Effects of rhythmic dumbbell upper limb rehabilitation training based on the multi-process action control framework on vascular access function and quality of life in hemodialysis patients
Jing Hu, Mingcong Cao, Rufu Jia, Keli Pan, Xuelian Jiang

TL;DR
A study found that rhythmic dumbbell exercises based on a specific control theory improved vascular function and quality of life in hemodialysis patients.
Contribution
This study introduces a novel rehabilitation approach using rhythmic dumbbell exercises based on the M-PAC framework for hemodialysis patients.
Findings
The intervention group showed significantly better AVF maturation and blood flow outcomes compared to the control group.
Quality of life scores improved more in the intervention group after the rehabilitation program.
Single-needle puncture success rates were higher in the intervention group post-exercise.
Abstract
To investigate the effects of rhythmic dumbbell upper limb rehabilitation exercise based on multi-process action control (M-PAC) theory on the function and quality of life of autogenous arteriovenous fistula in hemodialysis patients. A total of 72 patients who underwent autologous arteriovenous fistula (AVF) angioplasty and had stable and regular dialysis in the hemodialysis center of Cangzhou Central Hospital from January 2025 to April 2025 were selected as the research subjects, and were randomly divided into control group (n = 36) and intervention group (n = 36). Both groups were given routine rehabilitation management. The control group was given routine ball-holding rehabilitation exercise on the upper limb of the AVF side, and the intervention group was given rhythmic dumbbell rehabilitation exercise based on M-PAC theory. The intervention began 2 weeks after the operation, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
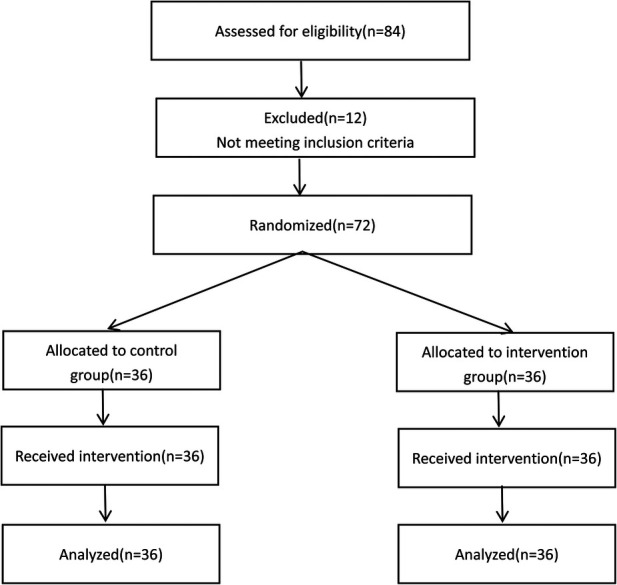 Figure 1
Figure 1| Group |
| Gender (male/female) | Age (years) | Kidney disease stage (stage 4/stage 5) | Primary etiology | Dialysis via CVC before AVF use (yes/no) | AVF side (left/right) | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Glomerulonephritis | Diabetes | Hypertension | Others | |||||||
| Control group | 36 | 21/15 | 55.33 ± 12.57 | 12/24 | 10 | 12 | 8 | 6 | 20/16 | 26/10 |
| Intervention group | 36 | 19/17 | 53.14 ± 12.07 | 15/21 | 13 | 10 | 8 | 5 | 18/18 | 22/14 |
| 0.225 | 0.756 | 0.533 | 0.664 | 0.056 | 0.563 | |||||
| 0.635 | 0.452 | 0.465 | 0.882 | 0.813 | 0.453 | |||||
| Variable | Group |
| Test | |||
|---|---|---|---|---|---|---|
| Cephalic vein blood flow (mL/min) | Control group | 36 | Post-intervention | 857.33 ± 117.41 | ||
| Intervention group | 36 | Post-intervention | 1,214.53 ± 146.28 | |||
| Difference between groups post-treatment | 357.19 ± 199.57 | 11.426 | <0.001 | |||
| Venous diameter (mm) | Control group | 36 | Pre-intervention | 2.25 ± 0.65 | −14.962 | <0.001 |
| Post-intervention | 4.72 ± 0.69 | |||||
| Intervention group | 36 | Pre-intervention | 2.37 ± 0.54 | −22.989 | <0.001 | |
| Post-intervention | 6.35 ± 0.81 | |||||
| Difference between groups pre-treatment | 0.83 ± 0.53 | 0.892 | 0.376 | |||
| Difference between groups post-treatmen | 1.63 ± 1.03 | 9.201 | <0.001 | |||
| STED (mm) | Control group | 36 | Pre-intervention | 6.03 ± 1.00 | 8.572 | 0.047 |
| Post-intervention | 4.58 ± 0.59 | |||||
| Intervention group | 36 | Pre-intervention | 6.04 ± 0.91 | 10.425 | <0.001 | |
| Post-intervention | 3.54 ± 0.55 | |||||
| Difference between groups pre-treatment | 1.17 ± 0.84 | 0.055 | 0.956 | |||
| Difference between groups post-treatment | 1.04 ± 0.30 | 7.725 | <0.001 |
| Variable | Category | Control group ( | Intervention group ( | ||
|---|---|---|---|---|---|
| Pump-controlled blood flow rate achievement | Achieved | 34 | 36 | – | 0.507 |
| Not achieved | 2 | 0 | |||
| Puncture success rate per needle | Success | 216 | 216 | 17.926 | < 0.001 |
| Failure | 51 | 15 |
| Group |
| Test | |||
|---|---|---|---|---|---|
| Control group | 36 | Post-intervention | 230.25 ± 17.81 | ||
| Intervention group | 36 | Post-intervention | 257.06 ± 19.42 | ||
| Difference between groups post-treatment | 29.53 ± 23.25 | 6.103 | <0.001 | ||
| Variable | Group |
| Test | |||
|---|---|---|---|---|---|---|
| Physical health (score) | Control group | 36 | Pre-intervention | 56.36 ± 10.23 | −4.480 | <0.001 |
| Post-intervention | 65.58 ± 9.03 | |||||
| Intervention group | 36 | Pre-intervention | 55.51 ± 9.50 | −7.764 | <0.001 | |
| Post-intervention | 73.09 ± 10.39 | |||||
| Difference between groups pre-treatment | 9.50 ± 7.65 | 0.361 | 0.719 | |||
| Difference between groups post-treatment | 12.11 ± 7.77 | −3.250 | 0.002 | |||
| Mental health (score) | Control group | 36 | Pre-intervention | 49.89 ± 9.57 | −4.943 | <0.001 |
| Post-intervention | 57.86 ± 7.56 | |||||
| Intervention group | 36 | Pre-intervention | 51.66 ± 8.88 | −8.936 | <0.001 | |
| Post-intervention | 69.89 ± 10.40 | |||||
| Difference between groups pre-treatment | 11.81 ± 8.52 | −0.807 | 0.423 | |||
| Difference between groups post-treatment | 13.94 ± 10.63 | −5.584 | <0.001 | |||
| Impact of kidney disease (score) | Control group | 36 | Pre-intervention | 48.61 ± 7.30 | −10.940 | <0.001 |
| Post-intervention | 68.03 ± 9.39 | |||||
| Intervention group | 36 | Pre-intervention | 47.80 ± 5.47 | −15.048 | <0.001 | |
| Post-intervention | 74.06 ± 10.34 | |||||
| Difference between groups pre-treatment | 5.97 ± 4.39 | 0.529 | 0.599 | |||
| Difference between groups post-treatment | 12.61 ± 8.86 | −2.574 | 0.012 | |||
| Kidney burden (score) | Control group | 36 | Pre-intervention | 52.00 ± 6.31 | −8.899 | <0.001 |
| Post-intervention | 64.47 ± 6.29 | −16.820 | <0.001 | |||
| Intervention group | 36 | Pre-intervention | 49.26 ± 5.84 | |||
| Post-intervention | 77.11 ± 8.85 | |||||
| Difference between groups pre-treatment | 5.22 ± 3.94 | 1.900 | 0.062 | |||
| Difference between groups post-treatment | 13.14 ± 4.70 | −6.953 | <0.001 | |||
| Symptoms and discomfort (score) | Control group | 36 | Pre-intervention | 55.17 ± 7.41 | −7.037 | <0.001 |
| Post-intervention | 67.92 ± 8.77 | −11.205 | <0.001 | |||
| Intervention group | 36 | Pre-intervention | 55.11 ± 8.50 | |||
| Post-intervention | 76.71 ± 9.00 | |||||
| Difference between groups pre-treatment | 8.08 ± 6.67 | 0.028 | 0.978 | |||
| Difference between groups post-treatment | 9.31 ± 1.92 | −4.173 | <0.001 |
- —Department of Health of Hebei Province10.13039/501100008240
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Dialysis and Renal Disease Management · Diagnosis and Treatment of Venous Diseases
Introduction
1
Maintenance Hemodialysis (MHD) is the primary treatment modality for patients with end-stage renal disease (ESRD) (1). Arteriovenous Fistula (AVF), as the preferred vascular access (2), directly affects both dialysis efficacy and the quality of life of patients (3). After AVF creation, it must mature sufficiently to be used for dialysis puncture. Poor AVF maturation often leads to the inability to perform dialysis on time or inadequate dialysis, placing a significant burden on MHD patients (4, 5). Studies have shown that 28%–53% of AVFs fail to mature clinically, rendering them unable to meet the dialysis needs, necessitating effective and scientific interventions to promote AVF maturation (6). Previous studies have indicated that upper limb muscle strength and coordination, through their “pumping” effect, can optimize hemodynamic changes, improve vascular elasticity, and promote AVF maturation and stability (7). As early as 2013, Salimi F (8) suggested that the intensity of exercise after AVF surgery should gradually increase, with the use of resistance bands, dumbbells, and other equipment to assist training. MO Y and colleagues (9) attempted to use dumbbells in promoting AVF maturation exercises, which showed certain positive effects. However, in practice, patients often exhibited poor adherence due to the monotony of the exercises. Satoh M et al. (10) demonstrated that music could stimulate the desire for exercise, providing motivation and making it easier for participants to persist.
Previous studies have demonstrated that dumbbell exercises alone can positively promote the maturation of AVF, while music-assisted interventions are effective in enhancing patients’ exercise motivation and adherence. However, in clinical practice, these approaches are often implemented in isolation and lack a coherent theoretical framework to support long-term behavioral change. In addition, repetitive and monotonous exercise patterns may induce fatigue, thereby reducing patient engagement and sustainability.
Despite the demonstrated physiological benefits of exercise-based interventions, sustained engagement in postoperative AVF rehabilitation remains challenging, particularly during the early maturation period. Effective AVF exercise programs therefore require not only appropriate physical loading, but also a structured approach to support patients in translating initial intentions into consistent, long-term exercise behavior.
To address these limitations, the present study systematically integrates rhythmic music with dumbbell exercise and, for the first time, introduces the Multi-Process Action Control (M-PAC) framework as the core management strategy. The M-PAC framework focuses on the transition from intention to action and emphasizes multiple regulatory mechanisms across different behavioral phases (11). Guided by this framework, rhythmic music was employed to enhance the enjoyment and coordination of exercise, while an individualized, progressive dumbbell-loading protocol was developed. More importantly, a structured patient management and support system was established based on the reflective, regulatory, and reflexive processes of the M-PAC framework, aiming to ensure the safe, sustainable, and effective implementation of the exercise intervention. The process and results are reported as follows.
Materials and methods
2
General information
2.1
A total of 72 patients who underwent arteriovenous fistula (AVF) creation and stable regular hemodialysis at the Blood Purification Center of Cangzhou Central Hospital between January and April 2025 were selected as the study subjects. A random number sequence was generated by an external member of the research team using the Research Randomizer website (https://www.randomizer.org/), and the numbers were placed into opaque, sealed, and consecutively coded envelopes to assign the participants into a control group and an intervention group, with 36 patients in each group (Figure 1). Group assignments were concealed in sequentially numbered, opaque, sealed envelopes. These envelopes were opened only after the participants completed baseline assessments, by a research nurse who was unaware of the sequence. Baseline characteristics between the two groups were compared to ensure balance, and no significant differences were found.
CONSORT flow diagram.
The sample size was estimated based on pilot data and clinical experience. Assuming a moderate effect size (Cohen's d ≈ 0.7), a two-sided significance level (α) of 0.05, and a power of 80%, the required sample size was calculated using the formula: n = 2(Z_1−α/2_ + Z_1−β_)^2^/d^2^
This yielded an estimated sample size of approximately 32 participants per group. Considering a potential 10% dropout rate, the final sample size was set at 36 participants per group, totaling 72 participants.
Diagnostic Criteria: The patients met the criteria for dialysis access establishment as outlined in the “Dialysis Access China Guidelines (2024 edition)” published by the Chinese Society of Nephrology (12). Specifically, dialysis access should be planned when the estimated glomerular filtration rate (eGFR) is between 15 and 30 mL·min^−1^·(1.7 3m^2^)^−1^ or when clinical symptoms are significant and conservative treatment is insufficient.
Inclusion Criteria:
-
(1)Age ≥ 18 years;
-
(2)Surgical creation of AVF at the radial artery and cephalic vein in the forearm wrist area;
-
(3)First-time creation of AVF;
-
(4)No history of psychiatric disorders, language, or hearing impairments. Exclusion Criteria:
-
(1)History of AVF creation;
-
(2)Presence of limb movement disorders or other issues preventing dumbbell exercises;
-
(3)Severe comorbid conditions, such as heart disease or malignant tumors. Exclusion and Dropout Criteria:
-
(1)Development of complications such as AVF occlusion during the intervention period;
-
(2)Failure to complete follow-up examinations or assessments;
-
(3)Voluntary withdrawal by the patient. This study has been approved by the Ethics Committee of Cangzhou Central Hospital (Ethics Approval No. 2024-262-01). All patients provided informed consent and voluntarily participated in the study.
Methods
2.2
Both groups received routine postoperative management following AVF creation. The control group performed grip ball exercises for rehabilitation, while the intervention group engaged in rhythmic dumbbell rehabilitation exercises based on the M-PAC (Multi-Process Action Control) theory. The total duration of the intervention was 3 months.
Control group
2.2.1
Routine postoperative management was provided. Preoperatively, patients were educated on protecting the AVF side limb. Postoperatively, patients were instructed on methods to alleviate swelling and pain, as well as wound exudation and pain management. Dressings were changed every 2–3 days, and patients were informed not to have blood drawn from or rest on the AVF side limb during sleep. After suture removal, patients performed grip ball rehabilitation exercises on the surgical side arm. A medium-hardness, 7–7.5 cm diameter dialysis-specific grip ball was used. Patients were instructed to grip the ball firmly until the finger joints were maximally flexed, holding for 5 s, then completely relaxing for 5 s. This exercise was performed for 15 min per session, three times daily.
Intervention group
2.2.2
(1)Personalized Dumbbell Selection: Dumbbell selection strictly followed the core principle of “avoiding heavy lifting with the AVF-side arm.” Previous research has indicated that a 6-pound weight is the threshold for red muscle fiber activation (13). For safety and effectiveness, a 6-pound dumbbell was initially selected for the first week of exercise. After one week, grip strength on the AVF side was measured weekly using a hand dynamometer. Based on the patient's dynamic grip strength, the dumbbell weight was adjusted. Referring to the study by Zhang Jialong and colleagues (14), the maximum dumbbell weight was set to no more than 30% of the patient's grip strength test result.(2)Personalized Rhythmic Selection: Previous research (15) has indicated that the appropriate rhythm range for asynchronous music use in physical exercise is 120–140 beats per minute (bpm), with the music tempo ideally matching the rhythm of the exercise. Therefore, this study selected music with a tempo of 130 bpm, of a type that the patient found personally comfortable. The aim was to make the exercise more rhythmic, improving the patient's coordination and sense of rhythm. The exercise followed the music's rhythm: lifting during one beat and resting during the next, aligning the exercise rhythm with the music rhythm. Music Library and Selection Criteria: This study utilized a standardized music library curated by the researchers. All musical pieces had a tempo of 130 beats per minute and primarily included genres such as light popular piano music, Chinese traditional instrumental music, and light music integrated with natural sounds. Personalized Selection Process: During the intervention, patients selected the type of music they most preferred and found most comfortable. Music Delivery and Application: The music was played through the patient's own smartphone and was continuously played throughout the rhythmic dumbbell rehabilitation exercise session. The use of headphones was recommended to minimize external distraction.(3)Exercise Method: The patient should be seated with the AVF-side upper arm naturally hanging by the side of the body, with a slight flexion at the elbow and the wrist in a neutral position. Holding the dumbbell with the palm facing the body, the movement should only occur at the shoulder joint, swinging the arm forward. The arm should be imagined as a pendulum. The initial range of motion should be small, 15–30 degrees, avoiding raising the arm above the shoulder or excessive abduction. As the patient adapts and their capability improves, the range may be gradually increased to 45 degrees, provided there is no discomfort or weakening of the AVF bruit. The maximum range should not exceed 60 degrees. Exercises should be performed three times a day for 10 min each time.(4)M-PAC Multi-Process Action Control Exercise Management:
Reflection Process: Before the intervention, the benefits and necessity of the rehabilitation exercise were explained to the patients using simple language, addressing “Why do this?” (to protect the fistula and improve function), “What can I do?” (ability), “Is it convenient?” (opportunity), and “Can I make it a habit?” (automaticity). Clear explanations were provided on the selection of dumbbell weight and range limitations, ensuring that patients understood that this was a tailored and safe plan.
Regulation Process: The patient was involved in selecting personalized dumbbells and music rhythm, and a daily exercise plan was created. Patients were instructed to set up a convenient exercise corner at home, with a stable chair, accessible dumbbells, and a music-playing device. Family members/caregivers were encouraged to understand the plan and assist in the early stages by supervising posture, reminding the patient of exercise times, and offering positive encouragement.
Reflection Process: Monthly follow-up visits were conducted, during which feedback on the rhythmic dumbbell exercises was gathered. A physical examination and ultrasound were performed on the AVF-side arm to check for any adverse events. Patients were asked about any difficulties or challenges they encountered during the exercise process, and they were encouraged to continue their efforts.
Observation indicators
2.3
The following indicators were compared between the two groups before and after the intervention.
Physiological maturation of AVF
2.3.1
According to the “Expert Consensus on Vascular Access for Hemodialysis in China (2nd Edition)” (16), the criteria for determining physiological maturation of AVF are: natural blood flow in the AVF puncture segment >500 mL/min, venous diameter ≥5 mm, and a skin-to-vessel distance (STED) of less than 6 mm. In this study, ultrasound measurements were used to assess blood flow in the cephalic vein 5 cm above the puncture site, as well as vessel diameter and the distance from the vessel to the skin (17).
Clinical maturation of AVF
2.3.2
According to the definition of insufficient blood flow in the “Expert Consensus on Vascular Access for Hemodialysis in China (2nd Edition)” (16), if the pump-controlled blood flow during dialysis is less than 200 mL/min, the clinical maturation of the AVF is considered inadequate. This study evaluated the pump-controlled blood flow rate, the percentage of patients meeting the target pump-controlled blood flow rate, and the success rate of the first puncture within one week after the initial puncture at the end of the 3-month intervention.
Ultrasound assessments and puncture success evaluations were conducted by staff who were blinded to group allocation to minimize observer bias.
Quality of life
2.3.3
The Chinese version of the Kidney Disease Quality of Life Short Form (KDQOL-SFTM) (18) was used to assess quality of life. This scale includes five dimensions: physical health, mental health, impact of kidney disease, kidney burden, and symptoms and discomfort. Each dimension is scored from 0 to 100, with higher scores indicating better quality of life. The Cronbach's α coefficient for the total scale was 0.902.
Statistical analysis
2.4
Statistical analysis was performed using SPSS version 26.0. Categorical data were expressed as frequencies, and the comparison between groups was conducted using the chi-square (χ^2^) test. The Levene test was used to assess the homogeneity of variances, and continuous data that met the normal distribution were expressed as mean ± standard deviation ( ± s). Within-group comparisons were performed using paired t-tests, while between-group comparisons were conducted using independent t-tests. A significance level of α = 0.05 was adopted.
Results
3
Comparison of the general conditions of patients in the two groups
3.1
The patients were randomly assigned into the control group (n = 36) and the intervention group (n = 36) using a random number table. No significant differences were observed between the two groups in terms of age, gender, stage of kidney disease, or primary etiology of the disease (P > 0.05). See Table 1.
Physiological maturation of AVF
3.2
Due to weak, fluctuating, or intermittent cephalic vein signals before AVF creation, it was technically difficult to obtain reliable blood flow measurements using Doppler ultrasound. Therefore, preoperative flow data were not included in the analysis. This limitation occurred at a similar frequency in both groups and is unlikely to affect baseline comparability. Before the creation, there were no significant differences between the two groups in terms of vessel diameter and distance from the skin (P > 0.05). After the intervention, both groups showed significant increases in cephalic vein blood flow and vessel diameter, and a significant decrease in the STED (P < 0.05). The changes in the intervention group were significantly higher than those in the control group (P < 0.05) See Table 2.
Clinical maturation of AVF
3.3
Three months after AVF creation, in the control group, 2 patients had pump-controlled blood flow rates lower than 200 mL/min, resulting in a clinical maturation rate of 94.44%. In the intervention group, all patients had pump-controlled blood flow rates greater than 200 mL/min, with a clinical maturation rate of 100%. Although the intervention group had a higher maturation rate than the control group, no statistically significant difference was found between the two groups (P > 0.05), as shown in Table 3. Regarding the specific values of pump-controlled blood flow, the intervention group was significantly higher than the control group (P < 0.05), as shown in Table 4.
After the regular AVF puncture began, all patients underwent dialysis three times a week, with at least two needles per dialysis session. The control group had a total of 267 punctures, with 51 failures and 216 successes. The intervention group had a total of 231 punctures, with 216 successes and 15 failures. The success rate of puncture per needle in the intervention group was significantly higher than that in the control group (P < 0.05), as shown in Table 3.
Quality of life
3.4
In the present study, the Cronbach's α coefficient for the overall scale was 0.92, while the coefficients for each subscale ranged from 0.76 to 0.89. Before the intervention, there were no significant differences in the quality of life between the two groups (P > 0.05). After the intervention, the quality of life in the control group showed no significant change, while the intervention group showed improvement. The quality of life in the intervention group was significantly better than that in the control group (P < 0.05). Inter-group comparisons revealed that after the intervention, patients in the intervention group scored significantly higher than those in the control group across all five domains (Physical Health: t = −3.250, P = 0.002; Mental Health: t = −5.584, P < 0.001; Impact of Kidney Disease: t = −2.574, P = 0.012; Kidney Burden: t = −6.953, P < 0.001; Symptoms and Discomfort: t = 4.173, P < 0.001). Specifically, the physical health score in the intervention group (73.09 ± 10.39) was approximately 7.5 points higher than that in the control group (65.58 ± 9.03), with the most pronounced advantage observed in the mental health domain (69.89 ± 10.40 vs. 57.86 ± 7.56). See Table 5.
Discussion
4
Arteriovenous fistula (AVF) has long been considered the lifeline for patients on maintenance hemodialysis (MHD), with its proper function playing a critical role in ensuring adequate dialysis for these patients (19–21). The Dialysis Access China Guidelines (2024) (12) recommend that post-AVF creation rehabilitation exercises contribute to the stable maturation of the fistula. The European Society for Vascular Surgery (2018) (22) and the European Renal Best Practice (2019) (23) guidelines similarly emphasize adequate vessel diameter, sufficient blood flow, and superficial vein depth as key determinants of functional AVF maturation and successful cannulation. However, there is no consensus on the specific types of exercises and management methods for such rehabilitation (24–26). In this study, we made exploratory improvements based on routine AVF rehabilitation exercises by combining rhythmic music with dumbbell exercises as an intervention, and applied the M-PAC theory to ensure the continuous and effective implementation of the exercises.
The results of this study indicate that rhythmic dumbbell rehabilitation exercises based on the M-PAC theory can promote the maturation of AVF. The “China Dialysis Access Expert Consensus (2nd Edition)” (16) states that after AVF creation, puncture cannot be immediately performed, and a maturation period of 4–12 weeks is required. During this period, vascular reconstruction occurs, blood flow increases, and the vessel wall thickens and becomes more superficial. For physiological maturation, the natural blood flow in the puncture segment must be greater than 500 mL/min, the venous diameter should be ≥5 mm, and the depth from the skin must be less than 6 mm. However, physiological maturation does not necessarily equate to clinical usability. Clinical maturation is defined as achieving a pump-controlled blood flow rate of 200 mL/min or higher after the patient begins dialysis, and should also be considered in conjunction with the actual puncture conditions.
In this study, rhythmic dumbbell rehabilitation exercises, under the management of the M-PAC theory, were applied during the AVF maturation period, leading to significant increases in cephalic vein blood flow and venous diameter, as well as a reduction in the depth from the skin. These physiological maturation indicators showed notable improvement. Although the pump-controlled blood flow rate achievement did not show significant differences, the actual pump-controlled blood flow values in clinical use significantly improved, and the success rate of puncture per needle also showed significant improvement. These clinical maturation indicators suggest that rhythmic dumbbell rehabilitation exercises based on the M-PAC theory have clear effects.
Previous studies have attempted various methods of functional exercise to promote AVF maturation (27–29), including some research involving dumbbell exercises (30–32). However, these studies often lacked theoretical support and struggled with effective management in clinical practice. Additionally, the monotonous nature of the exercises led to increased patient fatigue and poor adherence. In contrast, this study utilized the M-PAC multi-process control theory as the management basis, providing stage-specific and targeted interventions for patients, ensuring the effectiveness of the rehabilitation exercises. Furthermore, the individualized rhythmic music enhanced the appeal of dumbbell exercises, making them more acceptable to patients. The selection of dumbbell weight based on grip strength ensured the safety and effectiveness of the exercises, thereby promoting AVF maturation.
The results of this study also demonstrate that rhythmic dumbbell rehabilitation exercises based on the M-PAC theory can effectively improve the quality of life in AVF patients. Prior to AVF creation, patients were troubled by disease symptoms and psychological anxiety, leading to a significant decline in quality of life. After AVF creation, with a clear treatment path and better control of disease symptoms, patients experienced some improvement in quality of life. Zhao Zhongqiu et al. (33) found that music-based exercise could improve patients’ anxiety and depression, which is consistent with the results of this study. Rhythmic dumbbell exercises improved patients’ psychological status to some extent, positively influencing their quality of life. Furthermore, the M-PAC theory management process allowed patients to experience a rigorous and scientific hospital management process, which also had a positive effect on improving their quality of life.
In this study, the pump-controlled blood flow rate did not show a significant difference (P > 0.05). Several factors may explain this result: First, the primary outcome in this study was blood flow measured by ultrasound. The sample size calculated for a “rate” outcome based on this data was relatively small, which could have led to a false negative result due to insufficient sample size. Second, previous literature (34) has pointed out that when AVFs experience complications such as stenosis or thrombosis, ultrasound shows significant changes in blood flow, but the pump-controlled blood flow and dialysis adequacy may not immediately reflect these changes. This suggests that pump-controlled blood flow can only serve as an auxiliary reference when monitoring AVF function, and ultrasound results may provide a more timely and reliable assessment.
Conclusion
5
Rhythmic dumbbell exercises based on the M-PAC theory are beneficial for promoting the physiological and clinical maturation of AVF in MHD patients, as well as improving their quality of life. These exercises have potential for wider application.
Limitation
6
There are certain limitations in this study. This was a single-center study with an insufficient sample size. Additionally, the follow-up period could be extended to further investigate the impact of this rehabilitation exercise on long-term complications related to AVF. We acknowledge that several potential confounding factors—such as blood pressure, diabetes, vascular calcification, surgeon variability, antiplatelet use, and needling technique—may influence AVF maturation and puncture outcomes. However, these variables were not comprehensively collected or adjusted for in this study. This represents a limitation and may affect the interpretation of the intervention effect. Future studies should consider stratifying or adjusting for these confounders to ensure more accurate assessment of causality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alghamdi LS Alonazi W. The utilization of renal dialysis: a comprehensive study in Saudi Arabia. BMC Public Health. (2024) 24(1):1914. 10.1186/s 12889-024-19450-539014360 PMC 11253410 · doi ↗ · pubmed ↗
- 2Lee J Lee S Chang JW Kim SW Song JK. Clinical value of intraoperative flow measurements of brachiocephalic arteriovenous fistulas for hemodialysis. Korean J Thorac Cardiovasc Surg. (2020) 53(3):121–6. 10.5090/kjtcs.2020.53.3.12132551292 PMC 7287223 · doi ↗ · pubmed ↗
- 3Lok CE Huber TS Lee T Shenoy S Yevzlin AS Abreo K KDOQI clinical practice guideline for vascular access: 2019 update. Am J Kidney Dis. (2020) 75(4 Suppl 2):S 1–S 164. 10.1053/j.ajkd.2021.02.00232778223 · doi ↗ · pubmed ↗
- 4Northrup H He Y Berceli S Cheung AK Shiu YT. Arteriovenous fistula histology, hemodynamics, and wall mechanics: a case report of successful and failed access in a single patient. Kidney Med. (2024) 6(4):100801. 10.1016/j.xkme.2024.10080138562969 PMC 10982562 · doi ↗ · pubmed ↗
- 5Wang P Chen H. Research progress on the factors influencing poor maturation of autologous arteriovenous fistula. Chin J Nephrol. (2023) 23(7):585–9. 10.3969/j.issn.1671-2390.2023.07.009 · doi ↗
- 6Nousis A Tziastoudi M Oustampasidou N Efthymiadi M Divani M Eleftheriadis T Epidemiology of vascular access in patients undergoing chronic hemodialysis treatment in Greece. J Clin Med. (2025) 14(13):4571. 10.3390/jcm 1413457140648941 PMC 12249874 · doi ↗ · pubmed ↗
- 7Khattri RB Kim K Anderson EM Fazzone B Harland KC Hu Q Metabolomic profiling reveals muscle metabolic changes following iliac arteriovenous fistula creation in mice. Am J Physiol Renal Physiol. (2022) 323(5):F 577–89. 10.1152/ajprenal.00156.202236007889 PMC 9602894 · doi ↗ · pubmed ↗
- 8Salimi F Majd Nassiri G Moradi M Keshavarzian A Farajzadegan Z Saleki M Assessment of effects of upper extremity exercise with arm tourniquet on maturity of arteriovenous fistula in hemodialysis patients. J Vasc Access. (2013) 14(3):239–44. 10.5301/jva.500012323283645 · doi ↗ · pubmed ↗