Cryptococcus neoformans Meningitis in a Patient With Epidermolysis Bullosa and Rheumatoid Arthritis
Kay Lin Ng, Karunamuni I Karunaratne

TL;DR
A 59-year-old HIV-negative woman with two autoimmune conditions developed Cryptococcus neoformans meningitis and was successfully treated with a combination of antifungal therapy and surgical interventions.
Contribution
This case highlights the rare occurrence of cryptococcal meningitis in an HIV-negative patient with autoimmune disorders and immunosuppressive therapy.
Findings
Cryptococcus neoformans meningitis can occur in HIV-negative individuals on immunosuppressive drugs.
Aggressive antifungal treatment and neurosurgical interventions led to clinical improvement in the patient.
Abstract
Cryptococcal meningitis (CM) is an opportunistic fungal infection with a high mortality rate commonly associated with those with human immunodeficiency virus (HIV) or acquired immunodeficiency syndrome (AIDS). The epidemiology of CM in HIV-negative individuals is unclear, although it is estimated to be increasing in developed countries. We present a case of Cryptococcus neoformans meningitis in a 59-year-old HIV-negative female taking long-term mycophenolate (MMF) for epidermolysis bullosa acquisita (EBA) and upadacitinib for rheumatoid arthritis (RA). With an aggressive antifungal regimen, therapeutic lumbar punctures, lumbar drain insertion, and ventriculoperitoneal shunt insertion, the patient's condition improved, and she was discharged from the hospital.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
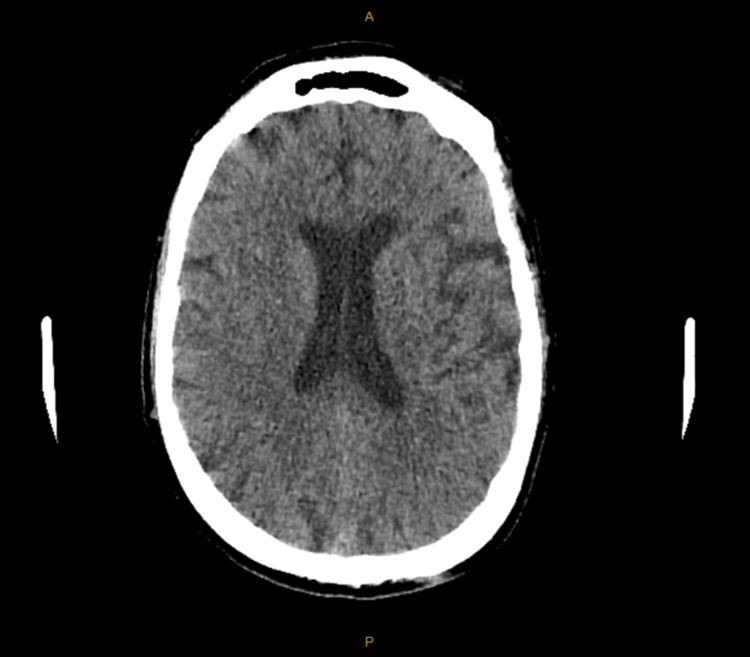 Figure 1
Figure 1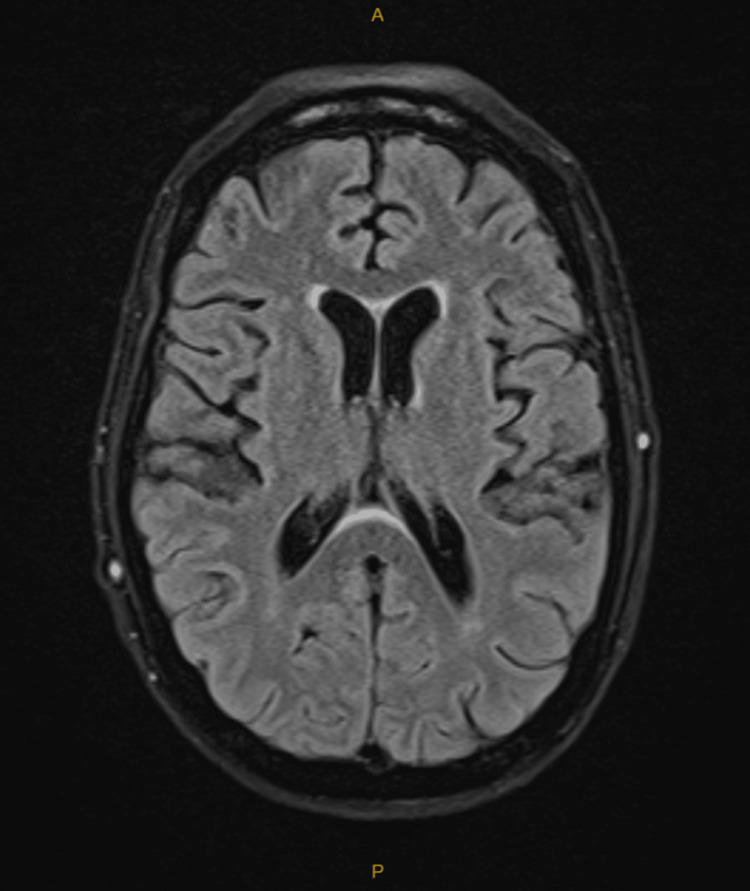 Figure 2
Figure 2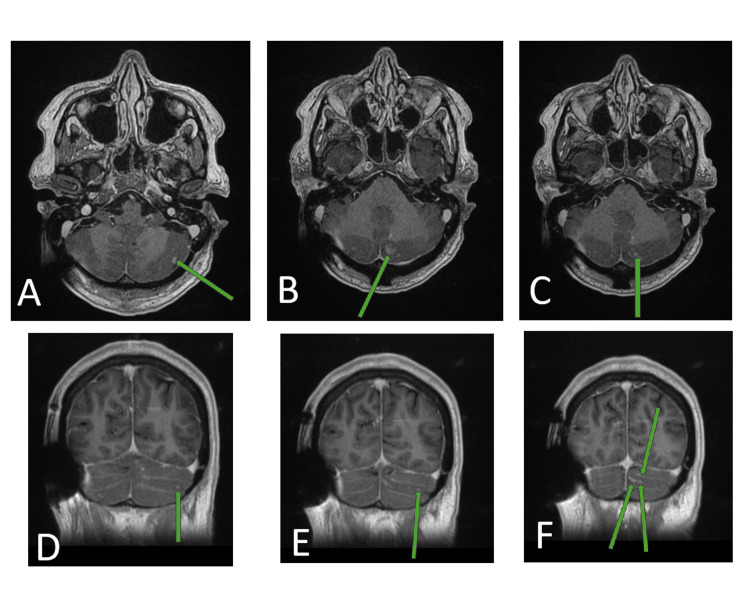 Figure 3
Figure 3| Parameters | Day 1 (22/5/25) | Day 2 (23/5/25) | Day 3 (24/5/25) | Day 4 (25/5/25) | Day 5 (26/5/25) | Day 6 (27/5/25) | Units | Reference Range |
| Sodium | 130 (L) | 132 (L) | 138 | 141 | 131 (L) | 133 (L) | mmol/L | 135–145 |
| Potassium | 2.6 (L) | 3.7 | 3.4 (L) | 3.5 | 3.0 (L) | 2.8 (L) | mmol/L | 3.5–5.5 |
| Chloride | 85 (L) | 95 | 103 | 103 | 93 (L) | 96 | mmol/L | 95–110 |
| Urea | 4.4 | 4.5 | 4.2 | 5.2 | 4.8 | 5.8 | mmol/L | 3.0–8.0 |
| Creatinine | 73 | 61 | 59 | 63 | 60 | 78 | µmol/L | 45–85 |
| eGFR | 78 (L) | >90 | >90 | >90 | >90 | 72 | mL/min/1.73 m2 | >89 |
| Bicarbonate | 28 | 27 | 25 | 25 | 22 | 25 | mmol/L | 20–32 |
| Total bilirubin | 19 (H) | - | - | - | - | 21 (H) | µmol/L | 3–15 |
| ALP | 50 | - | - | - | - | 50 | U/L | 30–115 |
| GGT | 22 | - | - | - | - | 30 | U/L | 5–35 |
| ALT | 14 | - | - | - | - | 21 | U/L | 5–30 |
| Total protein | 65 | - | - | - | - | 60 (L) | g/L | 63–80 |
| Albumin | 39 | - | 31 (L) | 30 (L) | 34 | 34 | g/L | 33–44 |
| Globulin | 26 | - | - | - | - | 26 | g/L | 26–41 |
| Total calcium | 2.35 | - | 2.14 (L) | 2.19 | 2.20 | 2.19 | mmol/L | 2.15–2.55 |
| Corrected calcium | 2.37 | - | 2.32 | 2.39 | 2.32 | 2.31 | mmol/L | 2.20–2.60 |
| Phosphate | 1.02 | - | 0.87 | 1.12 | 1.34 | 1.09 | mmol/L | 0.8–1.5 |
| Magnesium | 0.83 | - | 0.78 | 0.76 | 0.72 | 1.03 | mmol/L | 0.70–1.05 |
| Haemoglobin | 141 | 122 | 118 | 112 (L) | 137 | 143 | g/L | 115–165 |
| HCT | 0.38 | 0.35 (L) | 0.34 (L) | 0.33 (L) | 0.40 | 0.42 | L/L | 0.36–0.47 |
| MCV | 84 | 86 | 90 | 90 | 90 | 88 | n/L | 80–100 |
| WBC | 1.3 (L) | 0.9 (L) | 1.0 (L) | 1.1 (L) | 1.4 (L) | 3.7 (L) | n/L | 4.0–11.0 |
| Neutrophils | 0.2 (L) | 0.2 (L) | 0.2 (L) | 0.1 (L) | 0.2 (L) | 1.2 (L) | n/L | 2.0–7.5 |
| Lymphocytes | 0.5 (L) | 0.3 (L) | 0.3 (L) | 0.5 (L) | 0.6 (L) | 0.8 (L) | n/L | 1.0–4.0 |
| Monocytes | 0.6 | 0.5 | 0.6 | 0.6 | 0.6 | 1.7 (H) | n/L | 0.2–1.0 |
| Eosinophils | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 | n/L | <0.5 |
| Basophils | < 0.1 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 | n/L | <0.3 |
| Platelets | 233 | 195 | 156 | 131 (L) | 113 (L) | 86 (L) | n/L | 150–400 |
| nRBC | - | - | - | 2.7 (H) | 6.5 (H) | 1.6 (H) | /100 WBCs | <1.0 |
| Troponin | 25 (H) | - | - | - | - | 19 (H) | ng/L | <16 |
| CRP | 20 (H) | 16 (H) | 8 (H) | 4 | 14 (H) | 27 (H) | mg/L | <5 |
| Parameters | Day 1 (22/5/25) | Day 2 (23/5/25) | Day 3 (24/5/25) | Units | Reference Range |
| INR | 0.9 | - | 1.0 | - | 0.9–1.2 |
| APTT | 27 | - | 23 | Seconds | 25–35 |
| Fibrinogen | 4.1 | - | 2.5 | g/L | 2.0–4.5 |
| Thrombin time | 20 | - | 20 | Seconds | 15–22 |
| Syphilis antibody | - | Non-reactive | - | - | - |
| Blood culture | Nil growth | - | - | - | - |
| HIV ½ antigen/antibody | - | Not detected | - | - | - |
| Parameters | Day 1 (22/5/25) | Day 2 (23/5/25) | Day 5 (26/5/25) | Day 6 (27/5/25) |
| COVID/Influenza A/Influenza B/RSV swab | Negative | - | - | - |
|
| Negative | - | - | - |
| Rhinovirus/Parainfluenza/Human Metapneumovirus/Adenovirus swab | Rhinovirus positive | - | - | - |
| Urine | - |
| Urine MCS: Glucose Nil, Specific gravity 1.012, Protein Nil Ketones Trace, Blood +, Nitrite Nil, pH 8, Leucocytes < 3, Erythrocytes 30 (H), squamous epithelial cells < 5, no bacterial growth | - |
| MRSA swab (nose, throat, groin) | - | - | - | Negative |
| VRE swab (rectum) | - | - | - | VRE ( |
| CPO – Carbapenemase (rectum) | - | - | - | Negative |
| Parameters | Day 1 (22/5/25) | Day 3 (24/5/25) | Day 5 (26/5/25) | Day 6 (27/5/25) On transfer to tertiary hospital |
| Opening pressures | - | 21 cm H2O | >35 cm H2O (H) | - |
| Tube 1 | Protein 735 mg/L (H) Glucose 1.3 mmol/L (L) Polymorphs 18 x 106/L (H) Lymph/Mono 7 x 106/L (H) Erythrocytes 136 x 106/L (H) | Protein 580 mg/L (H) Glucose 2.5 mmol/L Polymorphs 20 x 106/L (H) Lymph/Mono 80 x 106/L (H) Erythrocytes 200 x 106/L (H) | Protein 1314 mg/L (H) Glucose 1.3 mmol/L (L) Polymorphs 2 x 106/L (H) Lymph/Mono 92 x 106/L (H) Erythrocytes 0 x 106/L | Protein 1.04 g/L (H) Glucose 1.04 mmol/L (L) Polymorphs < 1 x 106/L Lymphocytes 89 x 106/L (H) Erythrocytes 6 x 106/L (H) Total Leucocytes 89 x 106/L (H) |
| Tube 2 | Polymorphs 17 (H) Lymph/Mono 5 (H) Erythrocytes 119 (H) | Polymorphs 60 (H) Lymph/Mono 70 (H) Erythrocytes 50 (H) | - | - |
| Tube 3 | Polymorphs 13 (H) Lymph/Mono 7 (H) Erythrocytes 96 (H) | Polymorphs 20 (H) Lymph/Mono 90 (H) Erythrocytes 230 (H) | - | - |
| CSF Culture |
| Cryptococcus neoformans | No growth after 48 hours of microscopic incubation: Smear is moderately cellular and shows prominent small mature lymphocytes and histiocytes. No definite cryptococcal organisms are seen. Diagnosis: cerebrospinal fluid: Negative for malignancy |
|
| CSF Antigen | Cryptococcal antigen: detected titre 1:1280 | - | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Nail Diseases and Treatments · Infectious Diseases and Tuberculosis
Introduction
Cryptococcal meningitis (CM) is an opportunistic infection acquired through inhalation of aerosolised particles from bird guano or mopane trees [1,2]. It has a high mortality rate of 19% in those with HIV and AIDS, with around one million cases of cryptococcosis globally and 625,000 deaths each year [3-5].
In 2014, there were approximately 223,100 cases of CM globally, although this number may be larger, as only a few states in the United States of America report their data [3]. In the literature, high-risk patients include those with advanced HIV infections, immune suppression, or solid organ transplantation [1,5]. The exact epidemiology of CM in HIV-negative individuals is unclear, although it is estimated to be increasing in developed countries [4-6]. An aggressive antifungal regimen is required and is often associated with elevated intracranial pressure, requiring repeated therapeutic lumbar punctures or the insertion of drains or shunts [1,3,5,7]. In immunocompetent individuals, cryptococcal invasion is cleared by macrophages and by cytokines such as interferon-γ (IFN-γ), tumour necrosis factor-α (TNF-α), and granulocyte-macrophage colony-stimulating factor (GM-CSF) [8]. For immunocompromised individuals, macrophages and downstream cytokines are suppressed, precluding to cryptococcal infection.
We present a case of Cryptococcus neoformans meningitis in an HIV-negative, transplant-negative patient taking long-term mycophenolate (MMF) for epidermolysis bullosa acquisita (EBA) and upadacitinib for rheumatoid arthritis (RA). There have been some cases of CM reported in those who take MMF and have RA or are taking concurrent long-term steroids with biologics or disease-modifying anti-rheumatic drugs (DMARDs). There are now new reports of CM in those who take JAK inhibitors. However, there have been no reports associated with EBA nor any case reports with the individual taking a combination of MMF and upadacitinib. This case further highlights a case of CM in a patient from a developing country who does not have HIV, does not have a solid organ transplant, and is on combined cumulative immunosuppression with MMF and JAK inhibitors.
Case presentation
A 59-year-old Caucasian woman living in rural northwest Tasmania presented with a two-week history of worsening headache preceded by a respiratory illness and a three-day history of subjective fevers and confusion, such as becoming disoriented, difficulty speaking, urinary incontinence, childlike behaviour, reduced appetite, and mildly impaired gait.
Relevant medical history included EBA, diagnosed approximately 15 years ago. She has been on courses of immunosuppressive therapies, including topical steroids (clobetasol and betamethasone dipropionate), one year of intravenous immunoglobulin (IVIG) in 2013-2014, azathioprine, dapsone, rituximab, and mycophenolate. In addition to this, she was treated for her seronegative RA and was previously on methotrexate, leflunomide, and hydroxychloroquine. At the time of presentation, she had been taking mycophenolate 1000 mg twice daily for 10 years for EBA and upadacitinib 15 mg daily for RA for five years. Complications related to this immunosuppressive history include febrile neutropenia secondary to infusion port sepsis with Staphylococcus lentus-positive blood cultures in 2013, Herpes simplex virus (HSV) keratitis in the right eye, and left-sided Cytomegalovirus (CMV) retinitis occurring a year prior to presentation.
On examination, there was drowsiness and a Glasgow Coma Scale of 14 (E4V4M6). There was no other focal neurology. Blood tests showed a C-reactive protein (CRP) level of 20 (normal range: <5 mg/L), troponin I of 25 (normal: <16 ng/L), sodium of 130 (normal: 135-145 mmol/L), potassium of 2.5 (normal: 3.5-5.5 mmol/L), estimated glomerular filtration rate of 78 (normal: >89 mL/min/1.73 m^2^), white cell count of 1.3 (normal: 4.0-11.0/nL), neutrophils of 0.2 (normal: 2.0-7.5/nL), and lymphocytes of 0.5 (normal: 1.0-4.0/nL) (Table 1).
The remaining blood tests were normal, including nil growth in blood cultures (Table 2). The respiratory viral swab was positive for rhinovirus. Urinary antigens for Streptococcus pneumoniae and HIV, CMV, and syphilis serology were negative (Table 3). The patient's hypokalaemia was treated accordingly with intravenous potassium replacement, and with her neutropenia, her mycophenolate and upadacitinib were withheld in the context of a potential meningitis. Initial lumbar puncture opening pressures were not recorded; however, the cerebrospinal fluid showed protein levels of 735 (normal: 150-450 mg/L), glucose of 1.3 (normal: 2.2-3.9 mmol/L), polymorphs of 18 (normal: <1x10^6^/L), lymphocytes/monocytes of 7 (normal: <5x10^6^), and erythrocytes of 136 (normal: <1x10^6^/L), and subsequently a positive culture of Cryptococcus neoformans with an antibody titre of 1:1280 and a positive India ink stain (Tables 3, 4).
The brain CT showed no intracranial abnormalities, and the brain MRI reported no acute infarcts, no space-occupying lesions, and no evidence of meningitis or encephalitis (Figures 1, 2).
CT Brain Scan With Contrast Day 1 - Normal StudyCT: computerised tomography
MRI Brain T2 FLAIR With Contrast Day 2 - Normal StudyMRI: magnetic resonance imaging, T2 FLAIR: T2-weighted fluid-attenuated inversion recovery
The patient was commenced on amphotericin B 250 mg daily and oral flucytosine 2000 mg six-hourly. A chest X-ray was completed, which did not show any pulmonary disease. A repeat lumbar puncture done two days after the initial positive CSF culture showed an opening pressure of 21 cmH₂O, a protein of 580 mg/L, glucose of 2.5 mmol/L, polymorphs of 20x10^6^/L, lymphocytes/monocytes of 80x10^6^/L and was culture positive for Cryptococcus neoformans (Table 4). Two days later, an additional lumbar puncture was done due to increased somnolence: this demonstrated a significantly increased opening pressure of >35 cmH₂O, with protein of 1314 mg/L, glucose of 1.3 mmol/L, polymorphs of 2x10^6^/L, and lymphocytes/monocytes of 92x10^6^/L (Table 4).
With a significant increase in opening CSF pressure in 48 hours, risk of neurodeterioration, and a likely requirement of daily lumbar punctures in a rural hospital, she was transferred to a tertiary hospital under the Neurosurgery team for insertion of a lumbar drain, then subsequently an insertion of a ventriculoperitoneal shunt and completion of her course of antifungals. A subsequent MRI of the spine on Day 23 of admission showed small volume leptomeningeal enhancement in the posterior fossa consistent with known meningitis (Figure 3).
MRI Brain and Spine T1 With Contrast Showing Small Volume Leptomeningeal Enhancement in the Posterior Fossa (A–F)A–C: Axial MRI (T1 with contrast) with progressively caudal slices showing small volume leptomeningeal enhancement in the posterior fossaD–F: Coronal MRI (T1 with contrast) with progressively posterior slices showing small volume leptomeningeal enhancement in the posterior fossaMRI: magnetic resonance imaging
Flucytosine was withheld prior to two weeks’ duration due to pancytopaenia, and amphotericin B was continued for two weeks before stepping down to fluconazole 400 mg daily for eight weeks and reduced to 200 mg daily for one year. Ophthalmology reviewed the patient towards the end of her hospital stay and visualised mild bilateral papilloedema, likely secondary to her cryptococcal infection, but no recurrence of HSV keratitis or CMV retinitis. The patient’s discharge plan was an ongoing follow-up with Neurology, Infectious Diseases, and Ophthalmology. Two months post-discharge, she was recommenced on upadacitinib by her rheumatologist with no reported relapse as of seven months post-discharge. All other immunosuppression, including mycophenolate, has been withheld, and she will have ongoing Dermatology review for her EBA.
Discussion
General risk factors for non-HIV individuals acquiring CM include corticosteroid treatment, solid organ transplantation, liver cirrhosis, cancer, monoclonal antibodies, sarcoidosis, and tyrosine kinase inhibitors [2,4-7]. At the time of writing, there is no specific literature on EBA patients who develop CM due to immunosuppression. A recent retrospective case-control study described the characteristics of 20 patients with RA who developed cryptococcal infections, all of whom were on long-term corticosteroids (3.9±3.3 years), 65.0% were over 60 years of age, and 65.0% were female [9]. The study identified specific risk factors, including corticosteroids, chronic kidney disease, and adalimumab, none of which our patient was taking at the time of presentation [9]. Some patients were concurrently taking prednisolone with DMARDs and biologics such as anti-TNF and etanercept, though it was not specified what each individual patient was taking [9]. There was also one case report of a patient taking prednisolone and etanercept simultaneously at the time of developing CM [10].
The pathogenesis of CM is poorly understood and can either progress post-primary infection (pulmonary cryptococcus) rapidly or reside in phagocytes for up to 110 months (approximately nine years) in C. neoformans [5]. As our patient had been on both MMF and upadacitinib for the last five years and had previously undergone extensive immunosuppression, perhaps it was the recent primary respiratory illness that preceded our patient’s onset of CM, rather than an infection that had been dormant for years in the context of immunosuppression.
One limitation to be acknowledged was that the lumbar puncture opening pressure was not recorded at the patient's initial presentation. It is therefore unknown whether the patient presented with high opening pressures or whether this had developed during her hospital stay.
Some cases of CM have been reported in patients taking mycophenolate, and evidence from zebrafish models suggests that the pathway affects macrophages [11]. JAK inhibitors dampen multiple cytokines, including IFN-γ and GM-CSF, essential cytokines for the clearance of cryptococcal infections [8]. A 2024 literature review identified three published reports of patients on ruxolitinib, a JAK inhibitor, who were not on MMF and who subsequently developed CM [8]. Upadacitinib was approved by the FDA in August 2019, and there are warnings associated with pulmonary cryptococcosis and bacterial meningitis, but not specifically CM [12]. As of February 2026, there are no publications related to CM in which a patient is simultaneously on upadacitinib and mycophenolate.
Some studies suggest that the in-hospital mortality of HIV-negative people with CM is higher than that of those with HIV [4]. It is therefore important to raise awareness of the risk of CM in HIV-negative individuals on multiple immunosuppressants or novel therapies, such as JAK inhibitors, which are used to treat a wide variety of autoimmune conditions.
Conclusions
The risk of occurrence of CM in HIV-negative patients is not fully known and brings awareness to a potentially vulnerable population group in immunosuppressed individuals who are not transplant recipients, especially those taking new targeted therapies such as JAK-2 inhibitors or who are on more than one immunosuppressive therapy.
This case emphasises the need for heightened clinical awareness of CM and to consider individuals who may be taking targeted or multiple immunosuppression therapies. Future research should aim to elucidate the risk of CM for HIV-negative individuals taking older immunosuppressants such as MMF, newer biologics such as JAK inhibitors, or those taking more than one immunosuppressive medication and assess effective screening and treatment strategies for these complex presentations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cryptococcosis Harrison's Principles of Internal Medicine Casadevall A 16691670 Columbus (OH)Mc Graw-Hill Education 2022 https://accesspharmacy.mhmedical.com/content.aspx?bookid=3095§ionid=265435208
- 2Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 9th Edition Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 9th Edition Bennett JE Dolin R Blaser MJ 31463161 Amsterdam, Netherlands Elsevier 2020 https://shop.elsevier.com/books/mandell-douglas-and-bennetts-principles-and-practice-of-infectious-diseases/bennett/978-0-323-48255-4
- 3Cryptococcosis and cryptococcal meningitis: a narrative review and the up-to-date management approach Cureus Qureshi ZA Ghazanfar H Altaf F 016202410.7759/cureus.55498 PMC 1099006738571832 · doi ↗ · pubmed ↗
- 4Cryptococcal meningitis Nat Rev Dis Primers Tugume L Ssebambulidde K Kasibante J 62920233794568110.1038/s 41572-023-00472-z · doi ↗ · pubmed ↗
- 5Reframing the clinical phenotype and management of cryptococcal meningitis Pract Neurol Rocha MF Bain HD Stone N 25392520253899713610.1136/pn-2024-004133 PMC 11877062 · doi ↗ · pubmed ↗
- 6Clinical manifestations and diagnosis of Cryptococcus neoformans meningoencephalitis in patients without HIV Up To Date Cox GM Perfect JR Waltham, MA Up To Date 2025 https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-cryptococcus-neoformans-meningoencephalitis-in-patients-without-hiv
- 7Cryptococcus neoformans: treatment and prevention of meningoencephalitis and disseminated infection in patients without HIV Up To Date 1 2026 Cox GM Perfect JR Waltham, MA Up To Date 2024 https://www.uptodate.com/contents/cryptococcus-neoformans-treatment-and-prevention-of-meningoencephalitis-and-disseminated-infection-in-patients-without-hiv
- 8Cryptococcosis associated with biologic therapy: a narrative review Open Forum Infect Dis Li X Paccoud O Chan KH 011202410.1093/ofid/ofae 316PMC 1121200938947739 · doi ↗ · pubmed ↗