Right ventricular stiffness as a key feature in the ZSF1 model of heart failure with preserved ejection fraction
Florian Schlotter, Karl-Patrik Kresoja, Karl-Philipp Rommel, Lena Rosenbusch, Sarah Werner, Urvashi Sharma, Holger Thiele, Christian Besler, Philipp Lurz, Petra Büttner

TL;DR
The study shows that right ventricular stiffness in a rat model of heart failure with preserved ejection fraction is due to myocytic stiffening, not fibrosis.
Contribution
The study identifies myocytic stiffening as the primary driver of right ventricular diastolic dysfunction in a rat model of HFpEF.
Findings
Obese ZSF1 rats showed increased right and left ventricular stiffness with preserved right ventricular contractility.
RV stiffness correlated with LV stiffness, indicating biventricular diastolic dysfunction.
RV and septal cardiomyocyte hypertrophy was observed without changes in myocardial fibrosis.
Abstract
Heart failure with preserved ejection fraction (HFpEF) is a heterogeneous syndrome defined by diastolic dysfunction and limited therapeutic options, with increasing recognition of right ventricular (RV) involvement. Using invasive pressure-volume loop analysis, we assessed biventricular hemodynamics in lean and obese ZSF1 rats, a well-established rodent model of HFpEF. Obese rats exhibited significantly increased RV and left ventricular (LV) chamber stiffness, with a positive correlation between RV and LV stiffness constants, indicating biventricular diastolic dysfunction. RV end-systolic elastance was preserved, whereas LV contractility was increased. Despite elevated RV stiffness, myocardial fibrosis was unchanged, while RV and septal cardiomyocyte hypertrophy was significantly increased. These findings demonstrate that RV diastolic dysfunction in this HFpEF model is driven primarily…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
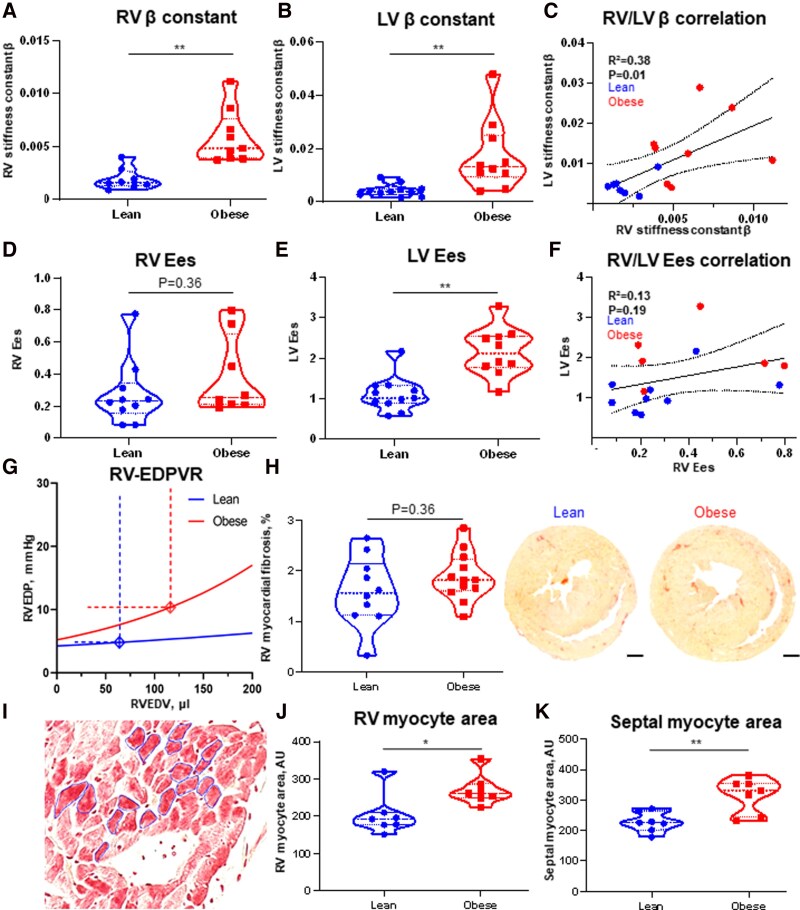 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Function and Risk Factors · Cardiac Fibrosis and Remodeling · Pulmonary Hypertension Research and Treatments
Heart failure with preserved ejection fraction (HFpEF) remains a significant clinical and scientific challenge, with limited effective therapeutic options. Its prevalence continues to rise, partly attributable to an aging population and common comorbidities such as hypertension, obesity, and metabolic disease. Advancing mechanistic insight and developing targeted therapies remain critical unmet needs. Preclinical research in HFpEF relies heavily on the assessment of in vivo physiological conditions, as the syndrome is primarily defined by functional haemodynamic alterations, namely changes in diastolic function, rather than distinct structural cardiac abnormalities. Subtle impairments in ventricular relaxation, compliance, and filling pressures are highly dynamic and influenced by loading conditions, making rigorous in vivo phenotyping essential for accurately modelling the disease and evaluating therapeutic efficacy. To date, only a limited number of in vivo models for HFpEF were developed, and each presents specific limitations in their ability to fully replicate the complex haemodynamic profile characteristic of the human condition.^1,2^ The current understanding of HFpEF pathophysiology recognizes it as a heterogenous and systemic disorder, involving not only the left ventricle (LV) and atrium but also the right ventricle (RV). Several mechanisms have been proposed to explain RV involvement, which may exacerbate the clinical manifestations and progression of HFpEF.
Invasive pressure-volume loop (PVL) analysis remains the reference standard for detailed haemodynamic assessment of cardiac function.^3^ However, to date, RV physiology has not been systematically evaluated using PVL analysis in rodent models of HFpEF, representing a gap in the preclinical characterization of this syndrome. In human HFpEF, major haemodynamic determinants of RV function include elevated end-diastolic RV pressures and increased chamber stiffness.^4^
Few preclinical models that recapitulate the hemodynamically defined HFpEF pathophysiology are available.^2^ The Zucker fatty and spontaneously hypertensive heart failure rate (ZSF1) serves as a widely used preclinical model for HFpEF and recapitulates major phenotypic traits of HFpEF, including concentric LV hypertrophy, preserved systolic function, diastolic dysfunction and exercise intolerance, as well as increased arterial stiffness, and insulin resistance.^2,5^
In this rodent model of HFpEF, lean (control) and obese ZSF1 rats (ZSF1-Lepr^fa^Lepr^cp^/Crl, Charles River, Kingston, USA; animal test reference number TVV 30/18) were studied at 20 weeks of age. Lean ZSF1 rats, that carry at least one functional leptin receptor allele exhibit normal metabolic and cardiac function and served as controls,^6^ whereas obese ZSF1 rats, homozygous for a leptin receptor mutation, develop obesity and HFpEF-like diastolic dysfunction. Animals were maintained on standard rat chow (RM1, SDS, Essex, UK) for 12 weeks starting at 8 weeks of age. For PVL analysis, a 1.49F pressure-volume catheter (Transonic Scisense Inc.) was introduced into the right ventricle via the right jugular vein and into the left ventricle via the carotid artery. In total, 12 lean and 12 obese ZSF1 rats were included in the analysis. PVL tracings were only included in the final analysis, if deemed suitable by two independent observers.
Body weights, heart weights and heart weight to tibia length ratios were significantly higher in obese rats [body weight: lean: 232 g (227 g; 254 g); obese: 467 g (450 g; 486 g); P < 0.01; heart weight: lean: 942 mg (896 mg; 963 mg); obese: 1355 mg (1323 mg; 1420 mg); P < 0.01; heart weight to tibia length ratio: lean: 25.7 (24.33; 26.10); obese: 36.70 (36.15; 38.50); P < 0.01].
Obese ZSF1 rats exhibited significantly increased RV stiffness compared with lean control rats. Specifically, the RV stiffness constant β was markedly elevated in obese rats [Figure 1 panel A: lean ZSF1, β = 0.0016 (0.0013; 0.0026); obese, β = 0.0048 (0.0039; 0.0076); P < 0.01]. Likewise, the LV stiffness constant β was significantly greater in obese ZSF1 rats than in their lean counterparts [Figure 1 panel B: lean, β = 0.0039 (0.0027; 0.0049); obese, β = 0.0132 (0.0093; 0.0251); P < 0.01]. A correlation between RV and LV stiffness constants was observed (Figure 1 panel C: R² = 0.38, P < 0.05).
RV end-systolic elastance (Ees), defined as the slope of the end-systolic pressure-volume relationship (ESPVR), a load-independent measure of ventricular contractility that reflects the ventricle’s contractile adaptation to increased afterload, did not differ significantly between lean and obese ZSF1 rats [Figure 1 panel D: lean, Ees = 0.23 (0.15; 0.34); obese, Ees = 0.25 (0.21; 0.65); P = 0.36]. In contrast, LV Ees was significantly increased in obese rats [Figure 1 panel E: lean, Ees = 1.01 (0.09; 2.17); obese, Ees = 2.12 (1.76; 2.54); P < 0.01]. No significant correlation was found between RV and LV Ees values (Figure 1 panel F: R² = 0.13, P = 0.19).
The RV end-diastolic pressure-volume relationship (EDPVR) in obese rats was steeper and left-shifted (Figure 1 panel G), indicating increased RV chamber stiffness and impaired diastolic function.
Interestingly, RV myocardial fibrosis, quantified by picrosirius red staining, did not differ significantly between the groups [Figure 1 panel H: lean, 1.6% picrosirius-positive area (1.1%; 2.1%); obese, 1.8% (1.6%; 2.2%); P = 0.31]. However, RV myocyte area, a marker of hypertrophy, was significantly larger in obese rats [Figure 1 panel I, J: lean, 192 arbitrary units (AU) (177; 320); obese, 261 AU (249; 287), P < 0.05]. Similarly, septal myocyte area was greater in obese rats compared with lean controls [K: lean, 226 AU (202; 265); obese, 332 AU (244; 354), P < 0.01].
Despite technical challenges, comprehensive assessment of RV hemodynamics is essential for a full understanding of HFpEF, given the increasingly recognized role of biventricular involvement in disease progression. Here, we provide invasive haemodynamic evidence of RV diastolic dysfunction in a well-established in vivo HFpEF model. Obese ZSF1 rats exhibited markedly increased RV chamber stiffness and impaired diastolic properties, closely resembling key features observed in human HFpEF. The correlation between RV and LV stiffness supports the presence of shared pathophysiological mechanisms underlying biventricular diastolic dysfunction. Of note, increased RV stiffness occurred in the absence of enhanced myocardial fibrosis, indicating that extracellular matrix remodeling is unlikely to be the primary driver. Instead, significant RV myocyte hypertrophy points to myocytic stiffening as a major contributor.^7^ Our study corroborates prior human data, provides new mechanistic insight into RV involvement in HFpEF, and further validates the ZSF1 rat as a translationally relevant in vivo model that captures key biventricular features of HFpEF.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schiattarella GG, Altamirano F, Tong D, French KM, Villalobos E, Kim SY et al Nitrosative stress drives heart failure with preserved ejection fraction. Nature 2019;568:351–6.30971818 10.1038/s 41586-019-1100-z PMC 6635957 · doi ↗ · pubmed ↗
- 2Valero-Muñoz M, Backman W, Sam F. Murine models of heart failure with preserved ejection fraction: a “fishing expedition”. JACC Basic Transl Sci 2017;2:770–89.29333506 10.1016/j.jacbts.2017.07.013PMC 5764178 · doi ↗ · pubmed ↗
- 3Brener MI, Masoumi A, Ng VG, Tello K, Bastos MB, Cornwell WK III et al Invasive right ventricular pressure-volume analysis: basic principles, clinical applications, and practical recommendations. Circ Heart Fail 2022;15:e 009101.34963308 10.1161/CIRCHEARTFAILURE.121.009101 PMC 8766922 · doi ↗ · pubmed ↗
- 4Rommel K-P, von Roeder M, Oberueck C, Latuscynski K, Besler C, Blazek S et al Load-independent systolic and diastolic right ventricular function in heart failure with preserved ejection fraction as assessed by resting and handgrip exercise pressure–volume loops. Circ Heart Fail 2018;11:e 004121.29449367 10.1161/CIRCHEARTFAILURE.117.004121 · doi ↗ · pubmed ↗
- 5Schauer A, Draskowski R, Jannasch A, Kirchhoff V, Goto K, Männel A et al ZSF 1 rat as animal model for H Fp EF: development of reduced diastolic function and skeletal muscle dysfunction. ESC Heart Fail 2020;7:2123–34.32710530 10.1002/ehf 2.12915 PMC 7524062 · doi ↗ · pubmed ↗
- 6Büttner P, Augstein A, Abdellatif M, Lourenço A, Leite-Moreira A, Falcão-Pires I et al Lean ZSF 1 rats in basic research on heart failure with preserved ejection fraction. ESC Heart Fail 2025;12:1474–8.39663741 10.1002/ehf 2.15111 PMC 11911634 · doi ↗ · pubmed ↗
- 7Rosch S, Kresoja K-P, Besler C, Fengler K, Schöber AR, von Roeder M et al Characteristics of heart failure with preserved ejection fraction across the range of left ventricular ejection fraction. Circulation 2022;146:506–18.35862208 10.1161/CIRCULATIONAHA.122.059280 · doi ↗ · pubmed ↗