Global Emergence and Spread of the XFG SARS-CoV-2 Variant and Its Clinical Profile Among XFG Patients in Maharashtra, India
Rajesh P Karyakarte, Rashmita Das, Sushma Yanamandra, Kalyani Jagarwal, Preeti Pawar, Viswanathan D V, Gilbert Chamy, Vasundhara Singh, Anna Tete, Asawari Koshti, Damini More, Poonam Madne, Vandana Patil, Suvarna Joshi, Jyoti Gurav

TL;DR
The XFG SARS-CoV-2 variant became dominant globally in late 2024-2025, spreading widely in India and showing mostly mild symptoms in infected individuals.
Contribution
This study provides insights into the global and regional spread of the XFG variant and its clinical profile in Maharashtra, India.
Findings
XFG became the predominant SARS-CoV-2 variant globally, with high prevalence in North America, Europe, and Africa.
In Maharashtra, XFG cases were mostly mild, with high recovery rates and low mortality among elderly patients with comorbidities.
XFG's rapid spread and diversification highlight the virus's adaptability and the need for enhanced surveillance.
Abstract
Background: In early 2025, changing dominance among Omicron-derived lineages culminated in the emergence of the recombinant XFG variant. XFG exhibited a significant growth advantage, rapidly emerging as the predominant SARS-CoV-2 variant in India and globally, prompting its designation as a Variant Under Monitoring by the World Health Organization in June 2025. This study examines the spread of the XFG variant and describes its clinical characteristics in Maharashtra, India. Methodology: The dataset included 204,603 SARS-CoV-2 genomes from the Global Initiative on Sharing All Influenza Data (GISAID) and 1,089 XFG sequences from India (obtained from the Indian Biological Data Centre (IBDC)), collected between November 1, 2024, and October 31, 2025, to assess the temporal and geographic distribution of XFG in the context of global SARS-CoV-2 circulation. Telephonic interviews were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
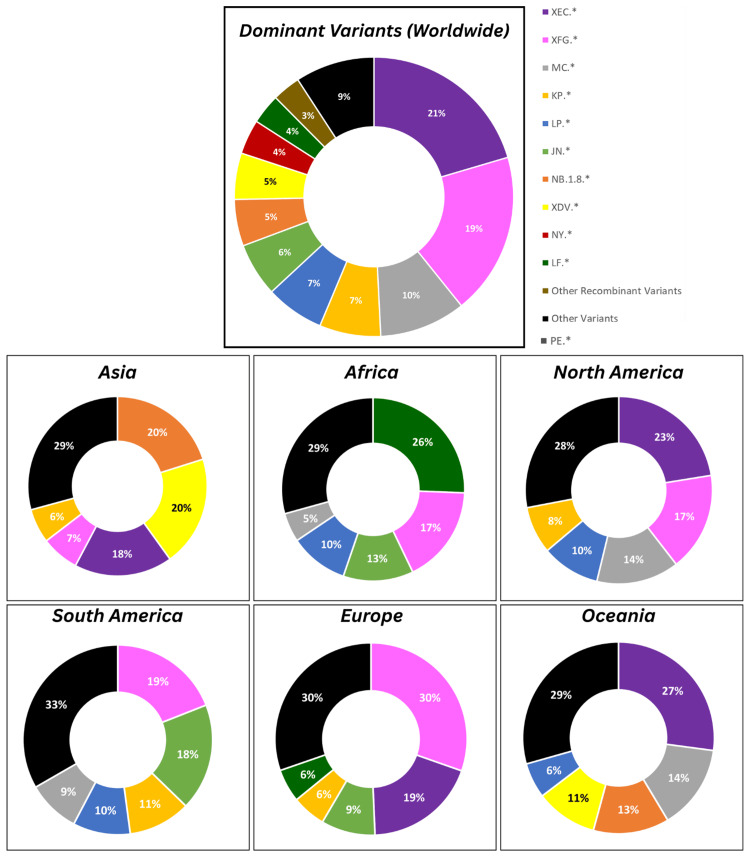 Figure 1
Figure 1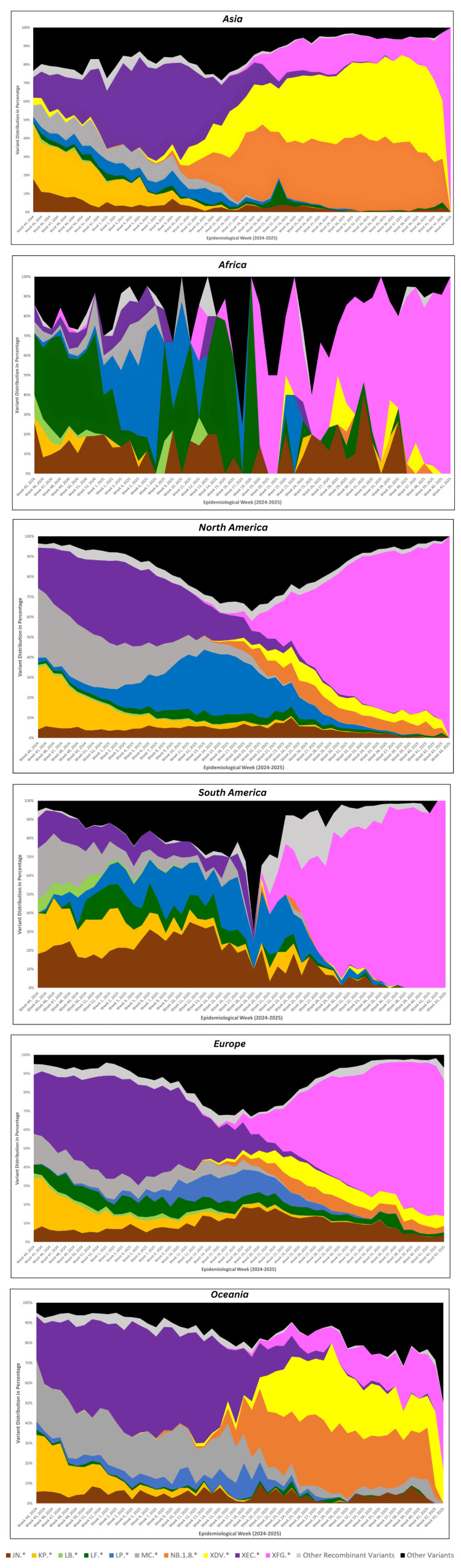 Figure 2
Figure 2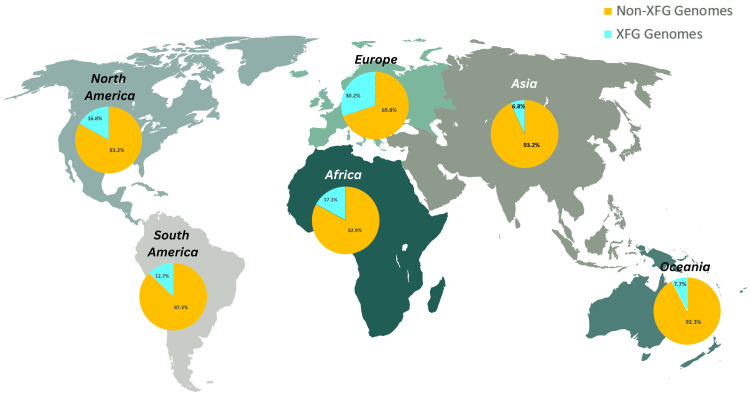 Figure 3
Figure 3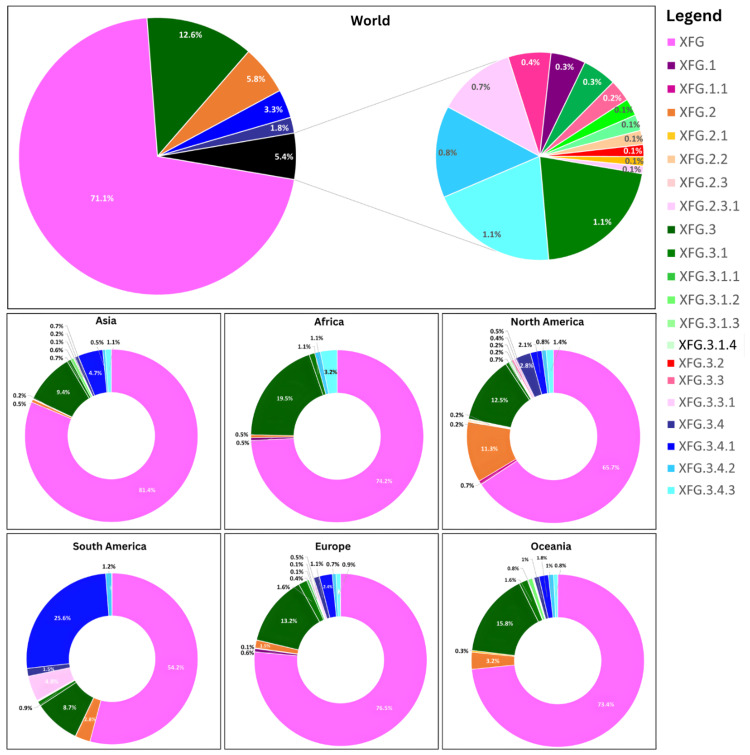 Figure 4
Figure 4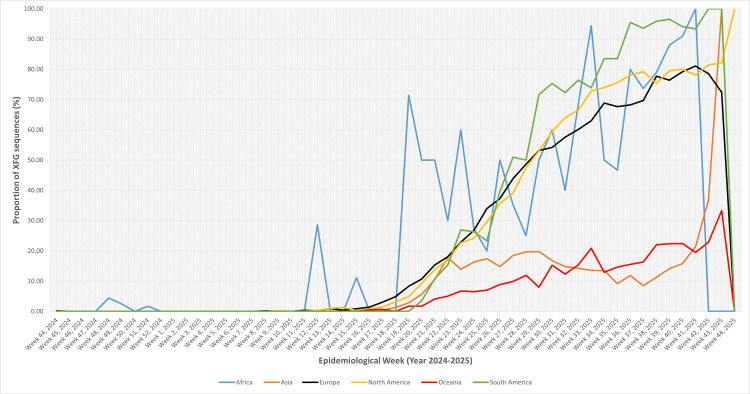 Figure 5
Figure 5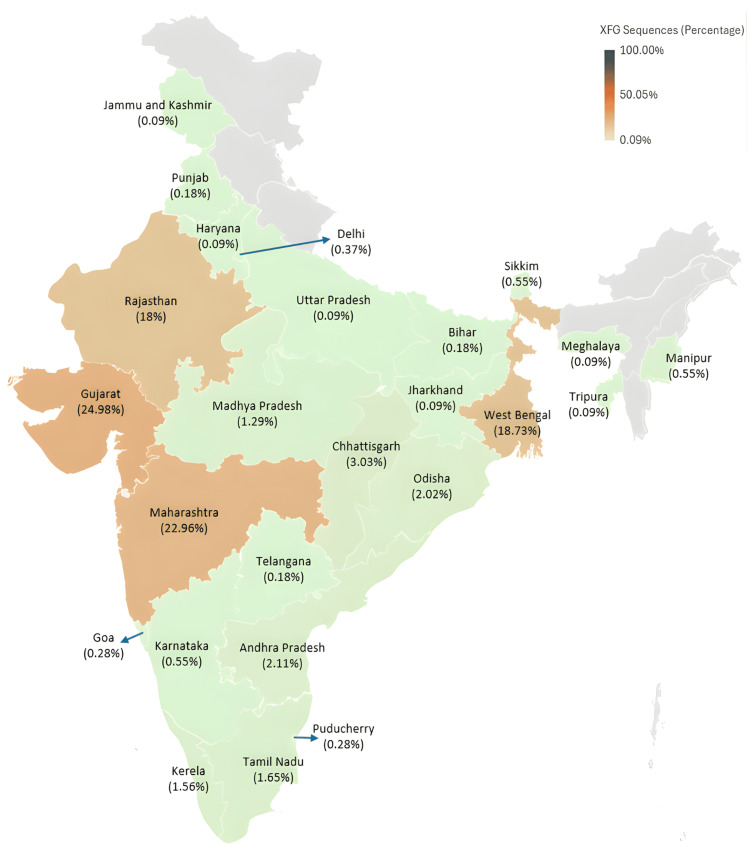 Figure 6
Figure 6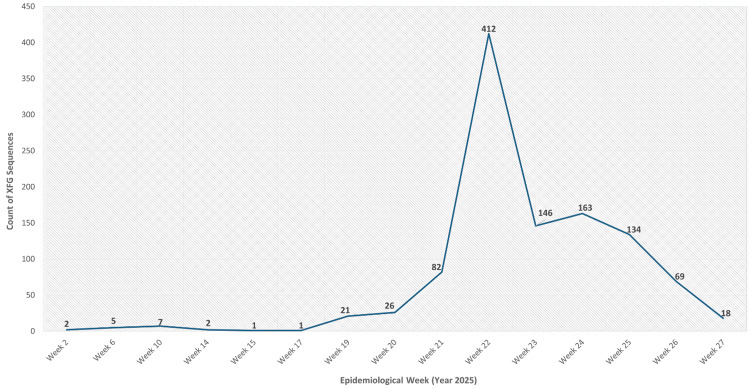 Figure 7
Figure 7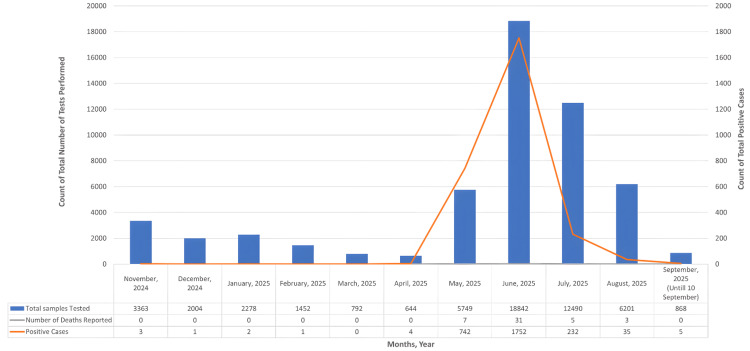 Figure 8
Figure 8| XFG sublineages | Count | Percentage (%) | ||
| XFG | 10 | 0.92 | ||
| XFG.3 | XFG.3 | 222 | 493 | 45.27 |
| XFG.3.1 | 4 | |||
| XFG.3.1.2 | 27 | |||
| XFG.3.10 | 2 | |||
| XFG.3.16 | 59 | |||
| XFG.3.18 | 1 | |||
| XFG.3.3 | 2 | |||
| XFG.3.4 | 44 | |||
| XFG.3.4.1 | 8 | |||
| XFG.3.4.2 | 12 | |||
| XFG.3.4.3 | 92 | |||
| XFG.3.5 | 3 | |||
| XFG.3.5.1 | 8 | |||
| XFG.3.7 | 9 | |||
| XFG.4 | XFG.4 | 76 | 455 | 41.78 |
| XFG.4.1 | 342 | |||
| XFG.4.2 | 37 | |||
| XFG.5 | XFG.5 | 24 | 109 | 10.01 |
| XFG.5.1 | 84 | |||
| XFG.5.2 | 1 | |||
| XFG.7 | 2 | 0.18 | ||
| XFG.11 | 4 | 0.37 | ||
| XFG.14 | 3 | 0.28 | ||
| XFG.15 | 1 | 0.09 | ||
| XFG.16 | 1 | 0.09 | ||
| XFG.21 | 11 | 1.01 | ||
| Grand total | 1089 | 100 | ||
| Demographic characteristics | Count (%) |
| Gender-wise distribution | |
| Male | 83 (46.37%) |
| Female | 96 (53.63%) |
| Age-wise distribution (years) | |
| 0-9 | 9 (5.03%) |
| 10-19 | 7 (3.91%) |
| 20-29 | 38 (21.23%) |
| 30-39 | 39 (21.79%) |
| 40-49 | 23 (12.85%) |
| 50-59 | 19 (10.61%) |
| 60 and above | 44 (24.58%) |
| Area-wise distribution in Maharashtra | |
| Pune | 168 (93.85%) |
| Ahilyanagar | 3 (1.68%) |
| Thane | 2 (1.12%) |
| Sangli | 1 (0.56%) |
| Satara | 1 (0.56%) |
| Yavatmal | 1 (0.56%) |
| Navi Mumbai | 1 (0.56%) |
| Raigarh | 1 (0.56%) |
| Latur | 1 (0.56%) |
| Clinical characteristics | Count (%) | ||
| History of previous infection | |||
| Yes | 55 (55.56%) | ||
| No | 44 (44.44%) | ||
| Presence of comorbidities | |||
| Present (the comorbidities are grouped by system, and individual patients may have multiple comorbidities.) | 31 (31.31%) | ||
| Metabolic disease | Diabetes mellitus | 18 (58.06%) | |
| Dyslipidemia | 2 (6.45%) | ||
| Cardiovascular disease | Hypertension | 17 (54.84%) | |
| Hypotension | 1 (3.23%) | ||
| Underlying heart disease | 2 (6.45%) | ||
| Endocrine disease | Hypothyroidism | 2 (6.45%) | |
| Renal disease | Renal failure | 1 (3.23%) | |
| Respiratory disease | Asthma | 1 (3.23%) | |
| Neurological disease | Parkinson's disease | 1 (3.23%) | |
| Autoimmune disease | Dermatomyositis | 1 (3.23%) | |
| Malignancy | Carcinoma | 3 (9.68%) | |
| Absent | 68 (68.69%) | ||
| Vaccination status | |||
| Vaccinated | 90 (90.91%) | ||
| One dose | 3 (3.33%) | ||
| Two doses | 39 (43.33%) | ||
| Booster dose (precautionary dose) | 48 (53.34%) | ||
| Not vaccinated | 9 (9.09%) | ||
| Symptom status | |||
| Symptomatic | 92 (92.93%) | ||
| Asymptomatic | 7 (7.07%) | ||
| Presenting symptoms (Presenting symptoms are grouped by system, and individual patients may have multiple symptoms.) | |||
| Constitutional symptoms | Fever | 75 (75.76%) | |
| Body ache | 35 (35.35%) | ||
| Fatigue | 35 (35.35%) | ||
| Respiratory symptoms | Cold | 39 (39.39%) | |
| Sore throat | 29 (29.29%) | ||
| Cough | 47 (47.47%) | ||
| Breathlessness | 18 (18.18%) | ||
| Neurological symptoms | Headache | 20 (20.20%) | |
| Loss of taste | 12 (12.12%) | ||
| Loss of smell | 10 (10.10%) | ||
| Gastrointestinal symptoms | Vomiting | 6 (6.06%) | |
| Diarrhea | 5 (5.05%) | ||
| Type of isolation | |||
| Home isolation | 68 (68.69%) | ||
| Hospital isolation/hospitalization | 31 (31.31%) | ||
| Type of treatment received | |||
| Symptomatic treatment (antipyretics, antihistaminic, multivitamins) | 82 (82.83%) | ||
| Need for oxygen therapy | 13 (13.13%) | ||
| Oxygen therapy alone | 8 (61.54%) | ||
| Invasive | 2 (25%) | ||
| Non-invasive | 6 (75%) | ||
| Oxygen therapy + steroid | 1 (7.70%) | ||
| Oxygen therapy + antiviral treatment | 2 (15.38%) | ||
| Oxygen therapy + antiviral treatment + steroid | 2 (15.38%) | ||
| Antiviral treatment alone | 2 (2.02%) | ||
| Steroids alone | 2 (2.02%) | ||
| Outcome of disease | |||
| Alive | 95 (95.96%) | ||
| Dead | 4 (4.04%) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · vaccines and immunoinformatics approaches · Respiratory viral infections research
Introduction
SARS-CoV-2, the virus responsible for COVID-19, continues to circulate globally and evolve since its first emergence in late 2019. Its remarkable adaptability is evident from the steady accumulation of a large number of mutations and emergence of multiple lineages and sublineages with varying transmission capabilities [1]. During the period from January to May 2025, the global SARS-CoV-2 variant dynamics underwent notable shifts. At the beginning of the year, XEC was the most prevalent variant globally, followed by KP.3.1.1. By February, XEC circulation began to decline, whereas LP.8.1 started to rise and became the most commonly detected variant by mid-March 2025. From mid-April, LP.8.1 started to decline with NB.1.8.1 detection increasing steadily [2].
Early 2025 saw a notable uptick in COVID-19 activity across parts of the Eastern Mediterranean, Southeast Asia, and Western Pacific regions [2]. Within Southeast Asia, a marked increase in cases was reported particularly in China, Hong Kong, Singapore, Thailand, and India [3]. This surge, beginning in late April and early May 2025, was primarily driven by the NB.1.8.1, a descendant of XDV.1.5.1, which evolved from the JN.1 variant [3,2]. As NB.1.8.1 continued to rise in global prevalence, it was designated as a Variant Under Monitoring (VUM) on May 23, 2025, by the World Health Organization (WHO), with the earliest sample collected on January 22, 2025 [4].
During this period of increasing transmission, a newly identified recombinant lineage, XFG, began to gain prominence and rapidly overtook NB.1.8.1 in circulation. This variant emerged through recombination between the Omicron sublineages LF.7 and LP.8.1.2, with the earliest sample collected on January 27, 2025. By late June 2025 (epidemiological week 22), the XFG variant had been detected in 38 countries and accounted for 22.7% of all global sequences submitted to the Global Initiative on Sharing All Influenza Data (GISAID). Its expansion was particularly striking in the Southeast Asia region, where its prevalence rose from 17.3% to 68.7%, following an earlier period of rapid dominance by NB.1.8.1 in the spring. On June 25, 2025, the WHO designated XFG as a VUM due to its apparent growth advantage over other circulating variants, including NB.1.8.1. Notably, in India, XFG had already established itself as the predominant lineage during the spring months, while NB.1.8.1 remained uncommon [5].
The present study aims to describe the temporal trends of the XFG SARS-CoV-2 variant globally and within India and to compare the trends in the context of the variant's broader emergence. In addition, it characterizes the clinical characteristics of laboratory-confirmed XFG cases in Maharashtra, India, and analyzes the associations between clinical variables and disease severity. Together, these analyses offer a comprehensive understanding of the public health relevance and clinical impact of this emerging variant.
Materials and methods
The present study forms a part of ongoing SARS-CoV-2 genomic surveillance efforts in Maharashtra, under the framework of the Indian SARS-CoV-2 Genomics Consortium (INSACOG), with the objective of monitoring genetic diversity and evolutionary trends of SARS-CoV-2.
This study was an observational, retrospective study analyzing the SARS-CoV-2 surveillance data. It comprised a descriptive analysis of publicly available SARS-CoV-2 sequences from GISAID and the Indian Biological Data Centre (IBDC) to describe temporal and geographic trends of XFG and a cross-sectional clinical characterization of laboratory-confirmed XFG cases in Maharashtra using telephonic interviews. The study was conducted at the Department of Microbiology, Byramjee Jeejeebhoy Government Medical College and Sassoon General Hospitals, Pune, India, after obtaining approval from the institute's Institutional Ethics Committee (approval number: BJGMC/IEC/Pharmac/ND-Dept0721233-233).
Lineage analysis of SARS-CoV-2 whole genome sequences from India and globally
To characterize the emergence and distribution of the XFG SARS-CoV-2 variant in Maharashtra, India, and beyond, publicly available SARS-CoV-2 genome sequences collected between November 1, 2024, and October 31, 2025, were analyzed. Genome data generated and submitted by various regional and national sequencing laboratories across India were accessed, with necessary permissions, from the Indian Biological Data Centre (IBDC). In parallel, genome sequences submitted by various international laboratories were retrieved from the GISAID repository [6]. Only complete sequences (sequences exceeding 29,000 nucleotides in length) accompanied by complete metadata, including sampling date and geographical origin, were included in the final dataset. Entries with low coverage (>5% Ns) were excluded from the dataset. The details of sequences retrieved from GISAID and IBDC are provided in Appendix A and Appendix B, respectively.
Lineage and clade annotations provided by GISAID and IBDC were utilized to describe the temporal and geographic distribution of the XFG sequences from India and of all circulating SARS-CoV-2 variants from the global dataset.
Collection of demographic and clinical data of XFG SARS-CoV-2-positive cases in Maharashtra
Demographic information, including age, sex, area of residence, contact details, and dates of sample collection, was compiled for XFG-positive cases sequenced at the Department of Microbiology, Byramjee Jeejeebhoy Government Medical College and Sassoon General Hospitals, Pune, Maharashtra, India. These details were extracted from the metadata provided by reverse transcription-polymerase chain reaction (RT-PCR) testing centers along with the specimens submitted for sequencing. To verify these records, telephonic interviews were conducted with individual patients after obtaining verbal consent. During these interviews, additional clinical information, such as presenting symptoms, type of isolation, hospitalization history, oxygen requirement, treatment received, and vaccination status, was collected. Responses were primarily self-reported; however, for children or severely ill individuals unable to respond, information provided by the primary caregiver was accepted and recorded. Cases where patients declined to share clinical details were documented and subsequently excluded from the analysis. The questionnaire template used in the study is available in Appendix C.
Daily epidemiological data, including the number of SARS-CoV-2 tests performed, test positivity rates, and counts of recoveries and deaths across Maharashtra, were obtained from the State District Health Services Department for the period between November 2024 and September 10, 2025. These data were analyzed to evaluate potential case surges temporally associated with the emergence of the XFG SARS-CoV-2 variant in the state.
Statistical analysis
Demographic and clinical datasets were recorded and analyzed using Microsoft® Excel (Microsoft Corporation, Redmond, Washington, United States). Continuous variables were presented as medians with corresponding interquartile ranges (IQRs), while categorical variables were reported as frequencies and percentages.
To assess the temporal changes in SARS-CoV-2 positivity, positivity rates were compared across aggregated epidemiological periods (pre-peak: November 2024 to April 2025; peak: May to July 2025; post-peak: August to September 2025) using the chi-squared test. Bivariate and multivariate analyses were performed to evaluate associations between clinical variables and disease severity, using hospitalization and mortality as outcomes. A p-value of ≤0.05 was considered statistically significant.
Results
Overview of global SARS-CoV-2 variant landscape
A total of 204,603 SARS-CoV-2 whole-genome sequences, submitted to GISAID during the study period, were analyzed to characterize the global distribution of major circulating lineages. The data reflects substantial lineage diversity worldwide, with over a thousand (1001) Omicron-descendant variants, including prominent variants such as XEC, XFG, MC, KP, LP, NB.1.8, XDV, JN, and LF and several other recombinant lineages.
Globally, XEC was the most dominant lineage detected (41,824 sequences; 20.4%), closely followed by XFG (38,435 sequences; 18.8%) and MC (20,450 sequences; 10%). Other notable contributors included KP (14,526 sequences; 7.1%), LP (13,863 sequences; 6.8%), JN (12,698 sequences; 6.2%), NB.1.8 (11,035 sequences; 5.4%), and XDV (10,984 sequences; 5.4%). A broad array of minor and other variants made up the remaining 46.7% (95,650 sequences), while other recombinant variants comprised 3.3% (6,674 sequences).
Regionally, variant predominance varied markedly by continent, highlighting localized circulation patterns (Figure 1). In Asia (n=27,385 sequences), NB.1.8 (20.1%) and XDV (19.9%) co-dominated with XEC (17.7%) and smaller shares from XFG (6.8%), and KP (6.2%). Africa contributed lower sequence volume (n=1,113 sequences) and greater fragmentation, led by LF (25.6%) and XFG (17.2%), followed by JN (12.4%), LP (10.3%), and other minor lineages. North America (n=98,071 sequences), the region with the highest submission rate, was driven by XEC (22.5%), XFG (17%), MC (14.3%), LP (10.1%), and smaller shares from KP.8 (8.2%), NY (5.5%), and JN (4.4%), reflecting diverse local dynamics. In South America (n=8,190 sequences), XFG (19%) prevailed, followed by JN (18.2%) and KP (10.6%). Europe (n=57,558 sequences) mirrored North American trends but with elevated XFG (30.4%) and XEC (19%), with shares from JN (9.1%), KP (5.7%), and LF (5.6%). Oceania (n=12,286 sequences) favored XEC (27.1%), MC (16.6%), NB.1.8 (12.8%), and XDV (10.4%), with XFG (5.1%) playing a smaller role.
Global and continent-wise distribution of dominant SARS-CoV-2 variants
These findings underscore the ongoing evolution and geographic heterogeneity of SARS-CoV-2, with XEC and XFG emerging as key global drivers in late 2025 globally, with continent-specific preferences, such as NB.1.8 in Asia and LF in Africa.
Temporal dynamics of SARS-CoV-2 variant circulation across continents
Figure 2 shows the spatiotemporal evolution of SARS-CoV-2 variants, weekly sequence data from 204,603 submissions (from week 44, 2024, to week 43, 2025). The data was stratified by continent and analyzed for proportional dominance across three periods: early (weeks 44-52, 2024), mid (weeks 1-26, 2025), and late (weeks 27-43, 2025). This revealed distinct regional trajectories amid global Omicron sublineage diversification, with declining submission volumes post-mid-2025 underscoring potential surveillance limitations.
Temporal trends of major SARS-CoV-2 lineages circulating across continents
Across continents, the circulating SARS-CoV-2 landscape showed substantial heterogeneity, yet several key patterns emerged. In Asia, early transmission was shaped primarily by KP and XEC, followed by a mid-phase shift towards XEC, NB.1.8, and XDV. XFG appeared later and increased steadily, reaching ~15% by the late phase, though it was not the dominant lineage in the region. In Africa, lineage patterns were more fragmented due to lower sampling. LF was the major contributor early on, transitioning to a more mixed profile during the mid-phase, with LP, LF, JN, and MC each contributing modestly. XFG remained sporadic until a late-phase spike (~69%), though this increase was driven by small sequence numbers and should be interpreted cautiously. In North America, lineage transitions were sharper. XEC and MC dominated early circulation, with LP gaining prominence mid-phase. XFG emerged slowly at first but expanded rapidly thereafter, ultimately accounting for more than 70% of late-phase genomes, representing one of the earliest and strongest regional takeovers by this lineage. South America exhibited a similar but even more pronounced pattern. Multiple variants co-circulated early (MC, JN, KP, and XEC), but XFG, initially absent, rose swiftly once introduced, becoming the overwhelmingly dominant lineage (~79%) in the late period and largely replacing other circulating variants. In Europe, early circulation was characterized by a strong presence of XEC. Although mid-phase diversity increased, XFG began to rise during this period and eventually became the predominant variant (~66%) in the late phase, marking a clear continental shift similar to that observed in the Americas. In Oceania, XEC and MC shaped early circulation, with increased lineage diversity mid-phase. XFG appeared later and expanded only modestly (~16%), never surpassing other dominant variants. This region, therefore, showed the slowest and least pronounced establishment of XFG globally.
Across regions, XFG displayed a strikingly uneven pattern of global establishment. By the late phase, it had become the dominant lineage in North America, Europe, South America, and Africa, where it accounted for approximately 66-83% of all sequences, effectively replacing earlier circulating variants. In contrast, Asia and Oceania showed only modest increases (<20%). This coordinated rise across continents highlights the strong transmissibility and competitive fitness of XFG, consistent with rapid transcontinental spread.
Geographic distribution of the XFG variant
Overall, XFG sequences constituted 18.63% of all SARS-CoV-2 genomes submitted globally to GISAID during the study period (38,114 XFG sequences out of 204,603 total genomes). The XFG variant was identified across all continents, demonstrating its broad geographical distribution.
In absolute numbers, North America contributed the largest share of XFG genomes (43.3%; 16,513 out of 38,114 sequences), followed by Asia (4.9%; 1,869 out of 38,114 sequences) and South America (4.1%; 1,556 out of 38,114 sequences).
When assessed as a proportion of each continent's total XFG genome submissions, Europe showed the highest relative representation of XFG (30.2%), followed by Africa (17.1%), North America (16.8%), South America (12.7%), and Oceania (7.7%). In contrast, Asia recorded the lowest proportion, with XFG comprising only 6.8% of its total submitted genomes (Figure 3).
Global distribution of XFG variant sequences among submitted SARS-CoV-2 genomes
Analysis of 38,114 XFG genomes submitted globally revealed substantial sublineage diversification within the XFG lineage (Figure 4). At the global level, the parent lineage XFG accounted for 71.1% of all XFG genomes, followed by XFG.3 (12.6%), XFG.1 (5.8%), XFG.3.4.3 (5.4%), XFG.3.4 (3.3%), and XFG.2 (1.8%). Several minor sublineages, including XFG.1.1, XFG.2.1, XFG.2.2, XFG.3.1, XFG.3.1.1, and others, collectively constituted the remaining proportion (5.4%), each contributing ≤1% to the global dataset.
Global and continent-wise distribution of XFG and its sublineages
Across all continents, the parent lineage XFG was the dominant sublineage, comprising more than half of all XFG genomes in every region (ranging from 54.2% in South America to 81.4% in Asia). The second most prevalent sublineage globally was XFG.3, showing notable geographic variation, with the highest proportions observed in Africa (19.5%), Oceania (15.8%), and Europe (13.2%) and comparatively lower representation in Asia (9.4%), North America (12.5%), and South America (8.7%). Some regions exhibited additional locally enriched sublineages. South America showed the greatest diversification, with a substantial proportion of XFG.3.4.1 (25.6%) and smaller contributions from XFG.3.3.1 (4.8%). North America showed a higher representation of XFG.2 (11.3%), while Africa had notable proportions of XFG.3.4.3 (3.2%). In contrast, Europe and Oceania showed relatively limited sublineage diversity, with XFG and XFG.3 accounting for the majority of sequences.
Overall, these findings highlight both the global dominance of the XFG lineage and the heterogeneous expansion of its sublineages across continents, suggesting region-specific patterns of transmission and diversification.
Temporal trends in global XFG detection
Among the analyzed datasets, the earliest detection of the XFG lineage occurred in Europe, with one genome each from Spain (epidemiological week 44, 2024) and Russia (week 45, 2024) (Figure 5). Shortly thereafter, Africa (Kenya) detected its first XFG sequences in week 48, 2024, and North America (USA) recorded isolated detections in week 50, 2024. No XFG sequences were identified in Asia, Oceania, or South America during late 2024.
Weekly proportion of XFG sequences among total SARS-CoV-2 genomes submitted from each continent (week 44, 2024, to week 44, 2025)
In early 2025, additional first detections appeared in Asia (Israel) (week 9, 2025). A consistent rise in XFG activity began around weeks 12-15, 2025, when several continents started reporting increasing numbers. This growth accelerated sharply from week 17 onward, with clear expansion across Europe, North America, and Asia and the first appearance in Oceania (a single genome from Australia in week 16, 2025). By week 20, a substantial increase was evident worldwide, particularly in Asia, Europe, North America, and Africa. South America, however, showed no activity until week 20 (a single genome from Brazil), marking a notably later emergence compared to other continents.
A period of sustained global increase extended from weeks 21 to 35, 2025, during which all continents exhibited steep increases in XFG submissions. Europe and North America experienced the most pronounced rises, peaking at week 36, 2025. In Asia, sequences peaked earlier at week 22, while Africa's activity remained lower but persistent, with weekly counts ranging from one to 22 cases. Oceania, despite its later emergence, demonstrated a steady rise from weeks 20 to 27, with peak activity in weeks 32-33, and South America, following its late introduction in week 20, showed a rapid increase with peaks between weeks 32 and 34.
Beginning week 37 onward, most continents exhibited a gradual decline, with sharp reductions observed after week 40. However, this downward trend must be interpreted cautiously, as the decrease coincides with a substantial reduction in the number of samples submitted for sequencing during this period, which may partially explain the observed fall in detected XFG sequences. By weeks 43-44, 2025, global XFG detection had markedly diminished, with only two cases reported worldwide in week 44.
In summary, XFG exhibited a globally synchronized but regionally staggered expansion, first detection in Europe and Africa in late 2024, followed by rapid amplification across all continents during mid-2025, including later-onset but substantial increases in Oceania and South America, and declining globally by late 2025.
Geographical and temporal distribution of the XFG SARS-CoV-2 variant in India
A total of 1,089 XFG sequences were retrieved from the IBDC portal and were included in the study. Following Nextclade Pangolin nomenclature, 27 different XFG sublineages were identified between week 44, 2024, and week 44, 2025. XFG.3 was the most common XFG sublineage (45.27%), followed by XFG.4 (41.78%) and XFG.5 (10.01%) (Table 1).
The XFG variant showed widespread geographic presence across India. The highest proportion of sequences was reported from Gujarat (272/1089, 24.98%), Maharashtra (250/1089, 22.96%), West Bengal (204/1089, 18.73%), and Rajasthan (196/1089, 18%), collectively accounting for over 80% of all XFG sequences detected nationwide (Figure 6).
Geographic distribution of the XFG SARS-CoV-2 variant in India based on sequences submitted to IBDCIBDC: Indian Biological Data Centre
The first XFG sequence was detected in Maharashtra on January 6, 2025 (epidemiological week 2, 2025). Sporadic detections were observed until week 17 (late April 2025), followed by a gradual increase beginning in week 19 (early May 2025) and a sharp surge peaking at week 22 (late May 2025). Thereafter, the number of XFG sequences declined progressively through weeks 23-27 (June-July 2025) (Figure 7).
Temporal distribution of XFG variant sequences across India based on sequences submitted to IBDCIBDC: Indian Biological Data Centre
Epidemiological trends during the emergence of the XFG SARS-CoV-2 variant in Maharashtra, India
Between November 2024 and April 2025, SARS-CoV-2 activity remained minimal, with a case positivity rate below 1% and no reported deaths. A sharp rise in both case numbers and positivity was observed in May 2025 (12.9%) and June 2025 (9.3%) (Figure 8), coinciding with the emergence and rapid spread of the XFG variant. By July 2025, case positivity declined to 1.9% and continued to drop in subsequent months, aligning with the genomic evidence of a reduction in XFG detections. To assess the statistical significance of these changes, positivity rates were compared across aggregated periods using a chi-squared test: pre-May (November 2024-April 2025; rate=0.10%), peak period (May-July 2025; rate=7.35%), and post-July (August-September 2025; rate=0.57%). The results indicated highly significant differences in rates (χ²=1236.66; df=2; p<0.001), confirming that the observed increase during the peak period was statistically significant and not due to chance.
Trends in SARS-CoV-2 testing, positivity, and mortality in Maharashtra (November 2024 to September 10, 2025)Note: Deaths represent monthly reported counts and are included to indicate the low fatality observed during the XFG wave.
During this period, a parallel increase in discharge rates was noted, despite increased transmission, as evident in Figure 8. Although 46 deaths were reported between May and August 2025, the numbers remained low relative to the rise in case detections, suggesting that the XFG-associated increase in transmission did not translate into increased disease severity or fatality.
Overall, the epidemiological data from Maharashtra mirrors the genomic trend, demonstrating that the XFG variant exhibited a rapid and transient rise, driving a short-lived increase in case positivity without a proportional escalation in severe outcomes.
Demographic and clinical characteristics of the XFG SARS-CoV-2 variant in Maharashtra
Complete metadata was available for 179 XFG cases included in the demographic study (Table 2). Among these 179 participants, 46.37% (83/179) were male, and 53.63% (96/179) were female. The median age of the study population was 38 (IQR: 28-60) years. The largest proportion of individuals belonged to the ≥60-year age group (24.58%). This was followed by individuals aged 30-39 years (21.79%) and 20-29 years (21.23%), together comprising over two-fifths of the study population. Most participants were from Pune (93.85%), followed by Ahilyanagar (1.68%) and Thane (1.12%).
All 179 identified cases were contacted for follow-up, of which 99 (55.31%) cases were included in the clinical study, while 80 (44.69%) cases could not be enrolled due to non-response, invalid contact details, or lack of consent. Table 3 summarizes the clinical characteristics, vaccination status, and outcome of XFG cases in Maharashtra. Most XFG cases had symptomatic disease (92 out of 99, 92.93%) with mild manifestations, such as fever, cough and cold, body ache, and fatigue. Underlying comorbid conditions, either alone or in combination, were reported in approximately one-third of cases (31 out of 99, 31.31%), with diabetes mellitus and hypertension emerging as the most prevalent, often co-occurring in affected individuals. Regarding the vaccination status, 90.91% (90 out of 99) of cases received at least one dose of the COVID-19 vaccine, while 9.09% (9 out of 99) were not vaccinated. All unvaccinated individuals were children aged 0-9 years.
Over two-thirds of patients (68 out of 99 cases, 68.69%) were managed at home with conservative symptomatic care, while the remainder (31 out of 99 cases, 31.31%) required hospitalization. Among the hospitalized cases, 61.29% (19 out of 31 cases) often received conservative treatment, with 38.71% of cases necessitating supplemental oxygen (12 out of 31 cases), often in non-invasive forms (8 out of 12 cases, 66.67%). The overall prognosis was favorable, with a near-complete recovery rate (95 out of 99 cases, 95.96%) and minimal mortality (4.04%), underscoring the generally benign course of disease in this cohort. All fatal cases occurred among elderly male patients (68-85 years) with significant underlying comorbidities. Two deaths were due to severe pneumonia and respiratory failure, while the remaining two deaths appeared to be related to decompensation of pre-existing conditions, including malignancy, renal failure, and acute cardiac events. In these cases, SARS-CoV-2 infection most likely appears to function as a precipitating factor, rather than the sole cause of mortality.
To identify factors associated with disease severity, bivariate analysis was performed using hospitalization (hospitalization vs. home isolation) and mortality as outcomes. The presence of comorbidities was significantly associated with both hospitalization (p=0.001) and mortality (p=0.008). In contrast, history of previous infection (p=0.66 for hospitalization; p=0.32 for mortality), vaccination status (p=0.46 for hospitalization; p=1 for mortality), and symptomatic presentation (p=1 for hospitalization; p=1 for mortality) were not significantly associated with either hospitalization or mortality.
On multivariate analysis, with hospitalization as outcome, the presence of comorbidities was the only independent predictor of hospitalization (adjusted odds ratio (aOR) 4.12; 95% CI 1.68-10.10; p=0.002). No associations were observed for vaccination status (p=0.63), previous infection (p=0.31), or symptomatic presentation (p=0.85). Owing to the small number of deaths (n=4) observed, multivariate analysis with mortality as an outcome was not performed.
Discussion
The SARS-CoV-2 recombinant variant XFG, arising from recombination between LF.7 and LP.8.1.2, represents a notable evolutionary event during 2025. According to the WHO TAG-VE risk evaluation, XFG accounted for 22.7% of globally available sequences by epidemiological week 22 of 2025 (1,648 sequences from 38 countries), increasing sharply from 7.4% in week 19. This rise was observed across all WHO regions, with the most pronounced relative increase seen in the Southeast Asia region, where XFG rapidly replaced the previously dominant NB.1.8.1. However, in India, XFG emerged as the predominant circulating variant during spring 2025, while NB.1.8.1 remained uncommon [5], highlighting marked regional heterogeneity in variant replacement dynamics. Consistent with this expansion, as of January 2026, XFG demonstrates an estimated global relative growth advantage of approximately 19% [7].
The XFG variant carries a characteristic set of spike mutations compared to NB.1.8.1, including S31P, K182R, R190S, R346T, K444R, V445R, T478K, N487D, and T572I. When compared to the JN.1 variant, XFG displays the following spike mutations: T22N, S31P, K182R, R190S, R346T, K444R, V445R, F456L, N487D, Q493E, and T572I [5,1]. However, these mutations alone cannot establish heightened risk and must be interpreted in the context of prevalence and genomic background. Branda et al. used phylogenomic and phylodynamic analyses to show that the Bayesian Skyline Plot and Lineages-Through-Time trajectories of the XFG variant are consistent with a brief but intense expansion (during late March-April), followed by evolutionary stabilization (from May to July), indicative of a currently non-threatening variant [1]. This pattern suggests that the lineage took an extended time to acquire its key mutations, a behavior that is typically not observed in variants of concern. Furthermore, the estimated evolutionary rate for XFG (~4.4×10⁻⁴ substitutions per site per year) is comparable to other recent SARS-CoV-2 variants and is substantially lower than the early pandemic strains, supporting the interpretation of endemic-era evolution rather than a lineage with unusually accelerated evolutionary potential [1].
Further, multiple recent reports suggest that the rapid expansion of XFG is plausibly driven primarily by enhanced immune escape, rather than markedly improved receptor binding. In a comprehensive pseudovirus neutralization and ACE2 inhibition study of dominant JN.1 subvariants, XFG and NB.1.8.1 demonstrated a clear growth advantage over previously dominant LP.8.1.1 and showed lower serum neutralization titers compared with LP.8.1.1 across cohorts, with XFG exhibiting an approximately 1.9-fold reduction in geometric mean neutralizing titers in KP.2 monovalent vaccine recipients and significantly reduced titers in non-boosted individuals, supporting increased antibody evasion as a key correlate of dominance [8]. These findings are concordant with an independent post-KP.2 vaccination immunogenicity analysis, where neutralizing titers against XFG were markedly reduced (GMT ~17) relative to vaccine-matched KP.2 and ancestral WA.1 and antigenic cartography positioned emerging FLiRT-associated variants, including XFG, at substantial antigenic distances from KP.2, consistent with immune escape potential that may erode population-level neutralization [9]. XFG also showed ~2-fold lower NT50 in convalescent plasma from inactivated vaccine recipients with JN.1/XDV infections, compared to LP.8.1.1 [10]. Structurally, the spike of XFG harbors additional RBD changes (including H445R, N487D, and Q493E, along with T572I in SD1). The monoclonal antibody profiling suggests that XFG resistance is attributable to N487D and Q493E, in escape from class 1/2 (group B) antibodies [8,10]. Notably, despite this immune-evasive phenotype, all three studies indicate a trade-off with receptor engagement, reporting reduced ACE2-binding/engagement efficiency for XFG relative to LP.8.1.1 [8-10]. It is likely linked to structural effects of mutations such as N487D, which may introduce electrostatic repulsion at the ACE2 interface. These mutations likely promote an "RBD down" conformation, enhancing evasion despite 2.34-fold lower ACE2-binding affinity (higher IC50) and reduced pseudovirus entry vs. LP.8.1.1 [8,10]. Compensatory changes like R346T and T572I in SD1 may stabilize the spike, countering fitness costs and enabling XFG's transmission advantage [8]. Taken together, these data support an evolutionary trajectory in which XFG appears to have gained a transmission advantage chiefly through immune escape, potentially enabling widespread dissemination, an interpretation that is consistent with our observation of rapid spread.
In the present study, the clinical disease associated with the XFG variant was predominantly mild, with limited progression to severe outcomes. Our findings closely align with findings from a recent community-based surveillance study in the Netherlands, comparing SARS-CoV-2 variants circulating during 2024 (dominated by the KP.3 variant) and 2025 (dominated by the XFG variant). The study showed that XFG infection did not confer increased clinical severity compared to earlier Omicron-descendant variants such as KP.3. The symptom burden and overall disease severity, assessed using adjusted health scores and total symptom counts, were comparable between the two periods, reinforcing the absence of intrinsically more severe disease associated with XFG [11]. Among the hospitalized patients in our cohort, most required only conservative management, with supplemental oxygen, predominantly non-invasive, needed in a minority. Mortality was low and confined to elderly individuals with significant underlying comorbidities, suggesting that SARS-CoV-2 infection likely acted as a precipitating or aggravating factor rather than the sole cause of death, consistent with the evolving understanding of COVID-19 outcomes in vulnerable populations. The predominance of mild illness and favorable clinical outcomes in our cohort support the conclusion that XFG infection is not associated with increased disease severity. It is noteworthy that bivariate and multivariate analyses of hospitalized patients showed a significant association with comorbidities.
This study has several limitations. First, the analysis was dependent on the SARS-CoV-2 sequences uploaded to public databases, which are influenced by regional sequencing capacity, submission practices, and reporting delays, potentially introducing sampling bias. In addition, the findings are based on individuals who underwent SARS-CoV-2 testing, had their samples sequenced, and consented to participate, which may under-represent asymptomatic or untested infections and limit estimation of the true disease burden. As the clinical analysis was restricted to cases from Maharashtra, the generalizability of the findings to other regions with differing demographic and epidemiological profiles may be limited. Also, clinical data were collected through telephonic interviews and may be subject to recall/reporting bias. Furthermore, non-response may also influence estimates of disease severity. Thus, future studies incorporating broader geographic coverage, standardized sequencing efforts, and prospective clinical data collection would improve the representativeness and accuracy of assessments of emerging SARS-CoV-2 variants.
Conclusions
The XFG variant has emerged as the dominant SARS-CoV-2 variant globally during late 2024 and 2025, driving transient waves across the continents. In India, XFG circulated widely across multiple states, with a short-lived surge during mid-2025. In Maharashtra, where genomic trends closely paralleled epidemiological patterns, the infections were predominantly mild, manifesting as fever, cough, cold, body ache, and fatigue. Despite its attenuated virulence, the variant's rapid transcontinental spread and sublineage diversification underscore SARS-CoV-2's enduring immune evasion and adaptability. Fluctuations in testing volumes and sequencing submissions may underestimate the true burden of infection. This emphasizes the need for continued surveillance for the early detection of emerging variants and for strengthening preparedness against future waves.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1SARS-Co V-2 XFG: a genomic insight into the new recombinant Infect Dis (Lond) Branda F Ciccozzi M Scarpa F 101710205720254083953010.1080/23744235.2025.2548552 · doi ↗ · pubmed ↗
- 2COVID-19 - global situation 12 2025 2025 https://www.who.int/emergencies/disease-outbreak-news/item/2025-DON 572
- 3COVID-19 resurgence in Asia: a regional health alert J Biomed Sci Banerjee I Robinson J Singh AP 13122025
- 4Risk evaluation for SARS-Co V-2 variant under monitoring: NB.1.8.1 12 2025 2025 https://www.who.int/publications/m/item/risk-evaluation-for-sars-cov-2-variant-under-monitoring-nb.1.8.1
- 5Risk evaluation for SARS-Co V-2 variant under monitoring: XFG 12 2025 2025 https://www.who.int/publications/m/item/risk-evaluation-for-sars-cov-2-variant-under-monitoring-xfg
- 6GISAID's role in pandemic response China CDC Wkly Khare S Gurry C Freitas L 10491051320213493451410.46234/ccdcw 2021.255PMC 8668406 · doi ↗ · pubmed ↗
- 7XFG* (Nextclade) 1 2026 2024 https://cov-spectrum.org/explore/World/All Samples/from%3D 2024-01-01%26to%3D 2026-12-29/variants?nextclade Pango Lineage=XFG*&
- 8Antibody evasion and receptor binding of SARS-Co V-2 LP.8.1.1, NB.1.8.1, XFG, and related subvariants Cell Rep Mellis IA Wu M Hong H 1164404420254129656810.1016/j.celrep.2025.116715 PMC 12978314 · doi ↗ · pubmed ↗