV serostatus who reported using hearing amplification and those who did not. As participants reported greater difficulty hearing, there was an increase in reported use of amplification, which is consistent with previous research [9-11]. A somewhat concerning outcome of the current data, however, is that approximately 50% of participants who reported having a lot of trouble hearing still did not report using any hearing amplification.
It is not known what barriers exist within the current study for half of the participants not seeking hearing amplification even for MWCCS participants who are engaged in care. For PWH, it is possible that other comorbidities (e.g., hypertension, hyperlipidemia) [21] take priority in PWH who have hearing problems. And with the availability of over-the-counter (OTC) hearing aids, only 2% (N=25) of adults who reported hearing difficulty have purchased OTC hearing aids, and only 4% (N=48) reported that they are likely to purchase OTC hearing aids within a year [22]. It is possible, however, that hearing aid uptake rates may be different for adults enrolled in the MWCCS. Social value is the self-perceived benefit of a hearing aid combined with the benefit perceived by others. Those who report greater hearing problems likely experience more communication difficulty in social situations and, as a result, are more socially motivated to purchase hearing aids. Further, answering yes to "Do friends and relatives think you have a hearing problem?" was significantly associated with hearing aid adoption [23], which contributes to the social value of hearing aids, yet still does not account for many who do not utilize hearing aids. Further, age-related stigma associated with hearing aids which can lead to feelings of shame and embarrassment [24] along with the diversity of listening environments often requires support for those seeking hearing aids.
There are some limitations with the current research. First, no diagnostic audiometric testing was completed in order to assess hearing sensitivity; self-reported hearing ability was used. Older adults, however, are accurate when assessing their hearing ability via self-report; in fact, some overestimate hearing loss [25]. Given the number of participants in the current study, self-reported hearing was the most efficient method. Second, it is possible that for the hearing amplification question, participants may have interpreted as ever used amplification, and as a result, current hearing amplification use may not have fully been assessed.
Conclusions
There was no unadjusted difference by HIV serostatus observed in the current study, and there was low hearing amplification uptake. The reason for the lack of hearing aid utilization is likely an interaction of many factors. As mentioned previously, those who need hearing aids struggle with stigma, feelings of shame and embarrassment, and difficulty in listening environments and often require guidance on how to seek aural rehabilitation. Professional recommendations are a strong motivator where audiologists can clearly communicate the importance of professional care. Audiologists can emphasize amplification as a mechanism for empowerment, enabling improved communication in all settings, meaningful connections with family, and more active participation in social and recreational activities. Increased public education about hearing loss and amplification options will also minimize the negative opinion of hearing aids, and this can come from both audiologists and primary care physicians.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prevalence of hearing loss and hearing aid use among US Medicare beneficiaries aged 71 years and older JAMA Netw Open Reed NS Garcia-Morales EE Myers C 06202310.1001/jamanetworkopen.2023.26320 PMC 1038300237505496 · doi ↗ · pubmed ↗
- 2Addressing estimated hearing loss in adults in 2060 JAMA Otolaryngol Head Neck Surg Goman AM Reed NS Lin FR 73373414320172825338610.1001/jamaoto.2016.4642 PMC 5824202 · doi ↗ · pubmed ↗
- 3Association of age-related hearing impairment with physical functioning among community-dwelling older adults in the USJAMA Netw Open Martinez-Amezcua P Powell D Kuo PL 04202110.1001/jamanetworkopen.2021.13742 PMC 823370034170305 · doi ↗ · pubmed ↗
- 4Trends in health care costs and utilization associated with untreated hearing loss over 10 years JAMA Otolaryngol Head Neck Surg Reed NS Altan A Deal JA Yeh C Kravetz AD Wallhagen M Lin FR 273414520193041913110.1001/jamaoto.2018.2875 PMC 6439810 · doi ↗ · pubmed ↗
- 5Prevalence of hearing aid use among older adults in the United States Arch Intern Med Chien W Lin FR 29229317220122233217010.1001/archinternmed.2011.1408 PMC 3564585 · doi ↗ · pubmed ↗
- 6Hearing aid prevalence and factors related to use among older adults from the Hispanic Community Health Study/Study of Latinos JAMA Otolaryngol Head Neck Surg Arnold ML Hyer K Small BJ 50150814520193099881610.1001/jamaoto.2019.0433 PMC 6583684 · doi ↗ · pubmed ↗
- 7Hearing aid adoption in the OTC hearing aid era: market trends and consumer insights from Marke Trak 2025 Semin Hear Jilla AM Jorgensen L 1841954620254127854310.1055/s-0045-1812040 PMC 12638189 · doi ↗ · pubmed ↗
- 8Predictors of entering a hearing aid evaluation period: a prospective study in older hearing-help seekers Trends Hear Pronk M Deeg DJ Versfeld NJ Heymans MW Naylor G Kramer SE 23312165177449152120172923733310.1177/2331216517744915 PMC 5734439 · doi ↗ · pubmed ↗